Indications of Anatomical Lung Resection in the Pulmonary Hydatid Cyst: About 21 Cases
- 1. Department of Thoracic Surgery, Hospital Center University Hassan II, Morocco
- 2. Department of Medicine and Pharmacy, Sidi Mohamed Ben Abdallah University, Morocco
Abstract
Introduction: The pulmonary hydatid cyst in adults, presents the second localization after the liver. The basic treatment remains surgery, most often by a conservative intervention of the pulmonary parenchyma, however sometimes anatomical lung resection is indicated. The purpose of this study is to specify the main indications of this anatomical resection for this benign pathology.
Material and methods: This is a retrospective study involving 21 patients over a period of 8 years, all operated for a pulmonary hydatid cyst by ananatomical lung resection.
Results: Among 21 patients, there were 10 men and 11 women, with a mean age of 33.6 years. A contact with dogs and habitat in a rural environment was found in 13 patients (62%). Hemoptysis was reported in 14 patients (66.66%), whereas hydatid vomica was present in only 5 patients (23.8%). The imagery showed right-side in 13 patients (61.9%) and left-side in 8 patients (38.1%), with a ruptured hydatid cyst in 11 patients (52.38%) versus intact hydatid cyst in 10 patients (27.6%). Surgery was retained for all patients, and lobectomy was performed in 10 patients (47.6%), and segmentectomy in 10 patients also (47.6%), with bilobectomy in one patient. The follow-up was simple in 17 patients (80.95%), against 2 cases of postoperative pneumonia (9.52%), and 2 cases of prolonged air leakage (9.52%). Mean follow-up in this study was 2 years, with no recurrence recorded.
Conclusion: Conservative surgery presents the reference procedure in the pulmonary hydatid cyst, but anatomical resection remains the best option in some cases.
Keywords
Hemoptysis; Echinococcus granulosus; Hydatid cyst; Complication; Thoracic surgery.
CITATION
Harmouchi H, Lakranbi M, Belliraj L, Ammor FZ, Issoufou I, et al. (2018) Indications of Anatomical Lung Resection in the Pulmonary Hydatid Cyst: About 21 Cases. J Liver Clin Res 5(2): 1048.
INTRODUCTION
The pulmonary hydatid cyst is a benign parasitic pathology that constitutes aendemic health problem in Morocco. This pulmonary localization remains the most frequent in adults after the liver [1]. The ruptures in the bronchial tree or in the pleural cavity are the most complications. The best therapeutic option is surgery, which is usually based on conservative lung parenchyma. However, some cases require anatomical lung resection. The purpose of our series is to specify the cases where a anatomical lung resection will be indicated in this pathology which remains benign.
MATERIALS AND METHODS
This was a retrospective, single-center study, involving 21 patients operated between January 2010 and December 2017 in the department of thoracic surgery at the CHU Hassan II of Fez, whose intervention was anatomical lung resection by a lobectomy, segmentectomy, bilobectomy or pneumonectomy. The objective of our study is to show the situations where a regulated resection is necessary for this pathology which remains benign. We recorded all the demographic, clinical and radiological data, the surgical procedure and the evolution of the patients in a previously established chart.
RESULTS
Among 21 patients, there were 10 men and 11 women, with an average age of 33.6 years (Table 1).
|
Table 1: Characteristics of patients. |
|
|
Patient data |
Numbers of patients (percentage) |
|
Median age |
33,6 ans |
|
Sex :
|
10 (47,6%) 11 (52,3%) |
|
Pathological antecedents:
|
13 (62%) 3 (14%) 5 (23,8%) |
|
Side :
|
13 (61,9%) 8 (38,1%) |
|
Hydatid serology :
|
3 (14,2%) 18 (85,7%) |
|
Functional sign:
|
14 (66,66%) 11 (52%) 5 (23,8%) 4 (19%) |
|
Intervention :
|
10 (47,6%) 10 (47,6%) 1 (4,7%) |
|
Postoperative complications :
|
17 (80,95%) 2 (9,52%) 2 (9,52%) |
A notion of contact with dogs and habitat in a rural setting was found in 13 patients (62%), and a chronic active smoking in 3 patients (14%). Hemoptysis was reported in 14 patients (66.6%), chest pain in 11 patients (52%), and mucopurulent sputum in 4 patients (19%). However, a hydatid vomica was present only in 5 patients (23.8%).The clinical examination showed a syndrome of pulmonary condensation in 8 patients (38%). The hydatid serology requested in all our patients was positive only in 3 patients (14.2%). The radiological assessment showed right side involvement in 13 patients (61.9%), and left side in 8 patients (38.1%), with a ruptured hydatid cyst in 11 patients (52.38%) versus intact hydatid cyst in 10 patients (47.6%). The mean diameter of these intact hydatid cysts was 13 cm. The chest x-ray showed a homogeneous opacity of water tone in 8 patients (38%), anair-fluid level with image of floating membranes in 3 patients (14,2%), and a cavitary image in 3 patients (14,2%), a small bell image in 3 patients (14.2%), a white hemithorax in 2 patients (9.52%), and aexcavated appearance in 2 patients (9.52%). Thoracic CT performed in all patients objectified a cavitary image in 3 patients (14.2%), an air-fluid level image in 3 patients (14.2%), a crescent gas appearance in 2 patients (9.52%), and air bubble sign in 2 patients (9.52%) (Table 2).
|
Table 2: Radiological characteristics of patients. |
|
|
Radiologicalcharacteristics |
Numbers of patients (percentage) |
|
11 (52,38%) 10 (27,6%) |
|
Chest X-Ray :
|
8 (38%) 3 (14,2%) 3 (14,2%) 3 (14,2%) 2 (9,52%) 2 (9,52%) |
|
Thoracic CT :
|
3 (14,2%) 3 (14,2%) 3 (14,2%) 2 (9,52%) |
A hydatid cyst of liver was associated in 3 patients (14.2%). Surgery was retained for all patients, and lobectomy was performed in 10 patients (47.6%), a segmentectomy in 10 patients (47.6%). However, only one bilobectomy was performed, and no pneumonectomy in our series was performed. It should also be noted that 3 cases had benefited of a pleuropulmonary decortication for hydatid cysts ruptured in the pleural cavity. The complications were simple in 17 patients (80.95%), against 2 cases of postoperative pneumonia (9.52%), and 2 cases of prolonged air leakage (9.52%). The median duration of hospitalization was 6 days, and 7 patients (33.3%) required antihelminthic treatment. The average of follow-up in this study was 2 years, with no recurrence recorded.
DISCUSSION
The hydatid cyst of the lung corresponds to the development of the larval form of Tenia Echinococcus granulosus. After passing through the digestive system, the parasite passes into the liver and reaches the lung via the inferior vena cava. Once fixed, it can be destroyed by a host reaction or by unsuitability to local physiological conditions, as it can continue its development by undergoing a cystic transformation into a hydatid cyst or be ruptured in the bronchial tree and easily acquires a superinfection, because of direct contact of the tracheobronchial system with the external environment (Figure 1) [2-4].
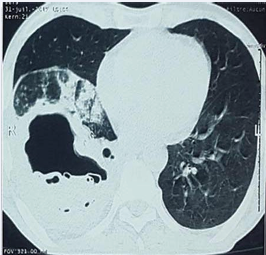
Figure 1: Thoracic CT in the parenchymal window showing a ruptured hydatid cyst of the right lower lobe fractured, with underlying pneumopathy.
Due to the elasticity and compliance of the lung parenchyma, the pulmonary hydatid cyst rapidly increases in size in the lungs than in other organs. The hydatid cyst can grow considerably without causing symptoms; however this symptomatology depends on the size of the cyst and its lung localization [5]. Generally, hemoptysis is a symptom rarely described in the pulmonary hydatid cyst [3,6]. The choice of the patients benefiting of anatomical lung resection in this series explains the frequency of haemoptysis in 66% of patients, since the parenchymal sequelae has already been established. Hydatid vomica, which is apathognomonic functional sign, present in 5 patients, testifies to the rupture of the hydatid cyst in the bronchial tree. The radiological expression of an intact hydatid cyst is often a rounded homogeneous opacity, well limited, of water tone (Figure 2,3).
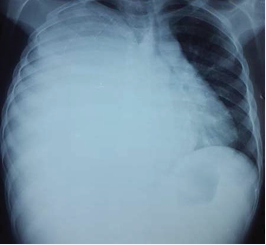
Figure 2: Chest X-ray showing a white right hemithorax corresponding to a giant right hydatid cyst.

Figure 3: CT thoracic in mediastinal window in favor of a giant right hydatid cyst pushing back the mediastinum towards the contralateral side.
However, several aspects were described in the ruptured hydatid cyst: signet ring sign, crescent sign and inverse crescent sign, air bubble sign and honeycomb, air-water level, double arch sign, serpiginous aspect, dry cyst sign, ball of wool aspect, small bell image, pseudotumoral aspect, sequela image, residual cavity, and cicatricial image [7]. Surgery remains the best therapeutic option in pulmonary hydatid cysts and should be operated as soon as they are diagnosed, since their usual course of evolution is the rupture either in the bronchial tree or in the pleural cavity, and since they can cause parenchymal lung destruction, or rarely result an anaphylactic reaction that may be life-threatening [8,9]. Conservative surgery of lung parenchyma remains the gold standard for the pulmonary hydatid cyst of the lung, either by enucleation, cystectomy or wedge resection. However, a controlled anatomical lung resection is indicated in cysts that cause parenchymal sequelae, and involve more than 50% of a pulmonary lobe, or presence of multiple cysts in the same lobe, or cysts that are associated with sequelae such as abscess chronic or bronchiectasis [5,10,11]. Giant hydatid cysts defined by a diameter greater than 1 cm [12], exert a chronic mass effect on the underlying parenchyma, and causes sequelae of bronchectasias, or even a destroyed lobe. In our series, the mean diameter of 10 full hydatid cysts was at 13 cm explaining the achievement of a systematized lung resectionfor these patients. Four lobectomies of middle lobe have been performed in this series, which is explained by the small volume of this lobe, and a chronic compressive effect can easily leave parenchymal sequelae. Often it is difficult to predict that anatomical resection will be required at the imaging stage, since after aspiration of the hydatid fluid and ventilation of the underlying parenchyma the quality of the pulmonary lobe is well appreciated. Vasquez at al reports a series of 115 patients with a lobectomy rate in 52% of cases [13]. Pneumonectomy remains exceptional in pulmonary hydatid pathology. However, in a series of 88 patients published in 2002, Amez et al recorded a pneumonectomy rate of 11.5% [13,14]. No pneumonectomy was performed in our series. The main complications described in the hydatid cyst surgery remains wound site infection, hemothorax, pyothorax, postoperative pneumonia, and prolonged air leakage. No complications were noted in our series.
CONCLUSION
Hydatid cyst of the lung remains a benign parasitic pathology whose ideal treatment is the surgery which is most often conservative of the pulmonary parenchyma. However, anatomical lung resection is sometimes indicated. Individual and collective prophylaxes, as well as early surgery, are the best procedures to avoid failure of the lung resection stage for this benign pathology.









































































































































