Huge Branchial Parotid Cyst: A Case Report and Review of the Literature
- 1. Department of ENT and CCF, Hassan II University Hospital, Morocco
ABSTRACT
Intraparotid branchial cysts are rare and poorly understood congenital malformations of the first branchial cleft. They are characterized by 3 types of manifestations that can be associated or isolated: inflammatory swelling of the subauricular and inferior parotid region with or without cervical skin fistula and a fistula of the floor of the external auditory canal with or without otorrhea, with or without premyringal flange on otoscopy. Ultrasound and magnetic resonance imaging (MRI) may be necessary, especially in parotid forms, to determine the cystic nature of the swelling. From a therapeutic point of view, surgical removal remains the ideal option. We report the case of a patient with a huge branchial cyst of right parotid location.
KEYWORDS
• Branchial system
• Intra parotid cyst
• Surgery
CITATION
Adoua Y, Oudidi A, Alami MN (2023) Huge Branchial Parotid Cyst: A Case Report and Review of the Literature. J Ear Nose Throat Disord 7(1): 1049.
INTRODUCTION
Parotid branchial cysts are rare dyssembryological malformations with auriculo-branchial expression. They are due to a defect of migration and coalescence of the embryonic buds of the first branchial cleft.
MATERIAL AND METHODS
We report the case of a 42-year-old patient referred to the ENT department of the Hassan II Hospital University in Fez for treatment of a swelling of the parotid region evolving slowly since young age marked by episodes of superinfection and fluctuating increase in volume. The clinical examination revealed a swelling of the right parotid region, 10 cm in length, painless, soft, and mobile to the two planes with a healthy skin aspect (Figure 1).

Figure 1 Clinical photo showing a right cystic parotid mass
Examination of the oral cavity and oropharynx did not reveal any parapharyngeal bulge. The otoscopic examination did not reveal any fistula in the floor of the external auditory canal. The patient had no trismus or facial paralysis. The cervical lymph nodes were free. The rest of the otorhinolaryngological and somatic examination was normal. The patient underwent a cervical ultrasound which showed a cystic formation at the expense of the right parotid gland with a 10 cm long axis. A parotid MRI was ordered, showed a well-limited formation of the right parotid gland with a low T1 and high T2 signal with thin, invisible walls, which became thickened and enhanced by contrast injection (PDC) (Figure 2).
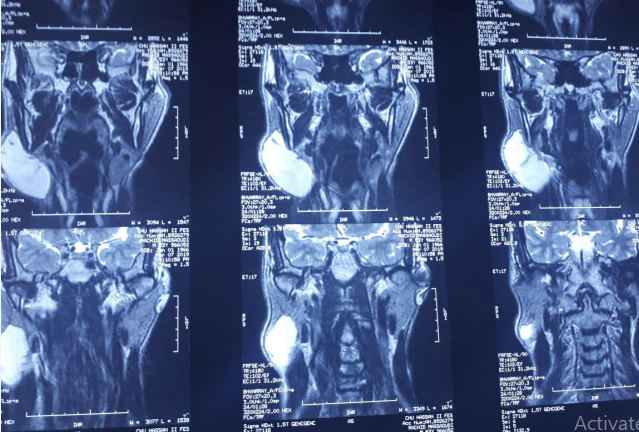
Figure 2 Parotid MRI coronal section showing a branchial cyst located in the right parotid
The patient underwent exo-facial parotidectomy. The postoperative course was simple. The final histological examination confirmed the embryonic branchial origin of the cyst. The evolution was favorable with no recurrence after 3 years.
DISCUSSION
Intraparotid cysts of branchial origin are malformative dysembryological cysts due to an abnormality in the docking of the ectodermal part of the first branchial arch responsible for the genesis of auriculobranchial cysts and fistulas. They represent between 1-8% of congenital anomalies of the first branchial arch and 1% of cervical anomalies [1]. Hunczowski described the first branchial cleft in 1789. Nevertheless, the first branchial cyst of the parotid gland was described by Hildebrandt in 1895. These malformations occur most frequently in children, before the age of five, and in adults in the third decade, with an average age of 44 years and a male-to-female ratio of 2:1 [2]. There are two anatomical types according to the relationship with the parotid gland and especially with the facial nerve according to Arnot’s classification in 1971:
Type I: considered a duplication of the membranous external auditory canal (EAC), the cyst is located in the retroauricular region, the fistulous path runs medially and anteriorly parallel to the EAC and passes outside the facial nerve to open into the bony portion of the EAC. Histological examination shows no skin appendage or cartilage residue, indicating an ectodermal origin.
Type II: more frequent than type I, the lesions associate a cyst of the lower part of the parotid region, an ascending fistulous pathway passing in the middle of the parotid gland indifferently inside or outside the facial nerve. The upper orifice is located at the osteo-cartilaginous junction of the EAC. The histology shows a differentiation with skin appendages and cartilage derivatives.
Clinical examination usually reveals a painless, soft, fluctuating swelling of variable size, usually from 0.5 cm to 5 cm in diameter, most often located in the superficial lobe of the parotid gland, especially in its lower part. The external orifice of the fistula is located in the triangle of Poncet and the internal orifice is located on the floor of the CAE, the path of the fistula is parallel to the CAE, apart from episodes of superinfection which are often revealing, these lesions often go unnoticed. Cysts develop in the parotid gland or in the lymph nodes of the parotid gland and are radiologically specific in the absence of a fistula [3,4]. Imaging examinations are of great diagnostic value, ultrasound coupled with Doppler, is a low cost examination, requested in first intention, it allows the positive diagnosis, the location and the cystic nature; it allows to guide a fine needle puncture, it generally reveals a rounded formation, with anechoic content with posterior reinforcement, well limited, with non-existent or very thin wall without tissue vegetation in the non-abscessive forms. Doppler allows to identify the vascular components of a mass and to specify its relationship with the vessels of the neck. However, it does not allow exploration of deep structures. MRI remains the examination of choice, it shows an oval or round cyst of the parotid gland, the parotid cavity or the parapharyngeal space, and also to specify the cystic nature of the swelling, and to appreciate its extension and its relationships, they have a low signal in T1 and high in T2. Their walls are thin, but may be thickened and enhanced by injection of PDC when the cyst is superinfected.
The differential diagnosis is represented by other lesions with a cystic component, such as cystic adenoid carcinoma (hypo signal T1, variable signal T2), malignant necrotic adenopathies, lymphangioma, lymphoepithelial cyst (HIV); thus any cystic formation of homogeneous density, parotid or juxta-parotid, should evoke a cyst of the 1st branchial cleft. From a therapeutic point of view, surgical removal is systematically indicated because of the infectious complications. It should be performed as soon as possible to limit the risks of inflammatory remodeling related to episodes of superinfection, and surgery should then be performed only after cooling with appropriate antibiotic therapy, the intimacy of the relations of the cysts of the first cleft with the facial nerve imposes a parotidectomy approach with a resection of the fistulous orifice, the fistula is then dissected from one side to the other by discovering its relations with the facial nerve, if it exists, the internal orifice will be resected with ablation of a cartilaginous fragment of the floor of the external auditory canal [4]. In the absence of treatment, cysts evolve towards superinfection, fistulization to the skin, cervical compression syndrome, neoplastic degeneration is extremely rare [3,5], nevertheless, iatrogenic complications are dominated by facial nerve and carotid injury and recurrence [5]
CONCLUSION
The cysts of the first branchial arch of parotid localization are rare dyssembryological malformations; due to a defect of closure of the first branchial cleft, their diagnosis is sometimes difficult. The treatment is always surgical and should be performed at a distance from infectious episodes. Post-operative complications are mainly represented by recurrence and facial paralysis.
REFERENCES
- Janka JakubÍkova, Roman StanÍk, Alena StanÍkova. Malformations of the first branchial cleft: duplication of the external auditory canal (case report). Int J Pediatr Otorhinolaryngol. 2005; 69: 255–61.
- Nisreen A, Imtiaz MQ. First branchial cleft fistula: a presentation on two cases and review of literature. Glob J Oto. 2017; 6: 555680.
- Gleizal A, Merrot O, Fagahati S, Beziat JL. [Surgery for cysts and fistulas of the face and neck]. EMC Techniques chirurgicales Chirurgie plastique reconstructrice et esthétique. 2011: 1–15.
- Benchemam Y, Bénateau H, Laraba C, Alix T, Assaf R, Labbé D, et al. Kystes de la première fente branchiale: à propos d´un cas. Revue de Stomatologie et de Chirurgie Maxillo-Faciale. 2002; 03: 379–383.
- Fernandez-Pineda I, Hernandez-Guisado JM, Gracia A, de Agustin JC. First branchial cleft fistula: a case report. International Journal of Pediatric Otorhinolaryngology Extra. 2008; 3: 174–176.








































































































































{kind=link}