Assessment of Dose to Glandular Tissue of Patients Undergoing Mammography Examinations
- 1. Department of Medical Physics, University of Ghana, Ghana
- 2. Radiological and Medical Sciences Research Institute, Ghana Atomic Energy Commission, Ghana
- 3. Supreme Specialist Centre, Korle-Bu Teaching Hospital, Ghana
Abstract
Assessment of Dose to the Glandular tissue of patients undergoing digital mammography examination from two Computed Radiology systems has been undertaken. A total of 81 patient data was used for the study. Basic Quality Control tests were first performed on the equipment using a Piranha Quality Control kit. Patients were put into two groups of 40-49years and 50-64 years and under different breast thicknesses. All calculated Mean Glandular Doses under the age groups 40–49 years and 50–64 years from facility A fell under the acceptable levels given by the European Protocol for the Quality Control of Physical and Technical Aspects of Mammography Screening. From the results it was observed that, patients with a compressed breast thickness of 32 mm under the age 40-49 years from facility B recorded a calculated Mean Glandular Dose of 1.55 mGy which was 3.27% above the acceptable level of 1.5 mGy. Furthermore, patient with compressed breast thickness of 60mm under the age 50 – 64 years recorded a calculated MGD of 2.51 mGy which was above the achievable level by 4.48% but was well below the acceptable level. The results of Quality Control tests indicated that the two Mammography units used for this study were functioning within the internationally acceptable performance criteria and are recommended for further examinations.
Keywords
• Mammography
• Mean glandular dose
• Breast cancer
• Quality control
• Computed radiology
Citation
Pwamang C, Sosu E, Schandorf C, Boadu M, Hewlett V (2016) Assessment of Dose to Glandular Tissue of Patients Undergoing Mammography Examinations.. J Radiol Radiat Ther 4(2): 1062.
ABBREVIATIONS
MGD: Mean Glandular Dose; PMMA: Poly Methyl Methacrylate; CBT: Compressed Breast Thickness
INTRODUCTION
Cancer is a disease caused by an uncontrolled division of abnormal cells in any part of the body. Metastases are the major cause of death from cancer [1]. Cancer is the second most common cause of death in the US and accounts for nearly 1 of every 4 deaths [2]. The most commonly diagnosed cancers worldwide are lung, breast, and colorectal cancers. It is reported that, 14.1 million new cancer cases and 8.2 million cancer-related deaths occurred in 2012, compared with 12.7 million and 7.6 million, respectively, in 2008 [3].
Breast cancer is reported as one of the first courses of women mortality [4]. It constitutes 21% of all cancer cases and ranks third among cancer types. It is the second highest cause of cancer deaths in females after cervix uteri cancer. There is no known cause of breast cancer neither is there an effective method of preventing it. In the pre-invasive stage of breast cancer, the cancer cells are confined to the breast ducts system. This is followed by the invasive stage where cancerous cells infiltrate into the surrounding tissues including the lymph nodes [5].
Mammography is nowadays the most accurate and effective means of early detection of breast cancer [6]. However, the potential risk of radiation-induced carcinogenesis is also increased with such diagnosis, thus making the assessment of breast dose very important [7]. Digital mammography is one of the two types of mammography systems. It uses X-rays to image the breast as in screen/film mammography. It has a detector that converts the X-rays to digital images and they are stored directly in a computer [8]. X-rays are ionizing radiations and can have adverse effects (Stochastic effects) on the human body. The active and radiosensitive glandular tissue has Tissue-Weighting Factor of 0.12, which indicate that the breast is one of the most radiosensitive organs in the body [9]. For this reason optimum equipment performance and dose management per mammogram is essential and cannot be overemphasized. The main objective of this study is to assess the radiation dose to patients undergoing digital mammography to form the basis for developing imaging protocols to ensure effective optimization of radiation protection in digital mammography practices. The specific objectives are: To estimate the Mean Glandular Dose (MGD) to patients using the Entrance Surface Air Kerma (ESAK) without back scatter, and to assess the performance of each mammography unit under my study, by performing Quality Control (QC) tests on them. The QC tests performed on the two facilities included kVp accuracy and repeatability, output repeatability and linearity, as well as Half Value layer (HVL).
MATERIALS AND METHODS
Subject
81 women undergoing mammography examination for both diagnostic (45 women) or screening (36 women) purposes were used for the study. Patients were put into two groups of 40-49years and 50-64 years and under different compressed breast thicknesses of 32mm, 45mm, and 53mm, 60mm, 75mm and 90mm. A data sheet was designed to collect data which included age, kVp, mAs and compressed breast thickness for each imaged breast. The breast thickness was simulator with the Polymethylmethacrylate (PMMA) and a spacer under the same exposure parameters as recorded after patient exposure to determine the incident air kerma and hence the Mean Glandular dose.
Theory
The MGD values are based on measurements of ESAK (Entrance Surface Air Kerma) and HVL (Half Value Layer). The exposure factors (CBT, kVp, mAs, and age) for a number of patients were recorded, and the exposure factors simulated for some selected breast thicknesses using PMMA slabs. To do the measurements correctly and according to standards, the radiation detector (Piranha) was placed directly below the compression paddle; this mimics the exposure of the fully automatic mode in manual mode using the same exposure factors resulted from the previously exposed patients, in order to obtain the ESAK. MGD was then calculated for various breast thicknesses and composition equivalent to the thickness of PMMA by using the equation (1):
MGD = K.g.c.s (1)
where K is the incident air kerma (without back scatter) at the upper surface of the breast, g is the incident air kerma to mean glandular dose conversion factor (g-factor), c corrects for any difference in breast composition from 50% glandularity and the factor s corrects for any difference due to the use of a different X-ray spectrum. The conversion factors g, c and s are extrapolated from the work of Dance et al 2000, 2009, and 2011 [12,13].
To get the ESAK from the exposure recorded from the piranha, the distance was first corrected to attain the final radiation intensity to the surface of the breast. This was done using the inverse square law equation; equation (2).
(2)
Where, is the initial intensity of radiation,
is the final radiation intensity,
is the initial distance, and
is the final distance.
This was necessary because, the distance at which the detector was measuring the incident radiation was different from the distance at which the various simulated breast thicknesses received the incident radiation. Hence was calculated. After that, the output was calculated using equation (3);
(3)
From equation (3) the output is gotten in mGy/mAs. ESAK was then calculated by dividing the output (mGy/mAs) by the recorded mAs;
(4)
This gave the ESAK in mGy. The g and c factors for the measured half-value layers were interpolated from the compiled data for age groups 40-49 years and 50-64 years, according to the breast thickness, and the s factor according to the anode/filter combination used. Finally, an inter unit comparison of the results of calculated ESAK and MGDs was made. The results were also compared to the International Atomic Energy Agency (IAEA) and European Quality Control of Physical and Technical Aspects of Mammography Screening.
Material
Two (2) Digital Mammography equipment with specifications presented in Table (1),PMMA (Polymethylmethacrylate), also known as Perspex, Piranha Quality Control Kit, Aluminum sheets, measuring rule, Microsoft Excel and Ocean software were used to collect data for Quality Control test and Mean glandular dose assessment.
|
Table 1: Specifications of mammography equipment used. |
||
|
CHARACTERISTIC |
A |
B |
|
Type of equipment |
CR |
CR |
|
Manufacturer |
Philips |
GE |
|
Model |
Mammo Diagnost AR |
Alpha RT |
|
Year of make |
2013 |
2012 |
|
Mode of operation |
AEC/Manual |
AEC/Manual |
|
Anode/filter combination |
Mo/Rh |
Mo/Rh |
|
kVp range |
20-35 |
23-35 |
|
mAs range |
1-600 |
0.004-450 |
|
Abbreviations: A,B: Mammography Facility; CR: Computed Radiology; GE: General Electric; AEC: Automatic Exposure Control; Mo: Molybdenum; Rh: Rhodium; kVp: Kilo voltage; mAs: Milli Ampere Seconds |
||
Method
Quality control test and assessment of mean glandular dose were undertaken using the International Atomic Energy Agency Human Health Series 2 and 17protocol [10,11] and the European Quality Control of Physical and Technical Aspects of Mammography Screening [9] respectively.
RESULTS
The results of kVp accuracy and repeatability, output linearity and repeatability, half value layer, and automatic exposure control measurements are presented in Table (2).
|
Table 2: Mammography equipment performance tests results. |
|||
|
QUALITY CONTROL TEST (Acceptable range) |
A |
B |
COMMENTS (PASS/FAIL) |
|
kVp accuracy ( ± 5%) |
-4.6 |
0.3 |
Pass |
|
kVp Repeatability (COV ≤ 2%) |
1.71 |
0.3 |
Pass |
|
HVL (mmAl) (kVp/100+0.03 ≤ HVL ≤ kVp/100+c) |
0.35 |
0.31 |
Pass |
|
Output repeatability (COV ≤ 5%) |
0.20 |
0.30 |
Pass |
|
Output Linearity (<10%) |
-0.20 |
0.22 |
Pass |
|
AEC repeatability ( ≤ 5%) |
0.74 |
1.94 |
Pass |
|
Abbreviations: A,B: Mammography Facility; CR: Computed Radiology; GE: General Electric; AEC: Automatic Exposure Control; kVp: Kilo Voltage, mmAl: Millimeters of Aluminum; COV: Co-efficient of Variation |
|||
The kVp accuracy for facility A was -4.6% and B had a kVp accuracy of 0.30%, which falls within the acceptable range of ± 5%. All two facilities recorded kVp repeatability as 1.71%, and 0.30% respectively, which also falls within the normal range of ≤ 2%. The HVL measured on the A was 0.35mmAl, and B was 0.31mmAl. Facility A recorded an output repeatability of 0.20% and a linearity of -0.20μGy/mAs, and that of B was 0.30% and 0.22μGy/mAs respectively. Calculated values from the Automatic Exposure Control assessment from the two facilities, (0.74%, and 1.94% for A and B respectively),were within the acceptable levels of ≤ 5%. Table (3) shows all the calculated MGDs under the age groups 40–49 years and 50–64 years.
|
Table 3: Comparison between the calculated Mean Glandular Dose and Standard Mean Glandular Dose (European protocol). |
|||||||
|
Thickness of PMMA (mm) |
Thickness of equivalent breast (mm) |
Maximum MGD to equivalent breast |
A |
B |
|||
|
40–49years |
50–64years |
40–49years |
50–64years |
40–49years |
50–64years |
||
|
Acceptable level (mGy) |
Achievable level (mGy) |
Calculated MGD (mGy) |
Calculated MGD (mGy) |
Calculated MGD (mGy) |
Calculated MGD (mGy) |
||
|
30 |
32 |
<1.5 |
<1.0 |
0.51 |
- |
1.55 |
- |
|
40 |
45 |
<2.0 |
<1.6 |
0.64 |
0.52 |
1.72 |
- |
|
45 |
53 |
<2.5 |
<2.0 |
- |
- |
1.96 |
- |
|
50 |
60 |
<3.0 |
<2.4 |
0.99 |
0.85 |
2.06 |
2.51 |
|
60 |
75 |
<4.5 |
<3.6 |
1.11 |
1.08 |
- |
2.94 |
|
70 |
90 |
<6.5 |
<5.1 |
1.50 |
1.27 |
- |
3.30 |
|
Abbreviations: mm: Millimeters; mGy: Milligray; MGD: Mean Glandular Dose; PMMA: Polymethylmethacrylate; (-) in table means no patient was received at the facility for that age category |
|||||||
DISCUSSION
This is the first study to undertake quality control assessment and estimation of Mean Glandular Dose at the two (2) facilities to form basis for developing imaging protocols, which will ensure effective optimisation of radiation protection in digital mammography practice. Results from the study indicated that all quality control tests performed on all the two mammography systems which included; kVp repeatability and accuracy test, Output repeatability and linearity test, Half Value Layer measurement, as well as Automatic Exposure Control repeatability measurement were all within the acceptable levels. Calculated MGDs under the age groups 40–49 years and 50–64 years from facility a fell under the acceptable levels given by the European Protocol for the Quality Control of Physical and Technical Aspects of Mammography Screening. From the results it was observed that, patients with a compressed breast thickness of 32 mm under the age 40-49 years from facility B recorded a calculated MGD of 1.55 mGy which was 3.27% above the acceptable level of 1.5 mGy. Furthermore, patient with compressed breast thickness of 60mm under the age 50-64 years recorded a calculated MGD of 2.51 mGy which was above the achievable level by 4.48% but was well below the acceptable level. Figure (1) and (2) show graphs of calculated MDG values versus compressed breast thickness compared with internal standards.
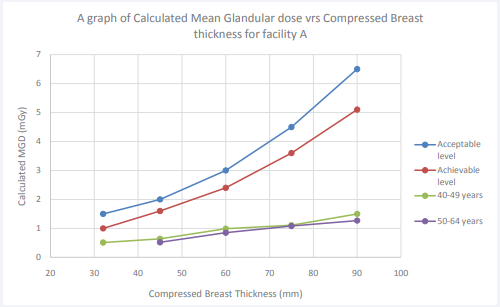
Figure 1: A graph of Calculated Mean Glandular dose vrs Compressed Breast thickness for facility A compared with European Quality Control of Physical and Technical Aspects of Mammography Screening protocol.
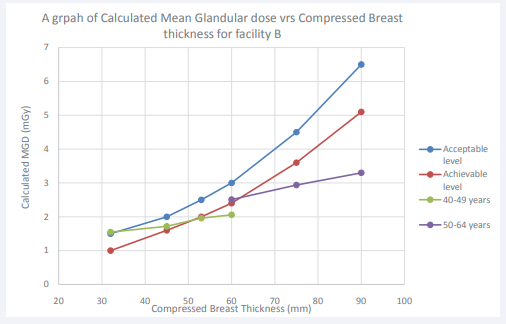
Figure 2: A graph of Calculated Mean Glandular dose vrs Compressed Breast thickness for facility B compared with European Quality Control of Physical and Technical Aspects of Mammography Screening protocol.
CONCLUSION
Basic quality control on two Computed Radiology (CR) mammography system and radiation dose to patients undergoing digital has been undertaken. Results from the quality control test show that the systems are functioning well. Calculated mean glandular dose of patients compares well with International Standard. The systems are recommended for Mammography practice.
ACKNOWLEDGEMENTS
This work was made possible through the Grace of the Almighty God. We also want to acknowledge the efforts of Theresah Gorman and Patience Aku - Sika Agbenyo both radiographers from The Trust Hospital and Supreme Diagnostic Centre both in Accra, Ghana.
REFERENCES
- World Health Organization. Cancer. 2015; 1-4
- Crosta Peter. Cancer; Facts, types and causes. 2015.
- Thomas Albert. Latest world cancer statistics, Global cancer burden rises to 14.1 million new cases in 2012: Marked increase in breast cancers must be addressed. International Agency for Research on cancer. WHO. 2013; 1-3.
- Smith RA. Epidemiology of breast cancer, in a Categorical Course in Physics. Imaging considerations and Medical Physics responsibilities. 1991.
- Wambani JS, Korir GK, Bwonya MN, Korir IK. Assessment of patient doses during mammography practice at Kenyatta National Hospital. East Africa Medical J. 2011; 88: 368-376.
- Tomal A, Poletti ME, Caldas LVE. Evaluation of subject contrast and normalized average glandular dose by semi-analytical models. Applied Radiation and Isotope. 2010; 68: 755-759.
- Donga L, Chua TC, Lee JS, Lanc GY, Wua TH, Yeh YH, et al. Estimation of mean-glandular dose from monitoring breast entrance skin air kerma using a high sensitivity metal oxide Semiconductor field effect transistor (MOSFET) dosimeter system in mammography. Appl Radiat Isot. 2002; 57: 791-799.
- Breastcancer.org. Mammography Technique and Types. 2013.
- European Nuclear Society. Tissue Weighting Factor. 2015.
- International Atomic Energy Agency. Quality Assurance Program for Screen Film Mammography. IAEA Human Health Series. 2009; 2: 125-130.
- International Atomic Energy Agency. Quality Assurance Program for Digital Mammography. IAEA Human Health. 2011; 17: 109-114.
- Dance DR, Skinner CL, Young KC, Beckett JR, Kotre CJ. Additional factors for the estimation of mean glandular breast dose using the UK mammography dosimetry protocol. Phys Med Biol. 2000; 45: 3225-3240.
- Dance DR. Monte Carlo calculation of conversion factors for the estimation of mean glandular breast dose. Phys Med Biol. 1990; 35: 1211-1219.







































































































































{kind=link}