Sudden Hearing Loss: When Is Hyperbaric Oxygen Indicated
- 1. Centro de Medicina Subacuática e Hiperbárica das Forças Armadas Portuguesas; Department of Otorhinolaryngology of Hospital das Forças Armadas; Department of Otorhinolaryngology of Cuf Descobertas Hospital Lisbon, Portugal
- 2. Department of Sciences and Technologies, Autonoma University of Lisbon, Portugal
- 3. Unitat de Terapêutica Hiperbárica Barcelona; Universitat de Barcelona, Portugal
ABSTRACT
Objective: The aim of this study is to evaluate the efficiency of Hyperbaric oxygen therapy (HBOT) in idiopathic sudden sensorineural hearing loss (ISSHL) and to define the factors related to the ISSHL that most improve with HBOT such as: onset of HBOT, hearing severity, audiometric shape and related symptoms (vertigo and tinnitus). Methods: Retrospective review of the clinical data of 394 patients treated with HBOT with the diagnosis of ISSHL in one single hyperbaric unit from 2005 to 2009. Audiograms from before and after HBOT were examined. Age, time onset of disease, hearing loss severity, audiometric shape, and related symptoms were reviewed. Recovery according to Siegel criteria was noted. Results: In 291 patients (73,8%) HBOT was started within 8 weeks of onset, while 87 (22%) HBOT was started after 8 weeks of ISSNL. 107 patients (27%) had cophosis and 190 (48%) had moderated hearing loss. The most frequent audiometric shape was the type E with 118 patients, followed by 79 patients with Type B. There was hearing recovery in 280 (71%) patients. According to Siegel’s classification, 113 (29%) patients had total recovery, 74 (19%) had partial recovery, 77 (19%) light recovery and 130 (33%) had no recovery Conclusion: Hyperbaric Oxygen may be beneficial in patients mainly with cophosis and within 8 weeks of disease onsite. Prospective, multicenter studies
CITATION
Amaro CE, Radu L, Desola J (2023) Sudden Hearing Loss: When Is Hyperbaric Oxygen Indicated. J Ear Nose Throat Disord 7(1): 1052.
INTRODUCTION
Idiopatic sudden sensorineural hearing loss (ISSHL) is an ear nose throat emergency [1] and is defined as a hearing loss of 30 dB or more over at least three contiguous frequencies, over a period of 72 hours or less, without an identifiable cause [2]. ISSHL has an annual incidence of 5 to 27 cases per 100000 inhabitants and it is believed that it is underestimated [3]. Though it can occur at any age, ISSHL affects mainly patients in 5th or 6th decade [4]. Most ISSHL are unilateral with only 2% of bilateral hearing loss [5,6]. Tinnitus and vertigo can be concomitant symptoms [5-11].
SSHL has a high spontaneous recovery rate in the first two weeks with some studies reporting a rate from 32 to 70% [7]. Some prognostic factors for spontaneous recovery have been identified, creating the acronym HEAR [5,8,4,9]:
- Hearing-cophosis and very severe hearing loss have the worse prognosis;
- Elapsed time of hearing loss;
- Audiometric shape-type C and E audiometric shape are likely those who have less recovery (Figure 1);
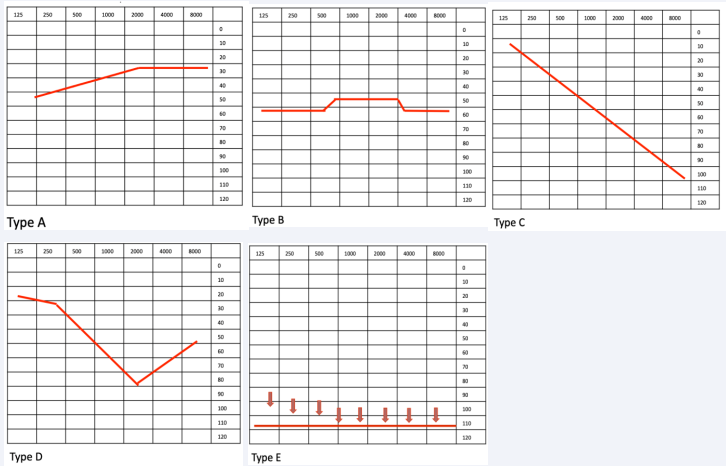
Figure 1 Audiometric shape.
- Related symptoms, such as tinnitus and vertigo.
Though its spontaneous recovery, it is recommended ISSHL treatment with systemic high dose corticosteroid therapy [10-12] in the first 2 weeks of disease onset [13]. It is also recommended intratympanic corticosteroid as first line therapy or savage therapy [11,14-17].
According to European Committee for Hyperbaric Medicine (ECHM) and Undersea and Hyperbaric Medical Society (UHMS), Hyperbaric oxygen therapy (HBOT) is defined as exposure of humans in hyperbaric treatment devices (hyperbaric chambers) up to 2.0 bar overpressure (equal to 20 meters depth of water) with the breathing of oxygen [18]. In the Tenth European Committee on Hyperbaric Medicine, HBOT is a type 1 recommendation in the treatment of ISSHL within two weeks of disease onset, being reasonable to use HBOT as an adjunct to corticosteroids therapy in patients presenting after the first two weeks of disease onset but not later than one month, particularly, in patients with severe and profound hearing loss [19]. In the most recent clinical practice guideline published by the American Academy of Otolaryngology Head and Neck Surgery Foundation, the initial therapy with HBOT within 2 weeks of onset of ISSHL is optional and salvage therapy with HBOT combined steroid therapy as salvage within 1 month of onset is also optional [13].
Aim of the study
The aim of this study is to evaluate the efficiency of HBOT in ISSHL and to define the factors related to the ISSHL that most improve with HBOT such as: onset of HBOT, hearing severity, audiometric shape and related symptoms (vertigo and tinnitus).
METHODS
After institutional review board approval, the data was retrospectively collected from the medical reports of patients seen in our institution (Centro de Medicina Subacuática e Hiperbárica das Forças Armadas) with ISSHL diagnosis between 2006 to 2009. All patients received corticosteroid therapy before being sent to our institution and they had to complete at least 10 sessions of HBOT and have the pre and post-treatment audiograms available.
From 2005 to 2009 our institution received 670 patients with ISSNL. From these, 276 were excluded and 394 patients were included in the study. Patients were excluded because:
1. the cause for hearing loss was identified such as: Cogan syndrome, sonotrauma, multiple sclerosis, labyrinthine hemorrhage (detected in magnetic resonance),labyrinthitis after middle ear infection, recent treatment with cisplatin and interferon (because of hepatitis C), otosclerosis, inner ear barotrauma;
2. had contraindications for HBOT: severe emphysema, uncontrolled epilepsy
3. Pre or pos audiometric testing was missing.
Pure tone average (PTA) was calculated as the arithmetic mean of thresholds at 0.5, 1, 2 and 4 kHz. Classification of hearing loss [20] was divided in: light (21 to 40 dB); moderate (41 to 70 dB); severe (71 to 90 dB); very severe (91 to 110 dB); cophosis (120 dB).
The audiometric shape was classified in Type A, B, C, D or E (Figure 1). HBOT protocol involved breathing 100% oxygen at 2.5 absolute atmospheres (ATA) inside a hyperbaric, multiplace 1st class chamber for 70 minutes with additional 15 min for recompression until reaching 2.5 ATA and 15 minutes for decompression back to surface. Sessions were one per day and patients had to perform a total of 10 to 20 sessions.
Hearing improvement was evaluated comparing audiometric PTA pre and pos HBOT. The response to therapy was categorized according to Siegel’s criteria [21]:
I. Healing: final threshold more than 25 dB.
II. Partial improvement: gain of more than 15 dB, final hearing threshold 25-45 dB.
III. Slight improvement: gain of more than 15 dB, final hearing threshold more than 45 dB.
IV. No response: gain of less than 15 dB and final hearing threshold more than 75 dB.
A recovery greater than 15 dB when comparing PTA pre and pos HBOT was considered as being responsive to treatment [22,23].
Statistical analysis
All statistical analyses were performed using the software system Phyton version 3.7.3. The Kruskall-Wallis [24] test was used to compare several independent groups at the same time. When it was statistically significant, the post hoc Dunn test [25] was applied. A p value of less than 0.05 was considered to be statistically significant.
RESULTS
From 2005 to 2009 our institution received 670 patients with ISSNL. From these, 276 were excluded and 394 patients were included in the study.
The median age at diagnosis was 49,7 years (range 10-86 years). 53% were male and 47% female. 276 (70%) patients had tinnitus and 169 (43%) had vertigo.
The medium time for treatment was within 6 weeks of disease onset. 126 (31.9%) HBOT was initiated within 2 weeks of disease onset. HBOT was started within 2 to 8 weeks of onset in 165 (41,9%). Therefore, in 291 patients (73,8%) HBOT was started within 8 weeks of onset, while 87 (22%) HBOT was started after 8 weeks of ISSNL. There was no information about elapsed time in 16 patients.
107 patients (27%) had cophosis and 190 (48%) had moderated hearing loss. The most frequent audiometric shape was the type E with 118 patients, followed by 79 patients with Type B. Most patients completed 20 HBOT sessions (65%), while only 32% completed 10 OHBT sessions.
Table 1, 2,3 resume some results of our study.
Hearing recovery
There was hearing recovery in 280 (71%) patients, and 114 (29%) had no recovery.
According to Siegel’s classification, 113 (29%) patients had total recovery, 74 (19%) had partial recovery, 77 (19%) light recovery and 130 (33%) had no recovery [Table 4].
Age (p=0.557), tinnitus (p=0.5896) and vertigo (p=0.5313) had no influence in hearing recovery. However, female patients had less probability of hearing recovery and it was statistically significant (p=0.047).
Initiating HBOT as soon as possible is an important prognostic factor and it was statistically significant (p<0.01). Patients starting HBOT within 8 weeks of ISSNL onset were those who had more hearing recovery (Figure 2).
Moreover, the sooner HBOT was started, the bigger was the absolute difference between pre and post PTA and it was statistically significant (p<0.01) (Figure 3).
The audiometric shape also influenced hearing recovery. Patients had more recovery if the shape was type E (p<0.01) (Figure 4).
Patients with cophosis had the best hearing recovery rate (p<0.01) being considered a good prognostic factor (Figure 5).
When correlating gender with age and audiometric shape, females with type A have less recovery than male patients while older female with type D stand out comparing to the other groups (Figure 6). However, each of these groups don’t have enough cases to elaborate a statistic study that could provide some conclusion.
DISCUSSION
Most studies reveal that association of precocious HBOT to medical therapy have better results in ISSHL than medical treatment alone [26-28]. Both the American Academy of Otolaryngology Head and Neck Surgery Foundation and the ECHM don’t recommend starting HBOT after one month of disease onset, even as a salvage therapy [19,13]. Actually, in the most of the published studies HBOT was started within 2-3 weeks of disease onset [27,29-31].
Khater and his co-workers showed a recovery rate of 72.7% in a study when HBOT was associated to medical treatment in the 1st week of disease onset [26].
In a retrospective study with 334 patients with ISSHL treated with intravenous corticosteroid therapy and 10 sessions of HBOT [27], there was a 69.2% of success. Those who received HBOT within the 7 days of onset had a recovery rate of 82.2% while there was just a 19% of recovery rate in patients who received HBOT 22 days after the onset of ISSHL.
In this study, all patients treated with HBOT had previously received corticosteroid therapy and it was still possible to see some hearing recovery in at least 71% of the cases. Doses and type of corticoid were not consistent among patients: some received deflazacort, others prednisolone or betamethasone, some received oral treatment, some received intramuscular treatment, and doses differed. It was not possible to have some corticoid treatment standardization. The earlier HBOT started (less than 8 weeks), the more recovery was seen in patients (p<0.01). Moreover, initiating HBOT precociously improved the PTA gain between pre and post treatment (p<0.01). Since most of the patients of this study started after 2 weeks of disease onset (66,6% of the patients), one must conclude that considering spontaneous recovery as the explanation for hearing improving is not applied in these cases. Moreover, this study showed that it is still possible to have some hearing recovery within 8 weeks of disease onset, thus making it possible to extend the acceptable period to start HBOT (more than one month).
As already reported by other works [30], patients in our study with cophosis and/or audiometric shape type E are those with better prognostic value in hearing recovery when patients receive HBOT (p<0.01). Surprisingly, female patients had worse prognosis than male, though a p=0.047 is actually very close to statistically significance. The authors of this study can’t find a reasonable explanation for this result. Age, tinnitus and vertigo had no influence in recovery.
CONCLUSION
Though its limitation for being retrospective, this study revealed that HBOT as an adjuvant treatment can improve hearing recovery not only as 1st line treatment but also as salvage treatment. Even when HBOT is started after 1 month of onset of disease, one can achieve good recoveries rates. Cophosis and type E audiometric shape are the best responders to HBOT and vertigo and tinnitus had no influence. The authors recommend a prospective, multicenter study comprising a greater number of patients.
ACKNOWLEDGEMENT
The authors would like to thank all the patients and the team of the hyperbaric unit for providing all the necessary data to build this work.
Ethics Declaration
This study was approved by the Hospital das Forças Armadas ethics committee and by Barcelona’s University ethics committee in 30.07.2021. This article is based on a preliminary study that was presented as a project in the Master in Underwater and Hyperbaric Medicine that CRIS-UTH organizes for the University of Barcelona.
REFERENCES
5. Byl FJ. Sudden hearing loss: eight years´experience and suggested prognostic table. Laryngosocpe. 1984; 94: 647-661.
11. Metrailer A, Babu SC. Management of sudden sensorineural hearing loss. Curr Opin Otolaryngol Head Neck Surg. 2016; 24: 403-406.
20. Recommandation biap 02/1 bis. Biap org. 1997.
24. on-line. [Online]. Available from: https://scikit-posthocs.readthedocs. io/en/latest/generated/scikit_posthocs.posthoc_dunn/.
25. on-line. [Online]. Available from: https://scikit-posthocs.readthedocs. io/en/latest/generated/scikit_posthocs.posthoc_dunn/.








































































































































{kind=link}