The Clinical Applications of Mitomycin C in Urologic Diseases: A Review Article
- 1. Professor in Pediatric Urology, Kermanshah University of Medical Sciences, Iran
- 2. Urology Resident in Kermanshah University of Medical Sciences, Iran
Abstract
Introduction: MMC is an antibiotic which through complex mechanisms prevent DNA synthesis and results in cell death subsequently. The first approved urological application of MMC was to treat bladder carcinoma in 1974. Since that time many studies have offered different utilization of MMC in urology. The efficacy, safety and long-term results of MMC has been shown in urological conditions however the majority of studies have concentrated on bladder cancer.
Methods: We searched the PubMed and Cochrane data bases by using the “ Mitomycin C” and “urological applications” as search keys, limiting search to systematic reviews from 2010 till 2016 in English language.
Results: Overall 20 articles were according to our inclusion criteria thus we reviewed them and represented all their relevant results.
Conclusion: The application of MMC in urology is more commonly in bladder cancer while for ureteropelvicial carcinoma and uretheral stricture is used too.
Keywords
• Mitomycin C
• Urology
• Bladder cancer
• Urethra
Citation
Moradi M, Rezaee H, Kaseb K (2017) The Clinical Applications of Mitomycin C in Urologic Diseases: A Review Article. J Drug Des Res 4(3): 1040.
INTRODUCTION
Mitomycin-C (MMC) is an antitumor antibiotic which the first time discovered by Japanese microbiologist through fermentation cultures of the Streptomyces caespitosus in 1950s [1]. This alkylating agent damage DNA cross-links that inhibit the DNA replication mechanism [2]. Mitomycin is active in all phases of the cell cycle, and is the best available drug for use in combination with radiation therapy to attack hypoxic tumor cells [3]. Its main clinical use is in the treatment of the anus squamous cell cancer in combination with 5-FU and radiation therapy. Also, it is used in combination with chemotherapy for squamous cell carcinoma of the cervix and gastric, breast, and pancreatic cancer [3]. Of the special utilization of mitomycin has been in treatment of superficial bladder cancer intravesically. Because virtually none of the agent is absorbed systemically, there is little to no systemic toxicity when used in this setting [3].
The first urological application of MMC was by shida and colleagues in 1976 [4]. The molecular weight of it is 334.3 kDa and is soluble in water and organic solvents and due to its hydrophilic nature and high molecular weight usually absorbed minimally [5]. The adverse effect of MMC in systematic use has been categorized into 3 groups in the Medscape medical software, more than 10% frequent are hemolytic uremic syndrome, myelosupression, nausea/vomiting and fever. One to 10 % frequent are stomatitis, increased serum creatinine and etc. The myelosuppresion has been the most frequent adverse effect by 64%.
METHOD
We searched the PubMed and Cochrane data bases by using the “ Mitomycin C” and “urological applications” as search keys, limiting search to full text systematic reviews from 2010 till 2016 in English language.
RESULT
Seventeen out of 20 of articles were about the MMC role in managing bladder cancer and the others were about upper urinary tract urothelial carcinoma and MMC effect on this cancer. Albeit MMC has different urological applications such as prevention of urethral stricture recurrence but in the mentioned time to the knowledge we have no systematic review has been done in such fields thus we used original articles.
DISCUSSION
MMC has been utilized for curing and managing different medical conditions for example in ophthalmology disease in order to preventing scar formation, docryocystorhinostomy and debridement therapy post keratectomy [6]. In otolaryngology disease usually due to anti fibrotic properties of MMC it’s used specially in decreasing the scaring/restenosis of the airway [7].
In the gastrointestinal carcinoma for the first time MMC used in combination with 5-FU in 1974 and nowadays it is as the standard treatment for types of cancers [8]. For dermal diseases mostly in order to prevent or treatment of keloid scar formation MMC has been applied [9].
Schematic Diagram of different theraputical applications of MMC
The urological applications of MMC are abstracted here and can be categorized as follow:
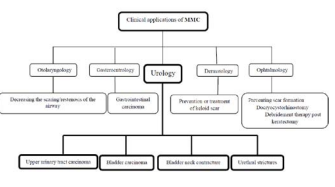
Upper urinary tract carcinoma
The MMC has been used for upper urinary tract transitional cell carcinomas through different forms of instillation as via nephrostomy, topical or retrograde by ureteroscopy [10,11]. In a recent study application of MMC (40 mg dissolved in 40 ml of 0.9% normal saline and instilled via an infusion pump over 40 minutes (1 ml/minute)) following laser ablation resulted in significant tumor recurrence decrease [12]. The adjuvant management of patients after kidney-sparing surgery is also evolving toward that used in patients with NMIBC, but Overall, the role of immunotherapy and chemotherapy for upper urinary tract transitional cell carcinomas is not firmly established [13,14].
Bladder carcinoma
Up to know the majority studies have been limited to urothelial cancers in which bladder cancer is the common one that during the years one instillation per week for 6 weeks intravesically has been scientifically popular [15,16]. Bladder cancer is one of the most common noncutaneous malignancies specially in men in which the most common presentation of these patients is painless hematuria, and transurethral resection of bladder tumor (TURBT) is as the cornerstone intervention in these patients. MMC and BCG (Bacillus Calmette-Guerin) therapies have been for many years the interventions which resulted in significant theraputical conclusions [17-24]. In the recent studies it has been shown that a single dose of intravesical chemotherapy as MMC within 24 hours following TUR of non-muscle-invasive bladder tumor (NMIBT) resulted in a 13% absolute reduction in tumor recurrence through prevention of cancerous cell implantation mechanism [25]. It is very important not to use this agent when the perforation of the bladder wall is suspected, and this must be noticed that despite the ability of BCG the Mitomycin-C can’t prevent tumor progression and it is effective on recurrence only, however in recent studies it has been suggested that the combination therapy of MMC with Gemcitabine maybe through autophagy induction of cancer stem cells (CSC) regulate the relapse of urothelial tumors [26]. Currently MMC is used in 40mg in 20 ml vials for intravesical chemotherapy although it has 5mg, 20mg, 40mg powders for injection [27]. The MMC also for Many of patients experience disease recurrence after BCG failure is the recommended treatment [28-32]. In recent different clinical application of Mitomycin it has been used as Hyperthermic Mitomycin (HM) which is heated through various manner in the bladder and it has been shown that this form of intravesical chemotherapy can result in increase of disease free survival rate and maybe 59% reduction of NMIBC recurrence [33].
Bladder neck contracture
The other application of MMC in urology is to prevent the bladder neck contracture after incision while it has been studied through injection of 0.3 to 0.4 mg/ml mitomycin C at each incision site and the results advocated its efficacy [32] but in another vast study the efficacy of MMC injection was lower than previous and deducted that maybe its usage accompany with serious adverse effects [34].
Urethral strictures
The other urological complications in which due to their frequent occurrence after transurethral resection of the prostate, urethral catheterization, cystoscopy, prostatectomy, pelvic trauma, prostate radiation therapy, hypospadias repair, urethritis, and lichen sclerosus many steps has been done to prevention [35]. In a very recent and interesting study the efficacy of using intralesional MMC (injections of 0.4-mg/mL MMC in 0.2- to 0.4- mL aliquots at various points along the length of each incision for a total volume of 10 mL) with clean intermittent catheterization (CIC) and visual internal Urethrotomy (VIU) for management of recurrent urethral strictures and bladder neck contractures studied and finally offered all of these interventions provides minimally invasive and widely available tools for managing urethral strictures less than 3 cm and bladder neck contractures specially for patients who are poor candidates for open surgery [36].
We have used in our experience MMC as intraurethral hydrogel (0.8 mg MMC and 1 cc mixture of distilled water and propylene glycol in a 40/60 relation were added to it), in order to prevent post-traumatic anterior urethral stricture recurrence after internal urethrotomy and it was significantly effective [37].
CONCLUSION
Despite different theraputical applications of MMC, in urology it has nearly bounded utilizations in which bladder carcinoma has been anciently the most common filed. It is worthful to use MMC in upper urinary tract carcinomas, bladder neck contractures and urethral strictures too but should have in mind that the results of studies sometimes are disappointing.









































































































































