Exercise-Induced Anaphylaxis: A Rare Case in a Healthy Young Adult
- 1. Department of Immunology, Memorial Souad Kafafi University Hospital of Medicine, Egypt
Abstract
Exercise-induced anaphylaxis (EIA) is a rare and potentially life-threatening reaction that occurs during physical activity or shortly after it. We present a 22-year-old male who developed widespread hives, itching, dizziness, and hypotension while exercising at the gym. He had no prior history of allergies, medication use, or recent food intake. Unlike food-dependent cases, this patient’s symptoms were triggered solely by physical exertion, highlighting the variable nature of EIA. Awareness of this condition and prompt recognition remain essential, as exercise alone can provoke severe, life- threatening reactions in susceptible individuals. Only a few EIA cases have been reported in the literature. some proposed treatments, knowledge gaps persist, highlighting the need for early recognition, exclusion of other causes, and appropriate evaluation to achieve optimal outcomes.
Keywords
• Exercise; Anaphylaxis; Allergy; Food; Itching; Rash; Urticaria
Citation
Gabr I (2025) Exercise-Induced Anaphylaxis: A Rare Case in a Healthy Young Adult. J Immunol Clin Res 8(2): 1057.
ABBREVIATIONS
EIA: Exercise-Induced Anaphylaxis; FDEIA: Food Dependent Exercise-Induced Anaphylaxis; IgE: Immunoglobulin E; CPR: Cardiopulmonary Resuscitation; BP: Blood Pressure
INTRODUCTION
Exercise-induced anaphylaxis (EIA) is a potentially life-threatening allergic reaction typically triggered by physical activity and sometimes associated with food cofactors or underlying atopic conditions [1]. However, in rare instances, EIA can occur in otherwise healthy individuals, without prior allergen exposure or underlying medical conditions [2]. This unusual presentation raises questions about the pathophysiology, predisposing factors, and optimal management strategies for such patients [3]. Recognition of EIA in individuals without known allergies presents a diagnostic and preventive challenge. Although uncommon, early identification and intervention are critical, as EIA can rapidly progress to hypotension, airway compromise, or cardiovascular collapse [2]. The aim of this article is to present a clinical case of exercise induced anaphylaxis in a previously healthy young adult, accompanied by a review of relevant literature, emphasizing diagnostic considerations and preventive strategies.
CASE PRESENTATION
A 22-year-old male presented to the emergency department after developing anaphylaxis during exercise at the gym. Approximately 10 minutes after starting his workout, he developed a rash with severe itching all over his body (Figure 1A,1B,1C), followed by progressive shortness of breath and the onset of loss of consciousness. On hospital admission, his blood pressure was 80/50 mmHg. He was promptly treated with intramuscular epinephrine and antihistamine (Avil). His symptoms resolved within approximately 4 hours. The patient was discharged after complete resolution of symptoms and was advised to follow up with an immunologist for further evaluation. The patient reported no previous reactions to exercise or fasting and had no personal or family history of anaphylaxis, atopic disease, drug allergy, or vaccine allergy. He had no prior history of allergic reactions. He had not eaten, taken any medications, or received any vaccines several hours before exercise.
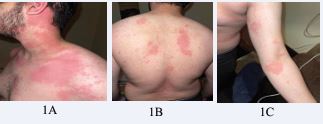
Figure 1 Widespread urticarial rash observed during the acute episode involving the anterior trunk, the posterior trunk, and the upper limb.
DISCUSSION
EIA: Exercise-Exercise-induced anaphylaxis (EIA) is a rare condition triggered by physical activity, with or without a food cofactor [1]. Population-based studies, including a survey of ~76,000 students in Yokohama, confirm its low prevalence [2], while longitudinal and registry data highlight aerobic activities, such as running, or gym-based exercise, as common triggers [3,4]. Food dependent EIA (FDEIA), although even rarer (~0.018% in some Japanese cohorts), demonstrates the additive effect of food and exercise in precipitating anaphylaxis [5]. EIA represents a heterogeneous condition in which physical activity alone or combined with food can provoke systemic allergic reactions, and this spectrum is reflected in several reported cases [6].
For instance, Ukleja-Soko?owska et al., described a 27-year-old male who developed anaphylaxis after consuming kiwi following gym exercise; provocation testing confirmed that symptoms appeared only when exercise was combined with food, illustrating FDEIA [7]. Similarly, Matsuo et al., reported a 21-year-old male with wheat-dependent EIA, who experienced generalized urticaria, hypotension, and dyspnea only after running post- meal, while wheat ingestion at rest was asymptomatic [8]. Lee et al., described a 22-year- old female with shellfish-associated EIA, whose reactions occurred only when exercise followed shellfish consumption [9].
The patient had been exercising regularly without any problems; however, after a six- month break, he experienced the reaction upon returning to physical training. In contrast, our case demonstrates EIA without any preceding food trigger, indicating that physical activity alone can be sufficient to provoke severe reactions [3,4]. No medications, vaccines, or food had been taken prior to exercise, and skin-prick test to common food allergens was negative (Figure 2), making FDEIA unlikely [4-6]. These cases collectively emphasize the clinical heterogeneity of EIA: some patients develop symptoms only when exercise is combined with specific food intake, while others, like our patient, experience reactions solely from physical exertion [1-5].
Diagnosing EIA is challenging due to the lack of definitive criteria and depends on excluding other causes through detailed history and physical examination [10]. Provocation testing, such as an exercise-challenge test, may reproduce symptoms and confirm the diagnosis of EIA, but it carries inherent risk and must be performed under strict medical supervision [11]. Therefore, careful clinical assessment, consideration of potential triggers, and supportive laboratory studies (such as serum histamine or tryptase when available) remain essential [6,7]. Collectively, these findings highlight the variable presentations, diagnostic difficulties, and potentially life- threatening nature of EIA, emphasizing the importance of individualized patient evaluation and preventive strategies tailored to the presence or absence of food cofactors [1-5].
The patient was advised to follow strict safety precautions during physical activity. He should always train with a companion who is aware of his condition, keep his cell phone accessible, and carry an EpiPen at all times, ensuring it is in date. Family members, friends, and gym staff should be familiar with its use and trained in basic CPR to respond promptly in case of an emergency [12]. In addition, the patient may take a non-sedating H1 antihistamine before activity to reduce mild allergic symptoms, including itching or hives [13]. While this can help alleviate some reactions, it does not prevent severe anaphylaxis, so the EpiPen must always be immediately accessible [12]. Other pharmacologic options, such as leukotriene receptor antagonists or short-acting beta agonists, can be considered individually under medical supervision, although evidence for their efficacy is limited [14]. Education on early recognition of warning signs, timely self-administration of medication, and adherence to a personalized safety plan are essential for effective management [12,13].

Figure 2 Skin prick test showing negative reactions to common allergens (wheat, peanuts, dust, soy, milk, egg, tomato, and kiwi).
ACKNOWLEDGEMENTS
I would like to express my sincere gratitude to the Department of Immunology at Memorial Souad Kafafi University Hospital for their kind support and valuable guidance throughout the preparation of this case report.
REFERENCES
- Sheffer AL, Austen KF. Exercise-induced anaphylaxis. J Allergy ClinImmunol. 1980; 66: 106-111.
- Shadick NA, Liang MH, Partridge AJ, Bingham III CO, Wright E, Fossel AH, et al. The natural history of exercise-induced anaphylaxis: survey results from a 10-year follow-up study. J Allergy Clin Immunol. 1999; 104: 123-127.
- Yamaguchi M, Shimizu A, Nakamura T. Epidemiology of exercise- induced and food-dependent exercise-induced anaphylaxis in Japanese school children. Allergol Int. 2006; 55: 369-375.
- Wade TR, Clark S, Hill DJ. Common triggers and clinical features of exercise- induced anaphylaxis. J Pediatr. 2000; 136: 517-522.
- Shadick NA, Liang MH, Partridge AJ. Long-term follow-up of exercise- associated anaphylaxis in adults. J Allergy Clin Immunol. 1999; 104: 789-793.
- Morita E, Kunie K, Matsuo H. Food-dependent exercise-inducedanaphylaxis. J Dermatol Sci. 2007; 47: 109-117.
- Matsuo H, Morita E, Ebisawa M. Wheat-dependent exercise-induced anaphylaxis in Japanese adults. Allergol Int. 2011; 60: 377-381.
- Lee HJ, Park HS, Kim JH. Shellfish-associated exercise-induced anaphylaxis: a case report. Allergy Asthma Immunol Res. 2013; 5: 328-331.
- Harada S, Morita E, Tanaka T. Risk of supervised exercise challenge in exercise-induced anaphylaxis: case series. Allergol Int. 2010; 59: 233-236.
- Barg W, Medrala W, Wolanczyk-Medrala A. Exercise-induced anaphylaxis: an update on diagnosis and treatment. Curr Allergy Asthma Rep. 2011; 11: 45-51.
- Caffarelli C, Passalacqua G, Piazza M. Exercise-induced anaphylaxis in children and adolescents. Pediatr Allergy Immunol. 2012; 23: 230- 237.
- MacCallum DS, Smith MM. Exercise-induced anaphylaxis. Sports Med Today. 2010; 23: 78-80.
- Christensen MJ, Sekerel BE. Exercise-induced anaphylaxis: causes, consequences, and management strategies. Immunol Allergy Clin North Am. 2019; 39: 541-551.
- Australasian Society of Clinical Immunology and Allergy (ASCIA). Acute management of anaphylaxis guidelines. Aust J Clin Immunol Allergy. 2022; 52: 145-152.









































































































































{kind=link}