The Impact of Menopause on Diabetic Retinopathy
- 1. Department of Diabetes Ministry of Health and Medical Education, Iran
- 2. Department of Endocrinology, Tehran University of Medical Sciences, Iran
Abstract
Background: The disease due to the disturbances in glucose, lipid and protein metabolisms which is the most prevalent disease of our times is known as diabetes. This multifactorial disease is more common in females of post menopause period because of different risk factors like higher age and body mass index (BMI).
Participants and Methods: The study was conducted on 1315 patients with type II diabetes referred to the Diabetes Clinic of Imam Khomeini hospital, in Tehran, Iran, in 2014. Sampling 534female patients aging from 30 up to 70, and with clinical history of 1up to 20 years of type II diabetes, and also with urinary albumin excretion of 30 up to 300mg per 24 hours, was carried out and then divided into pre-menopause and menopause groups. With controlled blood pressure, all these patients were under retinopathy assessment by an ophthalmologist. Lipid profile, BMI and HbA1c were also were also measured and the results using SPSS (version 19) were then analyzed.
Results: According to the evidences, micro-albuminuria was a common complication of type II diabetes, and there was a direct interrelation between micro-albuminuria and retinopathy. The study demonstrated micro-albuminuria increased in the menopause group, where menopause alone had no effect on retinopathy. In fact, the effective factors in association with micro-albuminuria and retinopathy in the menopause group were urinary albumin excretion (UAE), HbA1c, BMI and age and in the pre-menopause group were HbA1c, HDL, TG and age. Finally, since micro-albuminuria is a risk factor for retinopathy, and also micro-albuminuria is influenced by hormones, thus, hormone therapy seems to be helpful in controlling micro-albuminuria and thereby reducing retinopathy.
Conclusion: It was concluded that retinopathy did not increase with menopause. In fact, glycemic factors seemed to have the maximum impact on retinopathy. In order to reduce micro-albuminuria and thereby retinopathy, it is therefore suggested to have a greater control over hyperglycemia.
Keywords
• Menopause
• Retinopathy
• Pre-menopause
• Diabetes
Citation
Ghaemi F, Nakhjavani M, Esteghamati A (2016) The Impact of Menopause on Diabetic Retinopathy. J Endocrinol Diabetes Obes 4(2): 1088.
BACKGROUND
Diabetes is a metabolic disease characterized by a disturbance in glucose, lipid and protein metabolisms [1]. At present, it is known as the most common epidemic disease and therefore one of the most considerable social, economic, and health problems in the world [2]. According to WHO’s records, the population of diabetic patients across the world will increase from 171 million people in 2000 to 489million in 2030 [3]. One research has predicted that in 2025, more than 75 percent of diabetic patients will be found in developing countries [4]. Presently, there are about 4 millions of diabetic patients living in Iran, and this number will increase on the average of half a million per year. Other studies of retinopathy conducted in 2001 estimated the number of diabetic patients to be 1 millionin Iran. Based on the predictions of WHO, the number of people suffering from type II diabetes in ,may reach up to 5125000 [5].
Diabetes carries with it the threat of micro-vascular and macro-vascular problems and result in lower life expectancy [6,7]. Complications such as micro-albuminuria and retinopathy are common in diabetic patients and they can be prevented with early treatment and a healthy life style [8]. Despite the recent advances in controlling diabetes, these complications still persist, for instance, micro-albuminuria is reported to have an incidence of 30-50 percent in patients suffering from type II diabetes [9]. Moreover, the incidence of end stage renal disease (ESRD) has increased within the past two decades in type II diabetic patients [10].
Other important ophthalmic complications of diabetes are macular edema and premature cataract [11]. Compared to normal individuals, diabetic patients are 25 times more likely to go blind [12]. Statistics indicated that diabetic retinopathy is the most common chronic complication of diabetes and accounts for adult blindness in America in the ages ranging from20 to 74 [13,14]. The onset and severity of diabetic retinopathy is closely associated with the duration of diabetes [15]. Neuropathy, nephropathy and cardiovascular events are also reported as complications of diabetes mellitus [16].
Diabetes is also believed to be related to patient’s gender. Some studies have indicated that women are more susceptible to type II diabetes; especially in pregnancy and reproduction years because hormonal changes in these periods can affect blood glucose levels [17,18]. Weight is another risk factor associated with diabetes. Overweight women with type II diabetes may undergo menopause later than other diabetic female patients. It has been found that in overweight women the estrogen level decreases more slowly compared to underweight and normal weight women [19].
According to Rafati et al., [20], diabetic retinopathy in Iran has 26.6up to 56.8 percent prevalence and its range variation depends on the type of diabetes, the number of patients and the facilities of hospitals in specific community under study. There are several factors which can cause retinopathy. Vazirinasab et al., [21] studied diabetic patients in Tehran and concluded that retinopathy is correlated with risk factors such as Hb A1C, duration of diabetes, and systolic blood pressure. Furthermore, the progress of retinopathy is shown to be related to age, sex, high blood pressure and smoking [22], as well as the increase in lipid which damages retinal vessels [23].
Women with pan-retinopathy are reported to have higher percentage than men; however, retinopathy is still shown to be related to age, diabetes type, duration of the diabetes, and the recent control of blood sugar [24]. Montrasa et al., study [25] revealed that menopause does not enhance the risk of diabetes; premature menopause occurring below 45 years of age, however, can escalate the risk of non-insulin dependent diabetes mellitus (NIDDM).
The number of diabetic patients in Iran, specifically female diabetics is increasing, but public awareness of this disease, its complications such as retinopathy and nephropathy can contribute to its decrease. This suggests the necessity of public awareness, adequate prevention and treatment of diabetic patients, particularly females. The present paper thus examines the prevalence of retinopathy and its relation with menopause in diabetic women in an Iranian hospital.
METHOD
The case-control study in hand was conducted with a population of 1315 type II diabetic patients referring to the Diabetes Clinic of IK Hospital in Iran, in 2014. Through convenient sampling, 539 female patients aging from 30 up to 70 years were selected. All patients at the entry to the study had at least one year and at most 20 years of clinical history of diabetes. A test of micro-albuminuria was then performed. 197 out of 539 patients i.e. (36.5%) whose urinary albumin excretion was 30 to 300 mg/24 hours were selected as the subjects of this research.
In this study menopause is defined as the absence of menstruation or twelve consecutive months and is used as a criterion to categorize the subjects. The pre-menopause group (including 45 patients, i.e.25%) was in the age range from 30 to 50 years and the menopause group (including 152 patients, i.e.75%) was 51 to 70 years of age. The mean duration of disease in the pre-menopause and menopause group was 5 and 8.4 years, respectively. After obtaining their consents, both groups were led to ophthalmologist to be checked for retinopathy. Para-clinic examinations of lipid profile, BMI, HbA1cand HTN were performed .Blood pressure of both groups was under control. The outlier cases were excluded from the study and the results were then analyzed with SPSS (Version 19)
RESULTS
Analysis of the collected data in SPSS was carried out in three phases. In the first phase, to examine the relationship between retinopathy and micro-albuminuria, the mean micro-albuminuria in both groups of under study was measured; the mean for the pre-menopause group was 64.85 mg/24 hours and for the menopause group it was 34.92 mg/24 hours (Table 1). Then a t-test was conducted –t (0.018) and p<0.05 – and the difference between the two groups had statistical significance (Table 1).
Table 1: Health characteristics of the patients.
| Variables | Pre-menopause | Post-menopause | ||||
| Mean±SEM | Maximum | Minimum | Mean±SEM | Maximum | Minimum | |
| Age | 46±.60 | 50 | 35 | 59±.49 | 70 | 51 |
| Urine Albumin Excretion | 34.92±3.50 | 110.00 | 1.00 | 64.85±5.41 | 300.00 | 1.00 |
| BMI | 29.93±.82 | 41.40 | 21.76 | 30.44±.37 | 47.94 | 20.83 |
| Duaration of DM | 5.0±.78 | 23.0 | .1 | 8.4±.51 | 30.0 | .2 |
| Hb AIC | 7.67±.24 | 13.60 | 4.90 | 8.02±.14 | 14.50 | 4.20 |
| HDL | 46.51±159 | 75.00 | 30.00 | 49.89±1.01 | 87.00 | 22.00 |
| LDL | 110.98±4.91 | 188.00 | 48.00 | 108.75±3.03 | 218.00 | 25.00 |
| TG | 191.89±19.12 | 900.00 | 65.00 | 188.74±11.55 | 1560.00 | 51.00 |
Another t-test was conducted to examine micro-albuminuria in both groups of patients – those with retinopathy (49.32) and those without retinopathy (34.7). The result was t value 0.032 and the p value was less than 0.05 (Table 2) which had statistical significance.
Table 2: Micro-albuminuria in the pre-menopause and menopause groups and in retinopathy and non-retinopathy groups.
| t-test for Equality of Means | |||
| Sig. (2-tailed) | Mean Difference | Sig. (2-tailed) | |
| ln_UAE | pre-menopause | -.46447 | .018 |
| menopause | |||
| retinopathy | -.40752 | .032 | |
| non-retinopathy | |||
In the second phase of the research, using logistic regression the impact of differing factors on the micro-albuminuria-retinopathy relationship was examined. These factors include HTN, BMI, Lipid (TG, HDL, LDL, Chol), Hb A1C.
In the pre-menopause group, HbA1c, HDL, TG and age proved to have an impact on micro-albuminuria-retinopathy relationship, whereas in the menopause group, UAE, HbA1c, BMI and TG were proved to have influence on the relationship (Table 3).
Table 3: Factors affecting micro-albuminuria-retinopathy relationship in pre-menopause and menopause group.
| pre-menopause group | Variable | Wald | Sig |
| Hb A1C | 8.263 | 0.004 | |
| HDL | 4.193 | 0.041 | |
| TG | 4.030 | 0.045 | |
| Age | 8.930 | 0.004 | |
| Constant | 8.663 | 0.003 | |
| menopause group | UAE | 3.307 | 0.045 |
| A1C | 6.347 | 0.012 | |
| BMI | 5.527 | 0.019 | |
| TG | 2.798 | 0.049 | |
| Constant | 0.033 | 0.855 |
It was shown that micro-albuminuria and retinopathy had a positive correlation; on the other hand, retinopathy and menopause were not correlated (Figure 1).
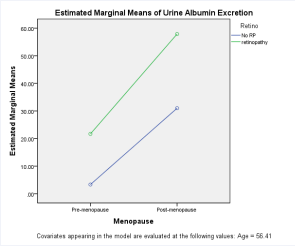
Figure 1 Micro-albuminuria in retinopathy and menopause.
However, in the third phase of the study, a Generalized Linear Model was used to adjust age and other factors, and the results revealed that HbA1c was the only factor affecting retinopathy and menopause (Table 4).
Table 4: The relationship between retinopathy and menopause.
| Dependent Variable: Urine Albumin Excretion | ||||||
| Source | Type III Sum of Squares | Df | Mean Square | F | Sig. | Partial Eta² |
| Corrected Model | 38295.325ª | 4 | 9573.831 | 2.753 | .029 | .054 |
| Intercept | 13278.692 | 1 | 13278.692 | 3.819 | .052 | .020 |
| Age | 5300.388 | 1 | 5300.388 | 1.524 | .218 | .008 |
| Menopause | 15080.093 | 1 | 15080.093 | 4.337 | .039 | .022 |
| Retino | 13101.768 | 1 | 13101.768 | 3.768 | .050 | .019 |
| Menopause * Retino | 466.493 | 1 | 466.493 | .134 | .715 | .001 |
| Error | 667627.755 | 192 | 3477.228 | |||
| Total | 895512.978 | 197 | ||||
| Corrected Total | 705923.080 | 196 | ||||
| a. R Squared = .054 (Adjusted R Squared = .035) | ||||||
DISCUSSION
The results suggested that micro-albuminuria is a common complication of diabetes type II, and this is in line with the findings of the study conducted byNakhjavani et al., [26] which found an association between micro-albuminuria and the long duration of diabetes, dyslipidemia and uncontrolled hyperglycemia. Nelaj et al., [27] conducted a similar research which revealed higher VMI, BMI, and a longer duration of diabetes in type II diabetes patients with micro-albuminuria compared to patients with type II diabetes without albuminuria.
Another result of this study was a positive correlation between micro-albuminuria and retinopathy which resembles the results obtained by Lunetta et al., [28] and Javadi [29]. Lunetta et al., focused on the nature of association between urinary albumin excretion (UAE) on the one hand and retinopathy, coronary heart disease (CHD), hypertension and triglycerides on the other. They conducted their study on 320 type II diabetic patients and concluded that increased UAE is associated with a greater prevalence of retinopathy and CHD in type II diabetic patients. Moreover, Javadi’s study showed that high prevalence of retinopathy was due to poor control and inadequate treatment of diabetes.
There were several studies examining the relationship between diabetes and menopause. For instance, Auryan and Itamar [30] found diabetes to be related to certain female-specific features like contraception and menopause. Also, Monterrosa-Castro et al., [31] explored the nature of association between diabetes and early menopause in women under 45 years of age. The outcome of their study was that menopause did not increase the risk of type II diabetes and therefore diabetes could be treated through hormone therapy [32]. In accord with these studies, the study in hand also revealed that diabetes is observed more often in menopause patients, which could be due to several factors including age and BMI. In fact, metabolic syndrome is observed more in menopause age range; refer to for instance the longitudinal research by Shai et al., [33] and the study by Ainy et al., [34]. The former argued that age and obesity affect diabetes in women. Another finding of their research was the relation between diabetes and ethnicity in women, and they demonstrated that Asians, Hispanics and black women have a greater risk of diabetes compared to white women. A similar study by Afzal and Mustehsan Bashir [35] attempted to examine the link between metabolic syndrome and menopause and their results indicated that metabolic syndrome had a higher prevalence in post-menopausal women compared to the pre-menopause group.
In Addition, the present study found out that in the menopause group of subjects micro-albuminuria increases; which resembles the findings of some other studies including Schopick et al., [36] and Roest et al., [37]. The former showed a clear relationship between the history of PMH for more than six years and a lower urinary ACR in non-diabetic women. The latter was a cohort study exploring the urinary albumin levels relation to cardiovascular mortality. The studies reported in [38], [39] and [40] too, have examined micro-albuminuria relation to menopause and have found a relationship between these two put emphasis on the usefulness of hormone therapy in order to decrease micro-albuminuria in menopause women.
Although micro-albuminuria, diabetes and metabolic syndrome increase in the menopause group, retinopathy (after age adjustment) was shown not to change with menopause. According to the findings of many studies such as Vérier-Mine et al., [41] the long-term impact of pregnancy on development and progress of microvascular complications in diabetes type II, first or the other pregnancy does not seem to be a risk factor for the long-term progress of any microvascular complication. As a matter of fact, retinopathy is intensified with puberty and pregnancy which illustrates the role of hormones in it.
The last finding of the present research concerns itself with hormone therapy. Certain studies have examined the efficacy of hormone therapy in treating diabetes. For instance, De Lauzon-Guillain et al., [42] found MHT to be associated with lower risk of new-onset diabetes. Gaspard and van den Brûle [43] came up with a similar result and these studies proved that diabetes control was impaired by hormone therapy. Palin et al., [44] carried through a questionnaire survey on the views of local practitioners and hospital doctors on HRT. The result was that a majority of doctors participating in the survey would recommend HRT to women, in particular to diabetic women, and their concern about the probable side-effects of such a treatment seemed not to deter them from prescribing HRT. The public opinion developed by NAMS lent credence to this finding [45].
Meanwhile, other studies have focused on the impact of hormone therapy on retinopathy; for instance, Grigsby et al., [46] provided evidence for the role played by sex hormones in the development and progression of diabetic retinopathy. At the same time, Yuen and Kahn [47], obtained a different result. They examined the association between age, gender and hormone. In diabetic patients older than 45 years of age, a risk of blindness was approximately equal for men and women. However, for patients under 45, diabetic males had a higher rate of diabetic blindness compared to females. These data were consistent with the hypothesis that the presence of female hormones improves the prognosis in diabetic retinopathy.
The present study revealed, on the one hand, that micro-albuminuria increases in the menopause group yet it was shown that menopause does not affect retinopathy on the other hand; thus, the main finding of this study indicates that since micro-albuminuria is a risk factor for retinopathy and micro-albuminuria is influenced by hormones and therefore, using hormone therapy can help with reducing micro-albuminuria and resulting in reduction of the risk of retinopathy.
CONCLUSION
This study was design to examine the factors affecting retinopathy. It illustrated that micro-albuminuria was a common complication of diabetes type II. The positive correlation between micro-albuminuria and retinopathy was shown to be different in the two groups of the study. In the pre-menopause group, Hb A1C, HDL, TG and age had impact on micro-albuminuria-retinopathy relationship, while in the menopause group, UAE, HbA1c, BMI and TG were shown to have influence on the relationship; where the only factor affecting retinopathy and menopause was proved to be HbA1c.Given the fact that hyperglycemia is the most significant factor influencing retinopathy, we should exert an intensive glycemic control in order to reducing micro-albuminuria and thereby controlling retinopathy.









































































































































