Imaging Correlation of a Carotid Embolus in Central Retinal Artery Occlusion (CRAO)
- 1. Department of Ophthalmology and Visual Sciences University of Utah, USA
- 2. Department of Radiology, University of Utah, USA
Abstract
Background: To highlight the utility of B-scan ultrasound in the diagnosis of a CRAO.
Case Presentation: A 64-year-old Caucasian male with a history of hypertension, presented to triage clinic for sudden vision loss in his right eye starting 36 hours previously. CTA showed a calcified plaque with an adjacent soft component in the right internal carotid artery. MRA showed intra-plaque hemorrhage without ulceration which was evidence against this as a source of emboli. B-scan ultrasound of the right eye showed a central retinal artery focus of increased echogenicity, consistent with an embolus. Ultimately, the true etiology of the CRAO was confirmed on B-scan ultrasound.
Conclusions: B-scan ultrasound can be a valuable, non-invasive diagnostic modality in determining the underlying etiology of a CRAO.
Keywords
• CRAO- Central Retinal Artery Occlusion
• B-Scan Ultrasound
• Carotid Embolus
• Ischemia
CITATION
Patil A, Wiggins R, Harrie R (2023) Imaging Correlation of a Carotid Embolus in Central Retinal Artery Occlusion (CRAO). J Radiol Radiat Ther 11(2): 1101.
ABBREVIATIONS
CRAO: Central Retinal Artery Occlusion; OD: Right Eye; OS: Left Eye; CTA: Computed Tomography Angiography; MRA: Magnetic Resonance Angiography; DWI-MRI: Diffusion Weighted Imaging-Magnetic Resonance Imaging.
INTRODUCTION
Central retinal artery occlusion (CRAO) is an ophthalmic emergency as it is an ocular presentation of a cerebral stroke [1]. Patients who are found to have a CRAO, typically suffer from profound visual loss permanently hindering their quality of life [2]. The ocular findings signify end-organ ischemia typically from underlying atherosclerotic disease. These same risk factors can then predispose a patient to future cerebral strokes and cardiovascular events. The most common cause of a CRAO in an older patient is cholesterol embolism typically from underlying carotid artery disease [3]. Atrial fibrillation should be ruled- out with cardiac monitoring if a carotid source isn’t identified. Giant cell arteritis should always be considered in patients over 70 and should be tested with an erythrocyte sedimentation rate and C-reactive protein. Patients younger than 50 should have a hypercoagulable workup including antiphospholipid antibody syndrome, autoimmune conditions, inflammatory disorders, and other hypercoagulable states [4]. Patients in this age group should also undergo a transesophageal echocardiogram with a bubble test to look for a cardiac valvular source of emboli or a septal defect.
Classic diagnostic modalities including cerebral vessel imaging and echocardiography cannot always identify the embolic source. This case report aims to highlight the utility of ocular B-scan ultrasound as a first line test to rule-out an embolus as the cause of CRAO.
CASE PRESENTATION
A 64-year-old man with a past medical history of mild hemophilia A and essential hypertension presented to ophthalmology triage clinic with the sudden onset of painless vision loss in his right eye that started 36 hours prior to being seen. He stated that prior to this, he had a few episodes of transient vision loss in the same eye that would last about a minute at a time. He denied any double vision, headaches, scalp tenderness or associated jaw pain. He has no prior surgical history. He endorses a 14-pack year smoking history, though he quit about 35 years ago. He otherwise consumes alcohol a few times a week. Prior to presentation, he was taking lisinopril for blood pressure management.
His examination was notable for visual acuity of light perception in his right eye (OD) with a positive relative afferent pupil defect and 20/20 visual acuity in his left eye (OS). His intraocular pressures and anterior segment slit lamp examination were normal in both eyes. His fundus exam OD was notable for a classic cherry-red fovea surrounded by 360-degrees of retinal whitening. He then underwent an emergent stroke workup. Computed tomography angiography (CTA) showed a calcified plaque with an adjacent soft component in the right internal carotid artery (Figure 1 A,B).
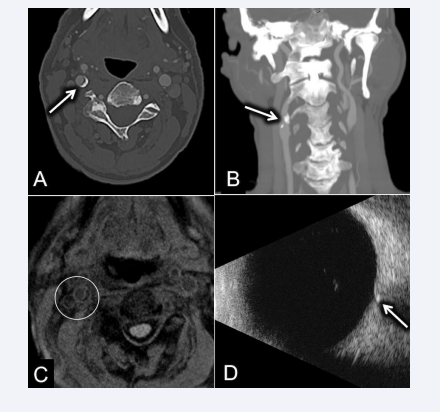
Figure 1 A: Axial section of a CTA scan showing a calcified plaque in the right internal carotid artery (highlighted by the white arrow). B: Sagittal section of a CTA scan showing the same calcified plaque in the right internal carotid artery (highlighted by the white arrow). C: MRA showed no intra-plaque hemorrhage which was evidence against ulceration as a source of emboli (highlighted by the white circle). B-scan ultrasound of the right eye showed a central retinal artery focus of increased echogenicity, consistent with an embolus (highlighted by the white arrow).
Magnetic resonance angiography (MRA) showed no intra-plaque hemorrhage which was evidence against plaque ulceration as a source of emboli (Figure 1C). B-scan ultrasound of the right eye showed a retrolaminar central retinal artery focus of increased echogenicity, consistent with a cholesterol embolus (Figure 1D). Ultimately, the true etiology of the CRAO was confirmed on B-scan ultrasound.
DISCUSSION
This case of CRAO, an ocular emergency, highlights the utility of B-scan ultrasound in allowing for rapid diagnosis and accurate identification of the underlying pathophysiology of an acute retinal stroke. Similar to this case presentation, 80% of CRAO patients will present with sudden profound vision loss in one eye with a visual acuity of 20/400 or worse [2]. Many of these patients have preceding transient vision loss episodes prior to this catastrophic event, which are representative of transient ischemic attacks. This classic presentation should immediately raise suspicion of an acute stroke and therefore prompt rapid diagnosis, workup, and treatment. Unfortunately, there is often a delay in diagnosis secondary to patients’ time of presentation and challenges with obtaining appropriate ophthalmic funduscopic evaluation emergently [5]. Point of care ultrasound may be of greater utility in aiding the diagnosis, especially in a setting where access to emergent ophthalmic care and evaluation is limited [6]. Nedelman stated that the B-scan finding of the “retrobulbar spot sign” was found in 59% of their CRAO patients [7]. This finding may aid in earlier treatment with tissue plasminogen activator (tPA) and brain imaging to evaluate for other cerebral infarctions. Studies have identified that 27% to 76.4% of patient’s presenting with acute retinal ischemia were found to have acute cerebral infarctions on further imaging, specifically diffusion weighted imaging-magnetic resonance imaging (DWI-MRI) [8]. Moreover, in cases such as this one, in which the underlying etiology of the acute stroke cannot be readily identified on imaging, ocular ultrasound is an excellent tool in accurately identifying emboli as the causative source. B-scan ultrasound is a simple and rapid test that can be performed in the setting of an acute central retinal artery occlusion. This instrument is generally available in most emergency rooms and university medical centers across the United States. Although fundus fluorescein angiography (FFA) and optical coherence tomography angiography (OCT-A) would show delayed retinal arterial filling, they would not be expected to demonstrate embolic material posterior to the lamina cribrosa. To our knowledge, this is the only case report that offers a presentation of conflicting imaging evidence in identifying the causative source in acute retinal ischemia, that was then accurately identified with point of care ultrasound, specifically ocular B-scan.
ACKNOWLEDGEMENTS
Supported in part by an Unrestricted Grant from Research to Prevent Blindness, New York, NY, to the Department of Ophthalmology & Visual Sciences, University of Utah.
REFERENCES
- Varma DD, Cugati S, Lee AW, Chen CS. A review of central retinal artery occlusion: clinical presentation and management. Eye (Lond). 2013; 27: 688-697.
- Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005; 140: 376-391.
- Arruga J, Sanders MD. Ophthalmologic Findings in 70 Patients with Evidence of Retinal Embolism. Ophthalmology. 1982; 89: 1336-1347.
- Biousse V. Acute Retinal Arterial Ischemia: An Emergency Often Ignored. Am J Ophthalmol. 2014; 157: 1119-1121.
- Caja KR, Griffith KM, Roth KR, Worrilow CC, Greenberg MR, Doherty TB. Detection of Central Retinal Artery Occlusion by Point-of-Care Ultrasound in the Emergency Department: A Case Series. Cureus. 2021; 13: e16142.
- Biousse V, Nahab F, Newman NJ. Management of Acute Retinal Ischemia: Follow the Guidelines! Ophthalmology. 2018; 125: 1597-1607.
- Nedelman M, Graef M, Weinand F, Klaus-Heiko W, Kaps M, Lorenz B, et al. Retrobulbar Spot Sign Predicts Thrombolytic Treatment Effects and Etiology in Central Retinal Artery Occlusion. Stroke. 2015; 46: 2322-2324.
- https://www.aao.org/preferred-practice-pattern/retinal- ophthalmic-artery-occlusions-ppp-2016







































































































































{kind=link}