Covid-19 Vaccination Barrier Analysis in Five Selected Districts of Southern Province in Zambia
- 1. Zambia Ministry of Health (Namwala District Health Office), Lusaka, Zambia
Abstract
Background: To investigate the barriers that lead to people in the communities refuse to get vaccinated against COVID-19. There are perceptions that COVID-19 vaccines are surrounded with myths and misconceptions resulting in reduced vaccination rates. Therefore, this study was conducted to analyze COVID-19 vaccination barriers in communities and provide significant evidence for improved vaccination rates among eligible and vulnerable population.
Methods: This study used a mixed methods research design; utilizing both quantitative and qualitative research methodologies. The probability sampling method was utilized to select 150 participants. The qualitative data was collected through the focus group discussions (FGDs) while quantitative data through a pilot tested questionnaire. Data was analyzed using thematic analysis strategy and SPSS software.
Results: The results of this study indicated that most of the respondents accounting for 67.7% affirmed that the COVID-19 vaccines were good for them. In addition, 25.8% of the respondents did not know whether the COVID-9 vaccines were good for them or not whereas, 6.5% of the respondents indicated that the COVID-19 vaccines were not good for them. Furthermore, the majority of the participants which accounted for 70% indicated that they were willing to take the COVID-19 vaccines if presented to them however, the other category that refused to get vaccinated associated COVID-19 injections to Satanism and that the COVID-19 vaccines were developed to eliminate African population.
Conclusion: The COVID-19 vaccines were associated with major myths and misconceptions that resulted in failure by health authorities achieving herd immunity of the eligible population hence, policy makers and health promoters need to strengthen health promotion and public health interventions on COVID-19 vaccines in communities.
Keywords
• COVID-19; Vaccines; Health Promotion; Awareness; Community
CITATION
Mwenya S, Chilala M (2023) Covid-19 Vaccination Barrier Analysis in Five Selected Districts of Southern Province in Zambia. J Prev Med Healthc 5(1): 1029.
ABBREVIATIONS
COVID-19: Coronavirus Disease 2019; UNICEF: United Nations Children’s Fund; FGDs: Focus Group Discussions.
BACKGROUND
The Coronavirus Disease 2019 (COVID-19) pandemic has been one of the greatest public health threat that has ever been recorded in many countries [1]. By the time of this study, it had resulted in more than 5 million deaths worldwide, collapsed health systems and disturbed livelihoods [2]. The Sub-Saharan Africa recorded 3,563,825 cases with 88,274 deaths by 6 June 2021 [3]. The continent’s case fatality rate stood at 2.5% against the global average of 4.8%, as of July 2021 [4].
Zambia reported the first COVID-19 case in March 2020 and had recorded 325,857 cases with 4,006 deaths, as of June 2022 [5]. The most common symptoms of COVID-19 are fever, cold, cough, back pain, breathing problems and pneumonia in severe cases [6]. Prevention strategies of COVID-19 comprise of restrictive measures such as social distancing, masking up, isolation, hand washing and vaccination while in some countries there has been complete lockdowns. These preventive interventions are all aimed at preventing the further spread of the virus to uninfected individuals and communities [7].
The collaborative efforts by scientists led to the development of several vaccines, with the first available COVID-19 vaccine having 95% efficacy and a good safety profile announced in the press by Pfizer-BioNTech in November 2020, raising the hope of ending the pandemic [8]. Furthermore, vaccines have been seen as a cost-effective health measure for disease prevention because they are developed to reduce the mortality and morbidity rate of diseases [9]. The COVID-19 vaccines are important in developing antibodies and thus put the virus’ spread into decline [10].
The motivation to accept the COVID-19 vaccines has varied considerably across countries over the course of the pandemic. Factors such as knowledge levels about the vaccines, conflicting views, bad experience, the belief that God protects against illness and environmental factors, significantly contributes to the uptake of vaccines as reported by Cooper et al. (2021), including rumours and conspiracy theories [9,10]. Furthermore, vaccine hesitancy also depend on the belief in the vaccine and its safety, the trust placed in the health systems, fear of developing serious side effects, health conditions and lack of validation by health care professionals [10].
Scaling up and implementation of COVID-19 vaccination programs have received much attention in most low and middle-income countries like Zambia. The Republic of Zambia, through the Ministry of Health, officially launched its COVID-19 vaccination campaign on 14 April 2021, after receiving the first consignment of 228,000 doses of the vaccines from the COVAX facility, a global initiative representing a partnership among the World Health Organization, the Global Alliance for Vaccines and Immunization, UNICEF and the Coalition for Epidemic Preparedness Innovations, working on the equitable distribution of COVID-19 vaccines [5]. Despite the huge efforts made towards achieving a successful COVID-19 vaccination campaign in Zambia, the country remained with the lowest vaccination rate among the eligible population with only 25,644 individuals fully vaccinated as of 9 October 2022, which translated into 5.4% of the total eligible population [9].
Furthermore, the World Health Organization’s Strategic Advisory Group of Experts on Immunization reviewed vaccine hesitancy definitions and concluded in their report that vaccine hesitancy is complex and driven by multiple factors. Additionally, vaccine hesitancy is one of the major contributing factors that hinders the achievement of herd immunity in the targeted population [12].
Therefore, this study seeks to investigate COVID-19 vaccination barriers in five selected districts of Southern Province of Zambia namely; Namwala, Kalomo, Sinazongwe, Pemba and Monze.
METHODS
Study design, aims and setting This study used a mixed methods research design; utilizing both quantitative and qualitative research methodologies. The qualitative data was collected through the focus group discussions (FGDs) that were conducted in Namwala, Kalomo, Monze, Pemba and Sinazongwe districts of Southern province implementing the Pfizer vaccination campaign. The target participant group for these FGDs were children aged 12 -16 years old, people living with disabilities, community members, traditional and faith leaders. In addition, to assess people’s perceptions regarding the use and uptake of the COVID-19 vaccines, the study team collected quantitative data from persons aged 12 and above in all the five selected districts implementing the Pfizer vaccination campaign. The specific aims and objectives of this study included the following:
• To identify the socio - demographic factors contributing to the low COVID-19 vaccination rates among the population in selected Districts of Southern Province.
• To understand people’s knowledge about the COVID-19 vaccines.
• To investigate whether or not men and women would take the COVID-19 vaccines when presented to them.
• To investigate whether children aged 12 – 16 years old would take the COVID-19 vaccines when presented to them.
• To identify the specific myths and misconceptions that are contributing to low COVID-19 vaccination.
Sampling
This study utilized the probability sampling method to select units of measure. By definition probability sampling is a sampling method in which each element from the larger population has a known non-zero chance of selection, or they must be selected using a random sampling technique [17,18]. The research participants were drawn from all the five districts implementing the Pfizer vaccination campaign namely; Monze, Pemba, Sinazongwe, Kalomo and Namwala.
Sample Size
A total sample of 150 participants were selected from Namwala, Pemba, Kalomo, Monze and Sinazongwe Districts. The sample size was arrived at after considering the five least performing areas under health facilities with low COVID-19 vaccines uptake in each respective District. The study participants were drawn from ordinary community members, faith and traditional leaders. In terms of sample proportions, 95 participants were drawn from ordinary community members, 25 participants from faith leaders and 30 participants from traditional leaders. The Table 1 below illustrates the distribution of selected participants from each participating District
Pilot Testing of the Study Tool
The study team conducted a pilot of the survey tools on 14 to 15 July, 2022. This exercise was done to confirm the adequacy of the tool developed and ensuring that all required data was covered in the tool. The tool was also piloted to guarantee its clarity in terms of yielding reliable data from the respondents. This was also done to test field procedures and processes that were used during actual data collection. Based on the pilot results, changes required to be adjusted to the instruments were done to ensure that the questions in the research tool provided clarity and adequacy [19].
Data Collection
Mobile phones and tablets were used to collect data from the participants. All questions in the tool were scripted on the web-based platform Open Data Kit (ODK). The survey tool was uploaded to the server and downloaded to the phones and tablets. Data was collected offline and uploaded online with the availability of internet service. The focus group interviews were audio recorded in order to ensure consistency during the data analysis process. The data was collected from 18 to 22 July, 2022.
Data Analysis
After processing and cleaning, the quantitative data was exported to SPSS for further cleaning and analysis. Frequencies and distributions of all study variables by District, sex of respondents, type of respondents and other relevant disaggregation were done and presented in tables and figures. Additionally, qualitative data was analyzed using thematic analysis strategy. The research team transcribed verbatim the interview materials, coded, generated themes to form thematic networks and reaching a saturation point during the analysis process [20].
Ethical Considerations
This study was approved by the Ministry of Health through the District Health Offices in the study sites. Informed consents from all study participants were obtained before administering the tools to the study participants. The research team ensured that all the participants freely volunteered to take part in the study by signing the consent forms. Furthermore, all participants’ names remained anonymous and they were free to withdraw from the study two weeks before data analysis.
Study Variables
The explanatory variables that were explored included; district, number of people in the household, type of study participants, age, education level, occupation, presence of chronic sickness, drinking alcohol, smoking cigarettes and hearing about COVID-19. The dependent variable was vaccination against COVID-19.
Demographic data and Characteristics of Research Participants
Demographic Profile: This section presents demographic data and characteristics of research participants and includes, sex of respondents, age of respondents and level of education.
Key Findings
• The survey was administered to a sample population of 150.
• Of the total sample, 36% (N=54) were community members, people living with disability were 11.3% (N=17), 19.3% (N=29) were Faith Leaders and 16.7% (N=25) were Traditional Leaders and 16.7% (N=25) were children aged 12 – 16.
• Male participants were at 63.5%, whereas females were at 36.5%.
• The majority of research participants were aged between 45 to 54 years, accounting for 18.5%.
• The majority of the participants had attained primary education accounting for 50.6% of the respondents.
Demographic Characteristics of the Sample Population
Sex of Respondents: Interviews were administered to a total of 150 research participants. Of the total population interviewed, male research participants were 63% whereas, female participants were 37% as indicated in Table 2.
Age of Respondents: This study recruited people in the age range of 12 to 75 years or older. Investigations into the age range of participants revealed that most research participants were aged between 45 to 54 years, accounting for 18.5% of the total sample. These were followed by people aged between 12 to 16 years, accounting for 17% of the sample. The least age range to form part of the sample were participants aged 75 years or older at 4.1% as shown in Table 3.
Type of Respondents: This study enrolled a total of 150 participants, out of which 96 were community members representing 64.4% of the sample, 29 were faith leaders accounting for 19.5% whereas, traditional leaders were 24, representing 16.1% of the total sample (Table 4).
Level of Education: The study revealed that most participants had attained primary education at 50.7%. There were also high numbers of research participants that had reached the secondary level of education at 36.6%. Results further showed that 6% had reached tertiary level while 6.7% did not have any form of education as illustrated in Table 5.
Type of Religion: The study investigated the type of church that the research participants attended in order to ascertain the type of religion practised within their households. The table below showed that majority of selected participants were Protestants who accounted for 74.4%. The least attended churches were found to be Pentecostal and Roman Catholics at 6.9% and 7% respectively (Table 6).
Occupation: The table below illustrates the occupation of the respondents, it revealed that majority of the participants were in informal occupation accounting for 92% (Table 7).
RESULTS
Awareness and knowledge about COVID-19 and COVID-19 vaccines
This section presents the study’s findings about people’s awareness levels of the COVID-19 and the vaccines, including the usage and uptake of the COVID-19 vaccines in Zambia.
Key Findings:
• 99.2% of the study population was aware of or knew about the COVID-19.
• Media (television, radio and newspapers) accounted for the primary sources of information for COVID-19 at 45.6 %.
• 99.5 % of the respondents indicated that they had heard about the COVID-19 vaccines.
• 33.8% of the respondents stated that they had heard about the COVID-19 vaccines from media sources (television, radio and newspapers).
• The least source of information for COVID-19 vaccines was social media at 8.4%.
• Health workers were the most trusted source of information for COVID-19 and COVID-19 vaccines and accounted for 89.1%.
• 7.8% of the participants indicated that they trusted media sources (television, radio and newspapers) as credible sources of information for COVID-19 and COVID-19 vaccines.
• Social media and friends scored very low as credible sources of information for COVID-19 and COVID-19 vaccines, accounting for 1.2% and 2.6% respectively.
Knowledge and awareness levels about the COVID-19
To assess people’s knowledge and awareness levels of the COVID-19, respondents were asked if they had heard any information about the COVID-19. The finding across all the five districts indicated that the information about COVID-19 had become almost universal in Zambia. Furthermore, the results showed that 149 (99.2%) out of 150 respondents interviewed mentioned that they had heard information about the COVID-19 however, only one respondent accounting for 0.8%, indicated that he had not listened to any information regarding the COVID-19 (Figure 1).
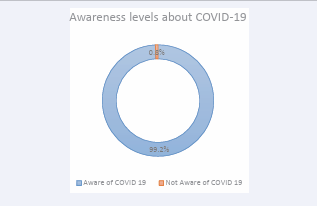
Figure 1: Awareness levels about COVID-19
Additionally, the most common sources of information about COVID-19 was health workers at 61.8%, media (television, radio, newspapers) at 45.6% and awareness campaigns at 33.7% in all the five Districts however, social media (facebook, twitter etc.) was the least common source of information at 7.7% followed by friends at 12.1% as illustrated in Figure 2.
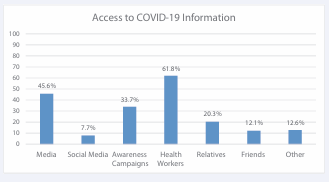
Figure 2: Access to COVID-19 Information
Knowledge about the COVID-19 Vaccines
To assess the levels of awareness about the COVID-19 vaccines, respondents were asked if they had heard about the COVID-19 vaccines. The study showed that 99.5% of the participants had heard about the COVID-19 vaccines. Furthermore, 81.3% of the respondents reported having heard about COVID-19 vaccines from health workers. The minor source of information for the COVID-19 vaccines was found to be social media, with only 8.4% of the interviewed population reporting that they heard about the COVID-19 vaccines from social media (Figure 3).
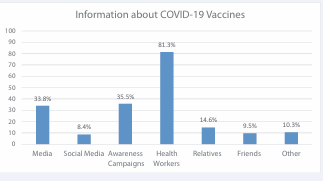
Figure 3: Information about COVID-19 vaccines
This study also presents the most and least trusted sources of information for COVID-19 and COVID-19 vaccines according to the participants (Figure 4).
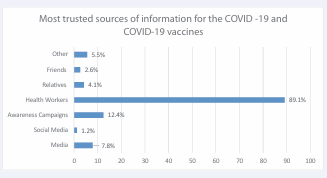
Figure 4: Most trusted sources of information for the COVID-19 and COVID-19 vaccines
Perceptions and uptake of the COVID-19 vaccines
The table below demonstrates the study findings on whether or not people would take the COVID-19 vaccines when presented to them:
Key Findings:
• 67.7% of respondents indicated that the COVID-19 vaccines were good for them.
• More males at 40% indicated that the COVID-19 vaccines were good for them compared to 26.7% of their female counterparts.
• 36.7% of the population that had attained primary education affirmed that the COVID-19 vaccines were good for them.
• The majority (67.7%) of respondents indicated that they would be willing to take the COVID-19 vaccines.
Perceptions about the COVID-19 Vaccines
To understand people’s perceptions about the COVID-19 vaccines, respondents were asked whether the COVID-19 vaccines were good for them or not. The results indicated that most of the respondents accounting for 67.7% affirmed that the COVID-19 vaccines were good for them. However, 25.8% of the respondents did not know whether the COVID-9 vaccines were good for them or not whereas, 6.5% of the respondents indicated that the COVID-19 vaccines were not good for them (Table 8).
Additionally, the perceptions regarding the COVID-19 vaccines were disaggregated by District in order to fully understand the different perceptions according to the participants. The findings when compared across the Districts revealed that Monze, Pemba and Sinazongwe had the highest COVID-19 vaccines acceptance rate while Kalomo had the least (Table 9).
Furthermore, people’s perceptions regarding the COVID-19 vaccines were disaggregated into the sex of respondents to determine different perceptions among males and females. The study showed more males than females affirming that the COVID-19 vaccines were good for them, accounting for 40% of males compared to 26.7% of female respondents (Table 10).
In addition, another analysis was done to determine whether or not the level of education contributed to the way people perceived the COVID-19 vaccines. For this analysis, responses of whether the COVID-19 vaccines were viewed as good or bad were disaggregated among people that had attained various levels of education. The results showed that there were significant differences in responses among different levels of education. It was observed that among the population that had reached primary education, 36.7% affirmed that the COVID-19 vaccines were good for them. Furthermore, 23.3% of the people that had attained secondary education confirmed that the COVID-19 vaccines were good for them however, none of the respondents who reached tertiary education indicated that the COVID-19 vaccines were good for them. Finally, of those who did not attain any form of education, 6.7% said that the COVID-19 vaccines were good for them (Table 11).
Willingness to take the COVID-19 Vaccines
The research participants were asked a question of “Are you planning to get vaccinated against COVID-19?”. The majority of the participants which accounted for 70% indicated that they were willing to take the COVID-19 vaccines if presented to them (Table 12).
Furthermore, a similar analysis was done to check the willingness of participants per district. The results showed that Monze, Pemba and Sinazongwe Districts had the highest number of participants who were willing to take the COVID-19 vaccines at 15.2% while Namwala District had the least of the respondents that were willing to be vaccinated against COVID-19 at 9.1% (Table 13).
The proportion of participants that expressed willingness to take the COVID-19 vaccines if presented to them was higher at 70%. The male participants that expressed willingness to take the COVID-19 vaccines were at 43.3% while female participants accounted for 26.7% (Table 14).
Additionally, the proportion of participants that had attained primary education was the highest in indicating that they would be willing to take the COVID-19 vaccines and accounted for 41.9% of the total responses. This was followed by respondents that had attained secondary education at 19.4% and those that had not attained any level of education were at 6.5% however, all participants that had attained tertiary education were not willing to take the COVID-19 vaccines (Table 15).
Factors contributing to the refusal to take COVID-19 Vaccines
This study investigated the reasons why the participants refused to take the COVID-19 vaccines and observed that 19.8% of the total participants did not take the COVID-19 vaccines because of the belief that the vaccines are harmful to humans. Furthermore, 14.1 % of the respondents reported that they did not take the COVID-19 vaccines because of personal choice. However, a multivariate logistic regression of factors associated with people getting vaccinated against COVID-19 indicated that number of people in the household, smoking cigarettes, drinking alcohol and heard of COVID-19 were not associated with people getting vaccinated against COVID-19 (Table 16).
Misconceptions and myths about COVID-19 and COVID-19 vaccines
The study also conducted the focus group discussions (FGDs) in all the five districts with the aim of identifying factors that contributed to low uptake of COVID-19 vaccines. During the FGDs in Sinazongwe District, lack of information, education and communication (I.E.C) materials and misconceptions were clearly noted:
“The COVID-19 vaccines were developed to eliminate the African countries after 2 years of being vaccinated”
The above stated misconception was one of the reasons why some people were not vaccinated in Sinazongwe District. Similar findings were also observed in Namwala District as some people avoided getting vaccinated because they believed that the COVID-19 vaccines were meant to reduce the population especially Africans. One of the respondents during the FGDs in Sinazongwe District said:
‘’The vaccines do not protect you from anything, even when you are vaccinated you can still get COVID-19 and it can still kill so why stressing getting the vaccines’’
According to the FGDs in Monze District, it came to light that some people believed that the COVID-19 vaccines were the mark of the beast and they did not understand why it’s the only disease which was given a card after vaccination. Similar observations were also noted in Kalomo District. In addition, some religious organizations considered administration of COVID-19 vaccines highly discouraged.
Several participants from Mawaya in Kalomo District said:
“People believe that it is demonic and therefore believe it should not be taken, this therefore makes community members shun away from taking the COVID-19 vaccines.”
Again, a similar response was given by community members from Macraymond in Kalomo District stating that:
“Some religious denominations such as Zion believe in natural healing and as such you would find them using salt as a source of healing.”
During the focus group discussions in Pemba District, it was believed that the COVID -19 vaccines initiates one into Satanism. A lady in Pemba District echoed that:
“It is an automatic way of initiating community members into Satanism”
Furthermore, lack of trust in the COVID-19 vaccines was another reason why some people refused to be vaccinated. This observation was confirmed by another participant from Macraymond in Kalomo District who said that:
“People do not trust the COVID-19 vaccines, they believe that they will produce side effects in future.’’
A similar response was also given by participants from Sinazongwe District which stated that:
“Some people prefer oral medications as opposed to injections because they believe that injections come with possible side effects.”
The other participants in the two FGDs added that there was a belief that somebody can be healed from COVID-19 naturally just by self-isolation.
DISCUSSION
The findings of this study revealed that a lot of community members had major myths and misconceptions about COVID-19 and COVID-19 vaccines in Kalomo, Pemba, Monze, Sinazongwe and Namwala Districts hence, refused to get vaccinated against the disease. This is evidenced when one participant associated the COVID-19 vaccines injection to a process of initiation into Satanism. In addition, other participants referred to the COVID-19 vaccines as demonic and that they were developed to eliminate Africans. These findings are consistent to a similar study conducted by Cooper et al. (2021), which acknowledged that there was over 90% global vaccines hesitancy among the 194 member states of the United Nations Children’s Fund, including in countries across the World Health Organization regions.
However, the results of this study also indicated that most of the respondents accounting for 67.7% affirmed that the COVID-19 vaccines were good for them. Furthermore, 25.8% of the respondents did not know whether the COVID-9 vaccines were good for them or not whereas, 6.5% of the respondents indicated that the COVID-19 vaccines were not good for them. Therefore, these findings demonstrates the need for provision of increased health promotion activities by health care professionals to the COVID-19 vaccines eligible population in order to improve the vaccination rate [13]. Moreover, health care workers were observed to be the most trusted and reliable source of information for COVID-19 vaccines by community members.
In addition, the results of the current study showed that there were significant differences in responses among different levels of education. It was observed that among the population that had reached primary education, 36.7% affirmed that the COVID-19 vaccines were good for them. Furthermore, 23.3% of the people that had attained secondary education confirmed that the COVID-19 vaccines were good for them however, none of the respondents who reached tertiary education indicated that the COVID-19 vaccines were good for them but those who did not attain any form of education, 6.7% said that the COVID-19 vaccines were good for them. In contrast, these findings differ from a study that was conducted in the United States of America that found that COVID-19 vaccination acceptance rate increased with increased levels of education [11]. Nevertheless, the majority of the participants which accounted for 70% indicated that they were willing to take the COVID-19 vaccines if presented to them.
Again, the proportion of participants that had attained primary education was the highest in indicating that they would be willing to take the COVID-19 vaccines and accounted for 41.9% of the total responses. This was followed by respondents that had attained secondary education at 19.4% and those that had not attained any level of education were at 6.5% however, all participants that had attained tertiary education were not willing to take the COVID-19 vaccines. Therefore, this meant that people with tertiary education formed the larger portion of those that refused to get vaccinated against COVID-19 hence, health promotion interventions should target this category in order to dispel the myths and misconceptions surrounding the COVID-19 vaccines [15].
Likewise, the results of this study further showed that Monze, Pemba and Sinazongwe Districts had the highest number of participants who were willing to take the COVID-19 vaccines at 15.2% while Namwala District had the least of the respondents that were willing to be vaccinated against COVID-19 at 9.1%. Furthermore, the findings of this study revealed that Monze, Pemba and Sinazongwe Districts had the highest COVID-19 acceptance rate at 16.1% while Kalomo District had the lowest at 6.5%. Additionally, the study showed more males affirming that the COVID-19 vaccines were good for them at 40% compared with their female counterparts at 26.7%.
Interestingly, the current study investigated the reasons why the participants refused to take the COVID-19 vaccines and observed that 19.8% of the total participants did not take the COVID-19 vaccines because of the belief that the vaccines are harmful to humans. Furthermore, 14.1 % of the respondents reported that they did not take the COVID-19 vaccines because of personal choice. However, a multivariate logistic regression of factors associated with people getting vaccinated against COVID-19 indicated that number of people in the household, smoking cigarettes, drinking alcohol and heard of COVID-19 were not associated with people getting vaccinated against COVID-19. These findings are similar to another study by Sutcliffe et al. (2022), which found that COVID-19 vaccines hesitancy in Africa was attributed to lack of confidence or knowledge of the vaccines, religious beliefs, lack of perceived risks of COVID-19 and mistrust of public health institutions [5,14].
Furthermore, this study found that majority of community members did not have the trust in the COVID-19 vaccines as they believed that they would still get infected even after getting vaccinated or develop serious life threatening side effects in the near future if they got vaccinated. The other category believed in isolation, religious and natural healing by using ordinary salt in order to cure several diseases as opposed to getting vaccinated. These findings are consistent with the study by Malik et al. (2020) who suggested that health communication should reach all communities especially the most vulnerable to educate them on the safety and efficacy of the COVID-19 vaccines in order to prevent the future spread of the disease and enhance healthier lives [11,16].
Limitations of the Study
This study was limited with wider mixed methodology techniques as the researchers were not very experienced with the chosen methods. Furthermore, there was limited literature consulted on the current research topic.
RECOMMENDATIONS
The following recommendations are provided based on the findings of the current study:
1. Health care workers should disseminate safety COVID-19 vaccines messages to the targeted eligible population.
2. Health promoters should strengthen COVID-19 vaccines awareness activities in communities in order to dispel the myths and misconceptions surrounding COVID-19 vaccines.
3. The COVID-19 vaccines should be administered to eligible population as routine vaccination activity at health facilities.
4. People with tertiary education, church leaders and traditional leaders should be targeted for COVID-19 vaccination awareness activities in order to improve the COVID-19 vaccination rates in communities.
5. There is a need of conducting future studies on the safety and efficacy of COVID-19 vaccines.
IMPLICATION FOR PRACTICE
The findings of this study has the potential to influence policy makers, health managers and health care professionals to strengthen health promotion and public health interventions on COVID-19 vaccination activities in order to improve on the vaccination rates and significantly reduce the spread of COVID-19 in communities.
CONCLUSION
The findings of this study revealed substantial evidence that a lot of myths and misconceptions on COVID-19 vaccines do exist in communities with the major ones being that the COVID-19 vaccines are demonic and that they were developed to eliminate the African population. Therefore, this presents an excellent opportunity for policy makers and health promoters to strengthen health promotion and public health interventions on COVID-19 vaccination activities in order to dispel these myths and misconceptions and thereby, increase the COVID-19 vaccination rates among the eligible population in communities.
ACKNOWLEDGEMENTS
The authors would like to thank all the participants for their valuable contributions in this study and indeed, the Ministry of Health for allowing the research team to freely access the study sites.
Authors’ Contributions
SM formulated the research topic, conducted literature review, participated in interviews, analyzed and interpreted data and drafted the manuscript. MC participated in interviews, analyzed and interpreted data. All authors critically reviewed and approved the final version of the manuscript.
Availability of Data and Materials
The anonymized datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by Ministry of Health and written consent was received from all the participants.
REFERENCES
3. World Health Organization. COVID-19 Weekly Epidemiological Update; Edition 43.
9. Ndwandwe D, Wiysonge CS. COVID-19 Vaccines. Curr Opin Immunol. 2021; 71: 111-116.
14. Troiano G, Nardi A. Vaccine hesitancy in the era of COVID-19. Public Health. 2021; 194: 245-251.
20. Fan J, Han F, Liu H. Challenges of big data analysis. National Science Review. 2014; 1: 293-314.






































































































































