Impact of Yoga Practice in Hearing-Impaired and Mute Adolescents: Experimental Study
- 1. SVYASA Yoga University, India
Abstract
Adolescents with hearing impairments and mutism face unique challenges in emotional regulation and cognitive development due to communication barriers and social isolation. Conventional therapeutic and educational strategies may not fully address these issues, necessitating the exploration of alternative interventions. Yoga, recognized for its holistic benefits on mental and emotional well-being, offers a promising approach for enhancing cognitive and emotional functioning in this population. This study examines the effects of Integrative Approaches to Yoga Therapy (IAYT) on cognitive and emotional functioning in hearing-impaired and mute adolescents. Study consisted 60 participants (16–21 years) recruited from Oceanik College, Bengaluru, allocated them into a yoga group and a control group. Cognitive and emotional outcomes were assessed using the Digit Letter Substitution Test (DLST) and the Positive and Negative Affect Schedule (PANAS). The yoga group showed significant improvements in attention, processing speed, and emotional well-being (p < 0.001), while the control group showed minimal changes. This study highlights the potential of yoga-based interventions in education and therapy for this population and calls for further research on long-term benefits and broader applicability.
Keywords
• Yoga; Hearing Impairment
• Mutism
• Emotion Regulation
• Attention
Citation
Aladakatti JG, Singh J, Snigdha A, Babu N (2025) Impact of Yoga Practice in Hearing-Impaired and Mute Adolescents: Experimental Study. J Fract Sprains 4(1): 1011.
INTRODUCTION
The adolescent years are marked by significant psychological and cognitive changes, often posing emotional regulation challenges [1]. This period is especially complex for adolescents with hearing impairments or mutism, as they face additional communication barriers and social isolation, which may lead to heightened emotional distress and cognitive difficulties [2]. Effective emotional control is essential for social interaction and overall well being, yet hearing-impaired and mute adolescents may struggle more with these skills due to limited access to verbal communication and social learning experiences [3]. Cognitive development, including attention, memory, and executive functioning, can also be adversely affected by the sensory and communication deficits experienced by this population. The traditional educational and therapeutic approaches may not always adequately address these multifaceted challenges, necessitating alternative and integrative interventions [4].Integrative Approaches to Yoga Therapy (IAYT) has emerged as a promising intervention that targets both emotional and cognitive dimensions through mind-body practices [5]. IAYT combines physical postures, breathing exercises, and meditation techniques designed to enhance self-awareness, emotional regulation, and mental focus [6]. Studies have shown that yoga practices can activate the parasympathetic nervous system, reduce stress levels, and improve cognitive functions such as attention and memory [7]. For adolescents with hearing impairments and mutism, IAYT may provide a non-verbal therapeutic modality that can be easily adapted to their needs, offering a holistic method for developing emotional resilience and cognitive skills [8,9] concluded that 4 months regular practice of Yoga improves the subjective feeling of wellbeing and quality of life, he also founded that yoga helps in reducing state and trait anxiety and helps to improve the mental health [10] concluded that yoga helps in reducing pain associated disability and improves the mental health of the practitioners. [11] founded that 12 12-week yoga programme helps in improving the self-concept of school going children. Barso et al., suggests that yoga practice is beneficial in the enhancement of self-esteem in the prison population [12]. This research aims to explore the potential impact of IAYT on emotion regulation and attention enhancement, providing evidence for its application in hearing impaired and mute adolescents.
METHODOLOGY
The study involved deaf and mute adolescents from PUC-I to degree levels at Oceanik College, Bengaluru, allocated into either experimental and control groups. Inclusion criteria included absolute deafness, ages 16–21, and ability to participate in yoga and games. Exclusion criteria included severe physical or cognitive impairments, involvement in other physical training programs, recent surgeries, or unavailability during the four-week study. Ethical approval and informed consent were obtained (RES/IEC-SVYASA-ERC/371/2024). Verbal consent was obtained from the college principal, and participants provided informed consent, ensuring they were aware of the study’s purpose and their right to withdraw with prior notice.
Assessments
The study assessed cognitive and emotional outcomes using the Digit Letter Substitution Test (DLST) for attention and processing speed and the Positive and Negative Affect Schedule (PANAS) for emotional states. The Digit Letter Substitution Test (DLST) assesses attention, psychomotor speed, and cognitive flexibility through a timed task of matching digits with corresponding letters, with scoring based on accuracy and speed. It is reliable and valid for evaluating cognitive changes [13,14]. The Positive and Negative Affect Schedule (PANAS) measures emotional states across two dimensions: positive affect (PA), reflecting enthusiasm and energy, and negative affect (NA), indicating distress and negative emotions. Using a 10-item Likert scale for each dimension, PANAS has strong reliability and validity for assessing emotional well-being [15].
Intervention
The IAYT module was framed by referring [16] the module comprised of breathing exercises, Sukshma vyayama (loosening exercises) for warm up followed by 12 rounds of surya namaskar and selected asanas to improve attention. Relaxation technique (shavasana) and pranayama followed. The practices were conducted as a group session with sufficient space arrangements. Every practice was taught through demonstration by the researcher and instructions to the subjects about the yoga poses were given in the sign language with the help of interpreters. Control group followed daily regular routine (Table 1).
Table 1: Duration of intervention.
|
SL No |
Practice |
Duration (minutes) |
|
1 |
Prayer |
1min |
|
2 |
Breathing exercise |
5 min |
|
3 |
Loosening exercises |
10 min |
|
4 |
Surya Namaskar (12) Vrikshasana Ardhachakrasana Natarajasana Janu sirasasana |
18 min |
|
5 |
Savasana |
2 min |
|
6 |
Nadi Shodhana Pranayama |
5 min |
|
7 |
Bhramari |
3 min |
|
8 |
Closing prayer |
1 min |
Statistical analysis
Data were analyzed using IBM SPSS version 27 (IBM Corp., Armonk, NY). Descriptive statistics, including means and standard deviations for continuous variables and number percentages for categorical variables, were calculated to summarize participant characteristics. Independent t-tests were used to compare baseline differences between the Yoga and Control groups for continuous variables, while chi-square tests were used for categorical variables. To assess within-group changes from baseline to post intervention, paired t-tests were performed. Between group differences in post-intervention outcomes were examined using independent t-tests. Effect sizes were calculated using Cohen’s d, where values of 0.2, 0.5, and 0.8 were interpreted as small, medium, and large effects, respectively. Mean differences between groups were reported with 95% confidence intervals (CI) to assess the magnitude of intervention effects. A significance level of p < 0.05 was considered statistically significant for all analyses.
RESULTS
Flow of participants is given in Figure1.
Figure 1 Trial Profile.
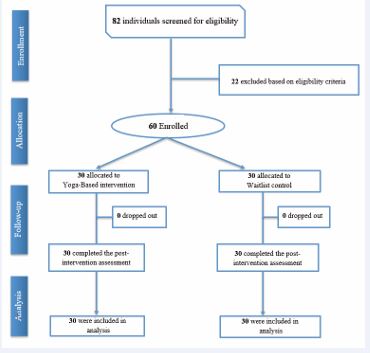
The study enrolled 60 participants through convenient sampling and assigned them to either the intervention (IAYT) group or the control group (n=30 each). No dropouts occurred, ensuring complete data collection. The demographic profile of the participants (Table 2)
Table 2: Demographic profile of participants.
|
Variable |
Overall (n=60) |
Yoga (n=30) |
Control (n=30) |
P-value |
|
Age, mean (SD) |
17.72 (0.99) |
17.63 (1.13) |
17.80 (0.85) |
0.520 |
|
Male, n (%) |
33 (55.01) |
19 (63.33) |
14 (46.67) |
0.194 |
|
DLST, mean (SD) |
32.58 (15.01) |
34.10 (13.53) |
31.07 (16.45) |
0.439 |
|
Positive affect, mean (SD) |
30.78 (5.82) |
29.67 (4.74) |
31.90 (6.62) |
0.139 |
|
Negative affect, mean (SD) |
32.47 (6.73) |
32.80 (6.59) |
32.13 (6.98) |
0.705 |
Data are presented as mean (SD) for continuous variables and n (%) for categorical variables. DLST: Digit Letter Substitution Test. P-values indicate comparisons between the yoga and control groups using independent t-tests for continuous variables and chi-square tests for categorical variables.
revealed a mean age of 17.72 years (SD=0.99), with the yoga group having a slightly lower mean age of 17.63 years (SD=1.13) compared to the control group with 17.80 years (SD=0.85), though this difference was not statistically significant (p=0.520). The overall sample consisted of 55.01% males, with a higher proportion in the yoga group (63.33%) compared to the control group (46.67%), but this difference was not significant (p=0.194). The DLST, positive affect, and negative affect scores showed slight variations between the yoga and control groups, but none of the differences were statistically significant (p > 0.05).
Study outcomes
Digit Letter Substitution Test (DLST) scores showed a significant improvement in the Yoga group, increasing from a baseline mean of 34.10 to 47.50 (p < 0.001), whereas the Control group exhibited a smaller increase from 31.07 to 35.67 (p = 0.04). The between-group comparison also showed a significant difference (p < 0.001). Similarly, positive affect scores improved significantly in the Yoga group, rising from 29.67 at baseline to 38.00 post intervention (p < 0.001), while the Control group showed no meaningful change (31.90 to 31.93, p = 0.931), with a significant between-group difference (p < 0.001). Negative affect scores decreased significantly in the Yoga group, from 32.80 to 22.27 (p < 0.001), whereas the Control group showed no significant change (32.13 to 32.23, p = 0.732), with a significant between-group difference (p < 0.001) (Table 3).
Table 3: Analysis of study variables.
|
Variable |
Group |
Mean baseline score |
Mean post intervention score |
P-value: Within group |
P-value: Between group |
|
DLST |
Yoga |
34.10 |
47.50 |
<0.001 |
<0.001 |
|
Control |
31.07 |
35.67 |
0.04 |
||
|
Positive affect |
Yoga |
29.67 |
38.00 |
<0.001 |
<0.001 |
|
Control |
31.90 |
31.93 |
0.931 |
||
|
Negative affect |
Yoga |
32.80 |
22.27 |
<0.001 |
<0.001 |
|
Control |
32.13 |
32.23 |
0.732 |
Mean baseline and post-intervention scores are reported for each group. Within- group p-values indicate changes over time using paired t-tests, while between-group p-values indicate comparisons between yoga and control groups using independent t-tests.
When analyzed for effect sizes, the Yoga group showed greater improvements across all variables compared to the Control group. For DLST, the mean change was 13.40 (SD = 9.65) in the Yoga group versus 4.60 (SD = 8.01) in the Control group, with a mean difference of 8.71 (95% CI: 4.01 to 13.42) and a large effect size (d = 1.01). Positive Affect improved significantly in the Yoga group (8.33, SD = 4.51) compared to the Control group (0.03, SD = 2.09), with a mean difference of 7.87 (95% CI: 6.08 to 9.66) and a very large effect (d = 2.36). Negative Affect decreased significantly in the Yoga group (-10.53, SD = 4.49) versus the Control group (0.10, SD = 1.58), with a mean difference of -10.35 (95% CI: -11.80 to -8.90) and a large effect (d = -3.20), highlighting the strong impact of Yoga on emotional well-being (Table 4).
Table 4: Effect sizes of study variables.
|
Variable |
Mean change scores (SD) |
Mean difference: Between group |
Cohen’s d |
|
|
Yoga |
Control |
|||
|
DLST |
13.40 (9.65) |
4.60 (8.01) |
8.71 (4.01 to 13.42) |
1.01 |
|
Positive affect |
8.33 (4.51) |
0.03 (2.09) |
7.87 (6.08 to 9.66) |
2.36 |
|
Negative affect |
-10.53 (4.49) |
0.10 (1.58) |
-10.35 (-11.80 to -8.90) |
-3.20 |
Mean change scores (SD) represent the average change from baseline to post- intervention, with standard deviation in parentheses. The mean difference (between-group) is calculated as the difference in mean change scores between the Yoga and Control groups, with 95% confidence intervals in parentheses. Cohen’s d represents the effect size.
DISCUSSION
The present study highlights that adolescent with hearing impairments and mutism participating in the Integrated Approach to Yoga Therapy (IAYT) experienced significant improvements in emotion regulation and cognitive functioning compared to a control group. The DLST scores increased significantly in the yoga group (mean change = 13.40 ± 9.65) with a between-group mean difference of 8.71 (95% CI: 4.01 to 13.42, p < 0.001). Positive affect improved significantly in the yoga group (8.33 ± 4.51) with a between-group difference of 7.87 (95% CI: 6.08 to 9.66, p < 0.001). Negative affect decreased substantially in the yoga group (-10.53 ± 4.49), with a between-group difference of -10.35 (95% CI: -11.80 to -8.90, p < 0.001). These findings highlight the significant benefits of yoga in enhancing cognitive function and emotional well-being. While the control group showed minor improvements, the intervention group demonstrated significantly better outcomes.This effect is particularly beneficial for hearing-impaired adolescents who frequently experience emotional distress due to their communication limitations [17]. These findings are consistent with previous research, which has shown that yoga interventions enhance emotional resilience and reduce stress-related symptoms in adolescents Gothe et al., Beyond emotional regulation, the study also found notable improvements in cognitive function, attention in the IAYT group compared to the control group. Adolescents with hearing impairments often experience cognitive delays due to reduced auditory input, which can hinder their language acquisition and academic performance [18]. The findings of this study align with previous research, which demonstrated that yoga interventions could significantly improve working memory, attention span, and cognitive flexibility in children with intellectual and sensory impairments [19]. Additionally, studies have also shown that regular yoga practice can improve executive functions such as task-switching, decision-making, and problem solving by strengthening the prefrontal cortex, which plays a crucial role in higher-order cognitive processes [20]. The mechanisms underlying these benefits can be attributed to yoga’s ability to regulate stress and enhance self-regulation. The combination of controlled breathing, meditation, and structured physical movement activates the parasympathetic nervous system, reducing cortisol levels and promoting relaxation [21-23]. The holistic nature of IAYT, which integrates physical movement, breathwork, and mindfulness, may explain its effectiveness. Unlike conventional therapies that focus on either physical or psychological aspects separately, IAYT addresses both, making it particularly suitable for individuals with sensory impairments who face challenges in processing emotional and cognitive stimuli [24]. Yoga’s emphasis on mindfulness, focused breathing, and movement-based concentration exercises has been shown to enhance cognitive functions by improving neural connectivity and promoting neuroplasticity [25]. Mindfulness and meditative practices enhance neural activity in the prefrontal cortex, improving executive functions such as attention, working memory, and impulse control [26,27]. Group yoga sessions would have increased social connectedness, helping adolescents feel more supported and integrated, which positively impacts their self-esteem and emotional well-being [28]. Together, these mechanisms would have contributed to enhanced cognitive and emotional resilience. The effect size analysis revealed substantial differences between the Yoga and Control groups across cognitive and emotional variables. Cohen’s d indicated a large effect for DLST (d = 1.01), suggesting that the Yoga intervention significantly enhanced cognitive performance. This is comparable to previous results on impact of yoga practice in attention among adolescents [29]. The effect on Positive Affect was even more pronounced (d = 2.36), reflecting a strong improvement in emotional well-being among participants in the Yoga group. Additionally, the large negative effect size for Negative Affect (d = -3.20) underscores the substantial reduction in negative emotions following Yoga practice. The results align with previous research supporting Yoga as a holistic approach to enhancing psychological resilience and cognitive efficiency [30-35]. These findings highlight the effectiveness of Yoga in improving both cognitive function and emotional regulation, with effect sizes far exceeding conventional thresholds for meaningful clinical impact. Overall, findings suggest that IAYT is a promising intervention for adolescents with hearing impairments and mutism, addressing both their emotional and cognitive needs. The non-verbal nature of yoga provides an accessible therapeutic tool, fostering emotional resilience and cognitive improvements through breath control, mindfulness, and movement. A key strength of this study is its holistic approach, which integrates multiple yoga techniques to address both emotional and cognitive well-being. However, limitations such as a small sample size, short intervention duration, reliance on subjective measures, and lack of comparative interventions should be addressed in future research. Expanding the study with larger, more diverse samples and incorporating objective neurophysiological assessments will further validate the long-term impact of yoga-based interventions in this population.
CONCLUSION
The study findings suggest that yoga is an effective intervention for improving cognitive function and emotional well-being. Participants in the yoga group demonstrated significant enhancements in attention and positive affect, along with a notable reduction in negative affect. These results highlight the potential of yoga as a complementary approach for cognitive and emotional enhancement, supporting its broader application in well being interventions.
REFERENCES
- Silvers JA. Adolescence as a pivotal period for emotion regulation development. Curr Opin Psychol. 2022; 44: 258-263.
- Wong P. Selective mutism: a review of etiology, comorbidities, and treatment. Psychiatry (Edgmont). 2010; 7: 23-31
- Yadav AK, Ahsan A, Kumar V. Impact of Hearing Aid Usage on Emotional and Social Skills in Persons With Severe to Profound Hearing Loss. J Audiol Otol. 2023; 27: 10-15.
- Romero-Ayuso D, Jorquera-Cabrera S, Segura-Fragoso A, Toledano- González A, Rodríguez-Martínez MC, Triviño-Juárez JM. Assessment of Sensory Processing and Executive Functions in Childhood: Development, Reliability, and Validity of the EPYFEI. Front Pediatr. 2018; 6: 71.
- Villacres Mdel C, Jagannathan A, Nagarathna R, Ramakrsihna J. Decoding the integrated approach to yoga therapy: Qualitative evidence based conceptual framework. Int J Yoga. 2014; 7: 22-31.
- Sengupta P. Health Impacts of Yoga and Pranayama: A State-of-the- Art Review. Int J Prev Med. 2012; 3: 444-458.
- Khajuria A, Kumar A, Joshi D, Kumaran SS. Reducing Stress with Yoga: A Systematic Review Based on Multimodal Biosignals. Int J Yoga. 2023; 16: 156-170.
- Radhakrishna S. Application of integrated yoga therapy to increase imitation skills in children with autism spectrum disorder. Int J of Yoga. 2020; 3: 26-30.
- Gururaja D, Harano K, Toyotake I, Kobayashi H. Effect of yoga on mental health: Comparative study between young and senior subjects in Japan. Int J of Yoga. 2020; 4: 7-12.
- Büssing A, Michalsen A, Khalsa SBS, Telles S, Sherman KJ. Effects of yoga on mental and physical health: a short summary of reviews. Evid-Based Complement and Alternat Med. 2012; 2012: 165410.
- Marciniak R, Sheardova K, ?ermáková P, Hude?ek D, Šumec R, HortJ. Effect of meditation on cognitive functions in context of aging and neurodegenerative diseases. Front in Behav Neurosci. 2014; 8: 17.
- Bartos LJ, Meek GA, Berger BG. Effectiveness of Yoga versus Exercise for Reducing Falling Risk in Older Adults: Physical and Psychological Indices. Percent Mot Skills. 2022; 129: 1245-1269.
- Pradhan B, Nagendra H. Normative data for the digit–letter substitution task in school children. Int J of Yoga. 2009; 2: 69.
- Salthouse TA. What do adult age differences in the Digit Symbol Substitution Test reflect? J of Gerontol. 1992; 47: P121-P128.
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J of Pers and Soc Psychol. 1988; 54: 1063-1070.
- Naduvanthody S, Subramanya P, Shitha P, Sayana PS. Effect of Structured Yoga Program on Functional Balance, Flexibility, and Emotional Status in Students with Bilateral Sensorineural Hearing Impairment. J of Applied Consciousness Studies. 2022; 10: 77-83.
- Stephens M, Hemingway M. Teaching yoga : essential foundations and techniques. 2010; 411.
- Kirk MA, Taha B, Dang K, McCague HP, Hatzinakos D, Katz J, et al. A Web-Based Cognitive Behavioral Therapy, Mindfulness Meditation, and Yoga Intervention for Posttraumatic Stress Disorder: Single-Arm Experimental Clinical Trial. JMIR Ment Health. 2022; 9: E26479.
- Mohanty S, Pradhan B, Hankey A. Yoga Practices as an Alternative Training for Physical Fitness in Children With Visual Impairment. Adapt Phys Activ Q. 2019; 36: 431-446.
- Jayantilal PK, Kashyap A. The Role of Yoga in Enhancing Decision Making: A Research Perspective. J of Ayurveda and Integr Med Sci. 2024; 9: 177-183.
- Gathercole SE, Alloway TP, Kirkwood HJ, Elliott JG, Holmes J, Hilton KA. Attentional and executive function behaviours in children with poor working memory. Learning and Individual Differences. 2008; 18: 214-223.
- Hart J. An overview of clinical applications of therapeutic yoga. Alternat and Complement Ther. 2008; 14: 29-32.
- Vancampfort D, Vansteelandt K, Scheewe T, Probst M, Knapen J, De Herdt A, et al. Yoga in schizophrenia: a systematic review of randomised controlled trials. Acta Psychiatr Scand. 2012; 126: 12-20.
- Amonkar N, Wan-Chun Su, Bhat AN, Srinivasan SM. Effects of Creative Movement Therapies on Social Communication, Behavioral-Affective, Sensorimotor, Cognitive, and Functional Participation Skills of Individuals with Autism Spectrum Disorder: A Systematic Review. Front in Psychiatry. 2021; 12: 722874.
- Srinivasan M, Ravi M. Effect of Yogic Practice and Saq Training on Selected Coordinative Abilities of Students with Hearing Impairment. Am J of Art and Design. 2017; 1: 15-20.
- Tang G, Gudsnuk K, Kuo SH, Cotrina ML, Rosoklija G, Sosunov A, et al. Loss of mTOR-dependent macroautophagy causes autistic-like synaptic pruning deficits. Neuron. 2014; 83: 1131-1143.
- Voss S, Cerna J, Gothe NP. Yoga Impacts Cognitive Health: Neurophysiological Changes and Stress-regulation Mechanisms. Exerc and Sport Sci Rev. 2022; 51: 73-81.
- Muller CL, Anacker AMJ, Veenstra-VanderWeele J. The serotonin system in autism spectrum disorder: From biomarker to animal models. Neuroscience. 2016; 321: 24-41.
- Gulati K, Sharma SK, Telles S, Balkrishna A. Self-esteem and performance in attentional tasks in school children after 4½ months of yoga. Int j of yoga. 2019; 12: 158-161.
- Frank JL, Kohler K, Peal A, Bose B. Effectiveness of a school-based yoga program on adolescent mental health and school performance: Findings from a randomized controlled trial. Mindfulness. 2017; 8: 544-553.
- Basso JC, McHale A, Ende V, Oberlin DJ, Suzuki WA. Brief, daily meditation enhances attention, memory, mood, and emotional regulation in non-experienced meditators. Behav Brain Res. 2019; 356: 208-220.
- Kral TRA, Imhoff-Smith T, Dean DC, Grupe D, Adluru N, Patsenko E, etal. Mindfulness-Based Stress Reduction-related changes in posterior cingulate resting brain connectivity. Soc Cogn and Affect Neurosci. 2019; 14: 777-787.
- LEE RLT, Ho LLK, Lam SKK, Chan DNS, Tang ACY, Fung KHK, et al. The Effects of a Group-Based Laughter Yoga Intervention on Mood, Anxiety and Loneliness in Adolescents with Mild Intellectual or Developmental Disabilities: A Pilot Randomized Controlled Trial. 2025: 19.
- Lynch J, Prihodova L, Dunne PJ, Carroll Á, Walsh C, McMahon G, et al. Mantra meditation for mental health in the general population: A systematic review. Eur J of Integr Med. 2018; 23: 101-108.
- Mehling WE, Wrubel J, Daubenmier JJ, Price CJ, Kerr CE, Silow T, et al. Body Awareness: a phenomenological inquiry into the common ground of mind-body therapies. Philos Ethics Humanit in Med. 2011; 6: 6.









































































































































{kind=link}