Inferior Vena Cava Aneurysm: A Novel Association with Polycystic Liver Disease
- 1. Department of Surgery, University of North Carolina School of Medicine, USA
- 2. Department of Radiology, University of North Carolina School of Medicine, USA
- 3. Lineberger Cancer Center, University of North Carolina School of Medicine, USA
Abstract
Polycystic liver disease (PCLD) is a rare disorder in which the hepatic parenchyma is progressively replaced by liver cysts. While the majority of patients are asymptomatic, the most common source of symptoms is related to the associated hepatomegaly and mass effect secondary to the cysts. We present the case of an asymptomatic patient with PCLD who was incidentally diagnosed with a suprahepatic inferior vena cava (IVC) aneurysm. This is an uncommon finding of a rare disorder with no prior published reports. With the lack of existing data we have proposed expectant management and observation for this patient.
Keywords
Polycystic liver disease; Vena cava aneurysm; Vascular malformation.
CITATION
Hutchinson CM, Overby DW, McGinty K, Gerber DA (2018) Inferior Vena Cava Aneurysm: A Novel Association with Polycystic Liver Disease. J Liver Clin Res 5(1): 1043.
INTRODUCTION
Polycystic liver disease (PCLD) is a rare disorder in which the hepatic parenchyma is progressively replaced by liver cysts [1]. There are two types of PCLD: sporadic and autosomal dominant PCLD. In sporadic PCLD, the hepatic cysts are smaller, asymptomatic and do not completely replace the liver parenchyma. Patients with sporadic PCLD do not develop extrahepatic manifestations nor do they require ongoing follow-up. In autosomal dominant PCLD there is progressive replacement of normal liver parenchyma with cysts of various sizes that eventually become symptomatic leading to a mass effect within the abdominal cavity. There are many associated complications with autosomal dominant PCLD including abdominal wall hernia, abdominal fullness, lower extremity edema, ascites, pain, cyst hemorrhage, rupture or infection [2]. After a complete review of the literature there are no described cases of PCLD-related diaphragmatic herniation contributing to vascular malformations.
CASE PRESENTATION
An asymptomatic 60-year-old male initially presented for treatment of a perirectal abscess. His past medical history was unremarkable and he had no prior or family history of liver disease. After antibiotics and drainage, interval computed tomography (CT) of the abdomen revealed a polycystic liver with herniation through the diaphragm causing a markedly dilated supradiaphragmatic IVC aneurysm (Figures 1,2).
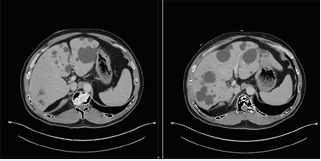
Figure 1: Axial CT images showing numerous hepatic cysts replacing normal liver parenchyma.
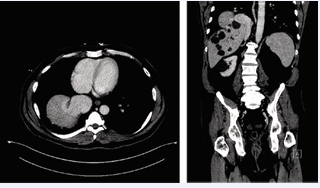
Figure 2: Axial and coronal CT images demonstrating hepatic herniation through the right hemidiaphragm and dilation of the suprahepatic IVC. There is no evidence of thrombus or azygous venous collaterals.
The CT scan demonstrated no enlarged azygous venous collaterals and no IVC thrombus. The patient’s hepatic laboratory tests were normal and there was no evidence of coagulopathy or presence of liver disease based on his imaging or lab work (i.e. portal hypertension, ascites, varices, encephalopathy). His case was discussed at a multidisciplinary hepatobiliary conference with the recommendation for an observational approach.
DISCUSSION
PCLD occurs as either a sporadic variant with isolated liver cysts or as a genetic autosomal dominant entity frequently associated with complications due to mass effect. It can also be seen in association with polycystic kidney disease. While the amount and severity of cystic burden can vary in PCLD, most patients remain asymptomatic and are typically managed expectantly [3].
Complications of PCLD including hernia, ascites, lower extremity edema, and pain are associated with increasing liver mass [2]. Severe PCLD can result in IVC or portal venous compression and associated portal hypertension. Liver herniation has been previously described as a result of PCLD [4]. However, supra diaphragmatic liver herniation associated with vascular malformations has not been described in the literature.
While there is no strict “normal” caliber of the IVC, as the diameter changes with volume status, patient size and flow dynamics, the expected contour of the inferior vena cava is smooth, without focal dilatation. In any vein, when there is limited dilatation (such as in this case), this leads to a diagnosis of aneurysm. In the absence of intervention or surgery, congenital aneurysm is the most likely diagnosis. Venous aneurysms are rare, particularly those involving the IVC. Trauma, inflammation, congenital weakness or degenerative changes must be considered as possible causes [5]. Complications of caval aneurysms can include deep vein thrombosis, lower extremity swelling, abdominal and/or back pain, rupture, penile bleeding, IVC syndrome, pulmonary embolism or other thromboembolic phenomena, such as paradoxical cerebral embolism [6]. Gradman and Steinberg developed a classification system for IVC aneurysms based on anatomic location and presence of venous thrombus [7]. Type I caval aneurysms are aneurysms of the suprahepatic IVC without venous obstruction. Eight case reports of Type I IVC aneurysm were found in the literature compromising 23 patients [6,8]. Several strategies have been described that cross the spectrum of operative and non operative management. Considering thrombus formation was unlikely in Type I IVC aneurysms, a conservative approach was recommended regardless of aneurysm size or etiology for the majority of these cases (95%) [9]. Survival outcomes were only recorded for 7 of the patients with a survival of 85%, though long term follow up was lacking [6,9].
Montero-Baker developed a treatment algorithm for IVC aneurysms based on symptomatology and classification (Type I-IV) (Figure 3) [9].
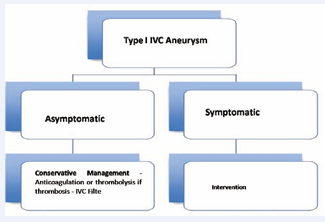
Figure 3: Management algorithm for Type I IVC Aneurysm (Adopted from Montero-Baker “Management of inferior vena cava aneurysm” 2015) [9].
Asymptomatic, Type I aneurysms were managed conservatively with medical optimization along with anticoagulation, thrombolysis or IVC filter if thrombus was present. Conservative management was also recommended for aneurysms < 5cm that remain stable or for patients with significant comorbidities or challenging IVC anatomy [9]. Conservative management consisted of serial ultrasound examinations without need for anticoagulation. Symptomatic patients were referred for intervention.
This patient presented with a supra diaphragmatic IVC aneurysm meeting criteria of a Type I IVC aneurysm and an observational approach was recommended based on existing treatment algorithms. However, little data for long term follow up exists and future longitudinal studies are needed to assess for late complications from IVC aneurysms [6].
ETHICAL APPROVAL
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
ACKNOWLEDGEMENT
CMH- manuscript writing; data collection, DWO- manuscript editing, KM- Image processing and review; manuscript editing, DAG- project development; manuscript writing/editing









































































































































