"Hut Lung" - Domestically Acquired Particulate Lung Disease
- 1. Department of Medicine, SUNY Upstate Medical University, Syracuse, USA
Abstract
Domestically Acquired Particulate Lung Disease (DAPLD) or “Hut Lung” is a form of mixed dust pneumoconiosis and is the result of indoor air pollution, such as smoke and dust from biomass fueled stoves. With continued exposure, it can progress to cor pulmonale and severe respiratory failure. Here we report a case of a Nepali refugee with complaints of a chronic cough and dyspnea on exertion. She had an abnormal chest CT. Lung biopsies revealed findings consistent with mixed dust pneumoconiosis. We highlight the importance of considering the possibility of the mixed dust pneumoconiosis in the appropriate clinical setting, especially in women with a history of indoor exposures from biomass fueled stoves and stone grinding.
Keywords
Respiratory medicine, Pulmonology, Inhalational lung injury, Hut lung, DAPLD, Particulate lung disease, Biomass stoves, Pneumoconiosis, Dust inhalation, Cor pulmonale, Stone grinding
Citation
Masuta P, Nandavaram S, Trikha G (2017) “Hut Lung” - Domestically Acquired Particulate Lung Disease. J Prev Med Healthc 1(2): 1006
Abbreviations
DAPLD: Domestically Acquired Particulate Lung Disease; CT: Computed Tomography
INTRODUCTION
Domestically Acquired Particulate Lung Disease (DAPLD) or “Hut Lung” is a chronic non-infectious and non-malignant pulmonary disorder. It is a result of the inhalation of smoke, fine particles and chemical compounds released from the use of biomass fuels for cooking and stone grinding in poorly ventilated workplaces. This disease entity can be seen in industrialized and developed nations even in the absence of any occupational exposures, especially among immigrated patients. It requires special attention to the social, occupational, domestic history and living conditions. It is important to recognize this disease to prevent further exposure and thereby prevent progression.
CASE PRESENTATION
A 58-year-old woman with a medical history significant for hypertension and treated latent tuberculosis presented with complaints of non-productive cough and dyspnea on exertion for 3 months. She did not report any fever, chills, night sweats, weight loss or hemoptysis. She was a refugee from Nepal and moved to the United States in 2012. She never smoked and denied any history of alcohol or recreational drug use. She denied any occupational exposures, however, she did have significant exposure to smoke and dust from the use of charcoal, wood stoves and stone grinding, while she was in Nepal.
Physical exam was benign. Complete blood count and immunological panel were within normal limits. Spirometry, lung volumes and diffusion capacity were within normal limits. Chest x-ray (Figure 1) showed faint reticular opacities prominent in the mid to lower lobes. Computed Tomography (Figure 2) of the chest showed a diffuse mosaic attenuation pattern. There were multiple pulmonary nodules noted in the right middle lobe. There was no lymphadenopathy. Transthoracic echocardiogram showed impaired left ventricular relaxation with normal LV ejection fraction. Bronchoscopy and transbronchial biopsies of the right upper, middle and lower lobes were performed. Histopathology (Figure 3, Figure 4) revealed mild, nonspecific chronic inflammation. Acid-fast bacilli and fungal stains were negative. There was no evidence of malignancy. Given the persistent symptoms and abnormal CT findings, wedge biopsy of the right upper, middle and lower lobes was performed. Wedge resections showed alveolated lung with expansion of peribronchiolar interstitium by black dust-laden macrophages and dust macules. There were areas of peribronchiolar fibrosis with birefringent silicate and silica material within the interstitium and macrophages. Based on her history of exposure to stone grinding, charcoal and wood burning stoves along with the histopathologic findings consistent with mixed dust pneumoconiosis, she was diagnosed with "Hut Lung” or Domestically Acquired Particulate Lung Disease.
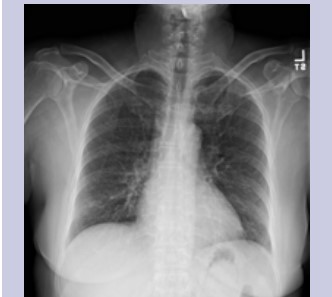
Figure 1: Chest X-Ray showing fine reticular opacities in the mid and lower lungs.
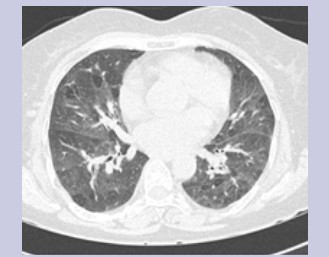
Figure 2: CT Thorax showing diffuse mosaic attenuation bilaterally.
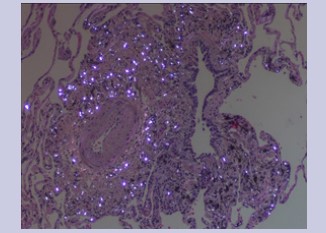
Figure 3: Histopathology showing birefringent silicate material within the interstitium.
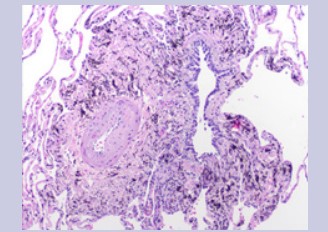
Figure 4: Histopathology showing non-specific granulomatous inflammation.
DISCUSSION
Hut lung is a form of mixed dust pneumoconiosis most commonly seen in developing countries. It is the result of smoke inhalation, fine particles and chemical compounds from the use of biomass fuels for cooking and from stone grinding in poorly ventilated homes. These fuels are typically composed of wood but can include straw, cornhusks and animal dung. The latter, in particular, is associated with longer burning times and greater particle emissions [1,2]. These dust particles deposit in the alveolar parenchyma and interstitium, where they are subsequently phagocytosed by macrophages and incite inflammation [3].
Symptoms are non-specific and depend on the duration of exposure to the smoke and dust. However, it is difficult to quantify the exposure and it is often limited by recall bias [1,3]. Symptoms can range from being asymptomatic to shortness of breath, with the most common symptom being chronic cough [1,2]. Based on the extent of involvement and degree of severity, pulmonary function tests can be normal or can reveal an obstructive or restrictive pattern [2]. Radiographic changes are nonspecific and include reticulation, ground glass opacities, nodules and progressive massive fibrosis [1,4]. Bronchoscopy often reveals dark black or anthracotic plaques in the airways. Lung biopsies reveal dust-laden macrophages, dust macules, fibrosis and birefringent particles [2]. Over time the disease process can progress to pulmonary fibrosis and cor pulmonale. High levels of carcinogens especially benzo(a)pyrene in the wood smoke increase the risk of malignancy [1,2].
There are no guidelines for the treatment of DAPLD. Prevention is the best treatment option. Improving ventilation and redesigning the biomass-fueled stoves are implementable measures to decrease the exposure to smoke and dust [3]. Early recognition and removal of the patient from the environment is the best treatment strategy to prevent progression of the disease.
CONCLUSION
DAPLD is mixed dust pneumoconiosis and is the result of indoor air pollution, such as smoke and dust from biomass fueled stoves. Through this case we highlight the importance of considering the possibility of the mixed dust pneumoconiosis in the appropriate clinical setting, especially in women with a history of such indoor exposures from biomass fueled stoves and stone grinding.
ACKNOWLEDGEMENT
We are very grateful to three anonymous reviewers for their helpful comments and peer-review
DISCLOSURE
The authors declare no conflicts of interest.
About the Corresponding Author
Dr. Pardeep Masuta
Summary of background: Dr. Pardeep Masuta is a resident physician in Internal Medicine at SUNY Upstate Medical University. He has attended Ross University in Dominica, West Indies.
Permanent e-mail address: pardeepmasuta@hotmail.com
Current research focus:
• Procalcitonin and antibiotic use
• Quality Improvement








































































































































