Report of Cases of Ruptured Pulmonary Hydatid Cysts with Complications of Hydro or Tension Pneumothorax
- 1. Department of Thoracic & General Surgery, Guilan University of Medical Sciences, Iran
- 2. Resident of General Surgery, Guilan University of Medical Sciences, Iran
Abstract
Tension pneumothorax is very rare complications of the pulmonary hydatid cyst and its diagnosis and treatment is still a complex of problem. We report four cases of tension pneumothorax, of which, two cases were referral to our hospital from local hospital with complaints of chest pain, cyanosis and dyspnea. Chest radiograph showed tension pneumothorax with mediastinal shift, and tracheal displacement. They had persistent air leaks with lung collapse despite insertion of chest tube. CT-scan of chest, performed in our center, showed lung was collapsed with air fluid level. All patients underwent bronchoscopy after stabilizing cardiovascular problems. Patients were taken to the operating room. During operation and exploration, ruptured pulmonary hydatid cysts were found in all four patients with a lot of debris and laminated membrane in the pleural space. Histopathological examination confirmed the diagnosis of hydatid cyst. Patients were discharged in good condition after 6 to 8 days of post operative period with the advice of Albendazole [800mg] daily. Ruptured pulmonary hydatid cyst should be kept in mind in the differential diagnosis of tension pneumothorax and surgical intervention should be performed as early as possible.
Keywords
Tension pneumothorax; Pulmonary hydatid cysts; Laminated membrane; Albendazole.
CITATION
Aghajanzadeh M, Omidmosafaii, Torabi H, Ziabari M, Pursafar M (2018) Report of Cases of Ruptured Pulmonary Hydatid Cysts with Complications of Hydro/Ten sion Pneumothorax. J Liver Clin Res 5(1): 1046.
INTRODUCTION
Hydatid disease is a serious health problem in some area in the world such as, Mediterranean region, the Middle East, New Zealand, and South Africa. In some countries like Iran and South Africa, it is endemic [1,2]. Although it can be found in any part throughout the body, it is more common in the liver (65 to75%) and lung [15%] Concomitant pulmonary and liver hydatid cysts occur in 4% to 25% of patients with echinococcosis [1,2]. It is imperative to investigate the possibility of new cysts in other parts of body in patients diagnosed with either a pulmonary or hepatic cyst Intrapleural rupture occurs in 5% of cases and may produce an acute clinical picture as intense chest pain, persistent cough, severe dyspnea, cyanosis, shock, and suffocation [3-5]. Liver cysts can also rupture into the peritoneum causing peritonitis, or trans diaphragmatically into the pleural space or bronchial tree causing pulmonary hydatidosis or a bronchial fistula [3]. Liver hydatid cysts can also rupture into the peritoneum causing peritonitis, or trans diaphragmatically into the pleural space or bronchial tree causing pulmonary hydatidosis or a bronchial fistula [3,6].The most frequent complication of pulmonary hydatid disease is the rupture of the cyst into tracheo-bronchial tree [5-7]. If a cyst rupture into the pleura or pulmonary parenchyma, it can be a severe and life threatening, such as tension pneumothorax [2-5].Diagnosis tools are clinical presentation, CXR and CT-scan of the chest [2,4,5]. Serological tests are less reliable in such condition we do not use these tests because false negative and positive are high [1-3]. Treatment of these cases are mainly surgery. The aim of surgical intervention in pulmonary hydatid cysts are mainly the removal of the laminated membrane without causing more intraoperative contamination and prevention of an intrapulmonary residual cystic cavity [2,3,7,8]. Here, we evaluated four patients with pulmonary hydatid cysts which presented with rare presentation of tension hydro/ pneumothorax during six years duration.
CASE PRESENTATION
Case 1
A 56-year old woman, whose family lives in a rural area , was admitted to local cardiac hospital with complaints of sever left sided chest pain, and sever dyspnea. Her physical examination revealed severe respiratory distress with a respiratory rate of 37 beats/ per minute , tachycardia of 120/per minut, blood pressure of 80/60 mm Hg, and decrease breath sounds at the left hemithorax. Chest radiograph taken on admission showed tension hydro/pneumothorax, mediastinal shift, and tracheal displacement (Figure 1A). Tube thoracostomy was placed, where there was a considerable air leake.All lab date was normal .She was referred to our hospital with chest –tube because of air leak and left lung collaps. CT-scan of chest was taked and show collaps of left lung with loculated pneumothorax (Figure-1B), She was taken operating room on next room. Left anterolateral thoracotomy was performed through the 5th intercostals space. During operation,displacing and compressing the left lower lobe.
After aspiration of pleural space, with a ring forceps laminated membranes were removed (Figure-1C). The pericystic cavity was irrigated with norma lsaline solution. All debris were removed, Small bronchial openings were found using saline and with application of positive intrapulmonary pressure. We closed them separately with 2-0 Vicryl. Then the residual cavity was obliterated with purse-string sutures from the deepest of cavity to the surface (capitonnage). The remnant pricyst of cavity was removed (Figure-1D).
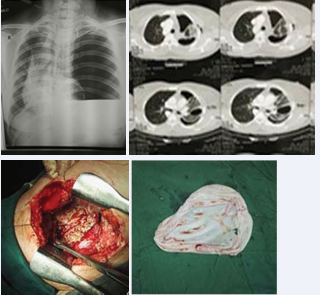
Figure 1: A: Show CXR with totally collapsed of left lung hydro/ pneumothorax and shift of mediastinum to the right. B: Show CT-scan of chest after chest-tube insertion and collapsed of left lung. C: Show debris of pleural space, D: Show laminate membrane.
Postoperative recovery was uneventful and she was discharged on the sixth postoperative day. Histopathological examination confirmed the diagnosis of hydatid cyst. Albendazole treatment (800mg) was prescribed.
Case 2
A 37-year old man admitted in our thoracic surgery ward with severe dyspnea and chest pain of sudden onset. Physical examination revealed severe respiratory distress (RR of 37 / per minute), tachycardia 120/per minute,BP of 90/60 mm and breath sounds on the left hemithorax. Chest radiograph showed a left hydro/ pyo pneumothorax with shift of mediastinum to right (Figure 2A). A chest tube was inserted in emergency room. He was transferred to Thoracic Surgery Department because of persistent air leak, and collapsed left lung. CT scan of the chest (Figure 2B) revealed collapse of left lung.
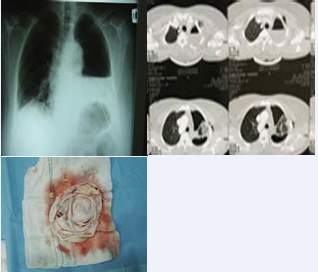
Figure 2 :A: Show CXR with hydropneumothorax of left side and mild shift of mediastinum to the right. B: Show CT-scan of chest after chest tube insertion and collapsed of left lung. C: Show laminate membrane.
Left thoracotomy was done. During exploration, laminated membrane and debris were present in the pleural space (Figure 2C). The laminated membrane and debrides were removed through washing of pleural cavity and bronchial opening was closed with vicryl-2 suture. Remnant cavity was closed with cap tonnage and resection of remnant fibrotic tissues. Lung decortication was performed and chest tube was inserted .Albendazole 800 mg/day was started two days after postoperative period for 3 months with an interval of 14 days between one month and another.
Case 3
A 35year-old male patient, with right chest drain was referred to our Thoracic Surgery department from local hospital (Figure 3A). The cause of referral was persistent air leak, lung collapse and effusion. The lung failed to re expand despite bronchoscopy, chest physiotherapy and continuous suction by inserting chest tube (Figure 3B). Chest CT scan showed a huge cavity with air fluid level in left lower lobe. The patient underwent right thoracotomy. During exploration, pus covered laminated membrane and debris were present in the pleural space (Figure 3C).
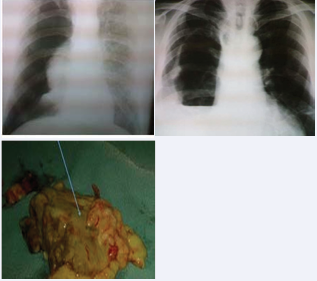
Figure 3: Show CXR with pneumothorax of right side and shift of mediastinum to the right. B: Show CXR after chest-tube insertion and collapsed of left Fig. C: Show pas covered laminate membrane.
The laminated membrane and pus were removed through washing of pleural cavity and bronchial opening was closed with vicryl-3 suture. Remnant cavity was closed after washout with normal saline and capitonnage, and finally, resection of remnant fibrotic tissues was performed. Lung decortication was performed and chest tube was inserted. Albendazole 800 mg/day was started after two days of postoperative period for 3 months with an interval of 14 days between one month and another. Patient was discharged in good condition.
Case 4
A 28-year-old male patient admitted to emergency service with dyspnea, chest pain and itching. On physical examination, he was in the state of shock, hypotensive and had macular skin lesions on the chest, abdomen, and both upper and lower extremities. The respiration rate was 32/min and breath sounds were absent on the left lung. After IV therapy of hydrocortisone , antihistamin and noradernalin, the patient condition improved. Posterior anterior (CXR) revealed hydropneumothorax on the left side (Figure 4A). On chest CT -scan examination, hydropneumothorax with the collapse of left inferior lung was observed (Figure 4B). On left side, chest tube was inserted. Laboratory data including biochemical parameters, whole blood count, liver, and kidney functions were normal. Low glucose and pH and high lactate dehydrogenase level of pleural fluid were suggestive of empyema in nature. At the 5th day persistent air leakage were found, and chest radiograph indicated an inadequate expansion of the left lung. Patient underwent to the left posterolateral thoracotomy with one lung ventilation. During exploration laminated membrane and debride were present in the pleural space .Twenty ml fluid was aspirated and laminated membrane was removed (Figure 4C).
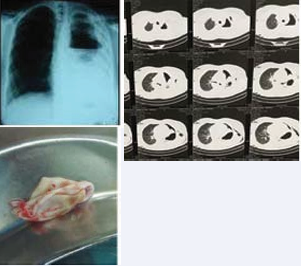
Figure 4: A: Show CXR with hydropneumothorax of left side after C-tube and mild shift of mediastinum to the right. B: Show CT-scan of chest after chest-tube insertion and collapsed of left lung. C: Show laminate membrane.
There was pleural peel on the left lung and decortication was done. Albendazole 800 mg/day was started postoperatively for 3 months with an interval of 14 days between one month and another. After an uneventful post-operative course, patient was discharged on the 6th postoperative day.
DISCUSSION
Hydatid cyst still remains an important health problem in developing countries [1-4,9]. It can appear in any place throughout the body and is more common in the liver (65 to75%) and lung (15%), In 10% frequently involves other organs [2]. Pulmonary hydatid cysts are asymptomatic until they reach a large size and become complicated [2,3,9,10]. A sudden rise in the intrapulmonary pressure, such as coughing, sneezing or an increase in intraabdominal pressure is the usual risk factor for rupture of the cyst. However rupture may occur spontaneously without any predisposing factor [4,5]. The occurrences of tension pneumothorax in the rupture of the pulmonary hydatid cyst is a rare complication [4-7]. The signs and symptoms of tension pneumothorax include severe dyspnea, cyanosis, tachycardia, engorgement of jugular vein in the neck and hypotension. Rarely macular skin lesions were present on the chest, abdomen and both upper and lower extremities as one of our patients [4-7]. The trachea and other components of mediastinum is usually deviated to the contralateral side, increased resonance to percussion on the affected side of the chest and absent breath sounds [4-6]. In our cases, physical examination of chest and chest radiographs, and histopathological examinations of surgically debridement of tissues were of great value in diagnosing the ruptured pulmonary hydatid cyst. The cavity in the lung and the bronchopleural fistula together worked as a check-valve mechanism and this phenomena cause tension pneumothorax [4,10]. A positive pressure inside the pleural cavity which shift the mediastinal structures to the contralateral side and interfering with the respiratory and cardiovascular systems [4,5,10]. These changes are responsible for the clinical picture in tension pneumothorax [4,7,10]. Serological tests are less reliable in such condition, we did not use routinely as these tests because false negative and positive is high [1-3]. The treatment of such patients are mainly surgery [3,5,8]. The aim of surgical intervention in pulmonary hydatid cysts are mainly the removal of the laminated membrane without causing intraoperative contamination and prevention of an intrapulmonary residual cystic space [1-3,8]. For this purpose, varying techniques, such as enucleation, pericystectomy, and simple cystotomy with or without capitonnage of the pericystic space can be chosen in proper conditions during the operation [3,8,10]. In cases with tension pneumothorax, we usually carried out : remove laminated membrane with washout of the remnant cavity , pricystectomy and then the cavity was obliterated by purse-string sutures from in base to top of cavity ( capitonnage) and finally decortications [1,3]. Radical pulmonary resections should be performed when the pulmonary parenchyma around the cyst is destroyed [2,3,8]. We used these procedures in all of our four cases without any morbidity and mortality.
CONCLUSION
Ruptured pulmonary hydatid cyst should be kept in mind in the differential diagnosis of primary pneumothorax and tension pneumothorax especially in endemic area and surgical intervention should be performed in first time after diagnosis. Postoperative and in hospital albendazole treatment is essential to avoid recurrence.









































































































































