A Brief Review of Claustrophobia and Continuous Positive Airway Pressure (CPAP) Therapy for Sleep Apnea
- 1. Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, USA
Abstract
The most common treatment for OSA is CPAP, yet its effectiveness is overshadowed by significant patient adherence difficulties. Compared to a pharmacotherapy intervention (e.g., taking daily medication to manage a medical condition), CPAP requires tolerating mask, head straps, and airway pressure throughout the sleep period in addition to maintaining and cleaning the device daily. Among the many barriers to adherence reported by patients, claustrophobia related to the CPAP device is reported by about 1/3 of CPAP users. The application of psychological interventions for phobias (exposure based therapies), modified for CPAP-related claustrophobia, shows promise in reducing claustrophobia and ultimately enhancing adherence. This review describes the scope of the problem regarding claustrophobia and CPAP, presenting a theoretical framework in which to understand the development and maintenance of claustrophobia. Extant literature applying exposure based therapies to CPAP-related claustrophobia is reviewed, highlighting the need for additional research in this promising area.
Keywords
• Claustrophobia
• Patient adherence
• Sleep apnea treatment
• Positive airway pressure
• Graded exposure therapy
Citation
Leggett MK (2016) A Brief Review of Claustrophobia and Continuous Positive Airway Pressure (CPAP) Therapy for Sleep Apnea. J Sleep Med Disord 3(2): 1043.
ABBREVIATIONS
OSA: Obstructive Sleep Apnea; CPAP: Continuous Positive Airway Pressure
INTRODUCTION
Continuous positive airway pressure (CPAP) effectively eliminates sleep-related upper airway obstruction, lowers blood pressure, reduces daytime somnolence, and improves quality of life among patients with obstructive sleep apnea (OSA) [1- 3]. Despite its effectiveness, adherence to CPAP therapy is notoriously problematic; CPAP requires a significant lifestyle change involving the nightly application and use of a mask throughout sleep, which may be perceived as burdensome, invasive, and uncomfortable. Indeed, up to 25% of patients reject CPAP entirely, and of those who accept this treatment, many use it less than prescribed or abandon its use long term [4,5]. CPAP adherence rates have been estimated to range between 30-60% [5]. Reasons for non-adherence to CPAP are varied and complex, and may include problems with the CPAP device, side effects, and/ or patient characteristics, as well as psychological, behavioral and social factors [6,7]. One significant barrier to CPAP adherence often reported by patients is claustrophobia, the experience of anxiety, fear of suffocation, or panic in response to CPAP therapy. This review summarizes the prevalence and significance of claustrophobia in CPAP users, provides a theoretical framework for understanding claustrophobia, and discusses the potential application of exposure-based interventions.
Prevalence and Significance
Claustrophobia is a commonly reported side effect of CPAP therapy and may lead to treatment abandonment. Almost 30% of sleep apnea patients endorse feeling claustrophobic or closed in with CPAP [8, 9]. A recent study suggests much higher rates of claustrophobic tendencies in sleep apnea patients (63%), particularly in females (84%) compared to males (44%) [10]. Claustrophobia is perceived by patients as one of the largest deterrents to CPAP therapy, with less than half of patients reporting that they would use CPAP if they felt claustrophobic [11]. In a study assessing CPAP adherence and side effects, claustrophobia was the only treatment side effect that discriminated adherence, with low CPAP adherers more likely to report problems with claustrophobia than high adherers [9]. Subsequent studies have found claustrophobia to be associated with a greater risk of poor CPAP adherence [8,10]. Thus, claustrophobia is a widespread issue impacting successful CPAP therapy.
Theoretical Framework
Claustrophobia entails extreme anxiety and panic elicited by situations or settings in which the individual experiences a sense of being closed in or entrapped and is composed of two core fears: fear of restriction and fear of suffocation [12]. The feared situation or object is typically avoided, which serves to reduce anxiety in the short-term but maintains the phobia in the long term. The development and maintenance of such fears is explained by traditional learning theories (e.g., classical conditioning and operant learning) and provides a framework for understanding and treating CPAP-related claustrophobia (see Means & Edinger [13] for a detailed description of learning theory applied to CPAP-related claustrophobia).
Because CPAP requires the patient to breathe pressurized air through a mask strapped to the head, it is not difficult to understand how this treatment may elicit fears of suffocation and restriction. In some patients this therapy may provoke memories of traumatic experiences (e.g., near-suffocation experience while wearing a gas mask in the military, near-drowning experience while swimming, etc.), resulting in fear and avoidance of CPAP. Other patients may develop claustrophobic reactions de novo specifically in response to an unpleasant experience while using CPAP. For example, some patients may awaken from sleep feeling as though they are not getting enough air from CPAP and experience frightening feelings of suffocation. This anxiety reaction may be exacerbated by nasal congestion experienced either as a side effect of the CPAP or due to other causes (nasal obstruction, sinus problems, respiratory infections, etc.).
Exposure-based Interventions
Interventions targeting CPAP-related claustrophobia have been developed on the presumption that the phobic reaction to CPAP is conceptually similar to other phobias (e.g., fear of heights, fear of flying) and therefore should be treatable with the same psychological interventions such as graded exposure therapy or systematic desensitization [13]. Graded exposure therapy and systematic desensitization are designed to weaken the learned associations between the feared object and the anxiety reaction. In graded exposure therapy, the individual develops a hierarchy of steps (ranging from least to most anxiety-provoking) related to the feared object or situation, with the guidance of a therapist (a sample hierarchy for CPAP-related claustrophobia is presented in Figure 1).
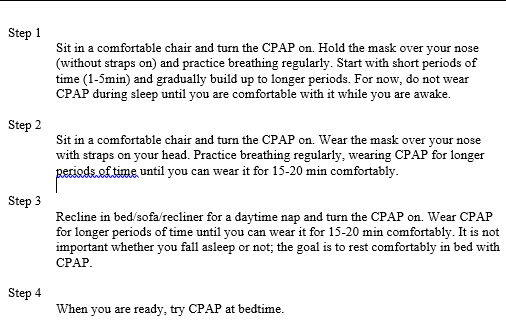
Figure 1: Sample graded exposure hierarchy for CPAP-related claustrophobia
The individual is then supported in confronting the feared situations in a gradual manner, and over time, the anxiety response lessens. The effectiveness of graded exposure therapy stems from learning to tolerate and manage anxiety without the need to escape or avoid the phobic stimulus. Desensitization therapy combines a relaxation component with the exposure hierarchy, so that anxiety experienced during exposure to the feared object or situation is replaced by feelings of relaxation.
Graded Exposure Therapy: Support for the potential effectiveness of graded exposure therapy for CPAP-related claustrophobia was first documented in a 1993 case study reported by Edinger & Radtke [14]. Post-therapy follow up with this case study patient showed continued CPAP use through an ensuing six-year period. A subsequent case study [15] and case series report [16] further validated the value of this intervention. In Means & Edinger’s [16] retrospective case series study, military veterans with CPAP-related claustrophobia attended between 1-6 exposure sessions with a behavioral sleep psychologist. Patients increased CPAP use 2.6 hours per night and 2.4 nights per week on average from pre-to-post therapy. Effect size calculations for CPAP adherence variables revealed a large effect of treatment. Consequently, Means and Edinger [13] developed a CPAP-specific exposure therapy protocol designed to be delivered in <6 sessions over 1-3 months.
Table 1: Summary of exposure-based intervention studies for CPAP-related claustrophobia.
| Edinger & Radtke [14] | McCrae & Ingmundson [15] | Means & Edinger [16] | |
| Study design | Case report | Case report | Retrospective case series |
| Sample size | 1 | 1 | 13 |
| Average age (years) | 44 | 45 | 60.9 |
| % male | 100 | 100 | 92 |
| Intervention | Graded exposure | Graded exposure | Graded exposure |
| # of treatment sessions | 5 | 6 | 2.6 (range = 1 - 6) |
| Follow up periods | 6 months; 6.5 years | 1 week; 4 months; 6 months | 15.3 weeks on average |
| Primary outcome measures | Self-report | Self-report | Objective measures of CPAP adherence (% of nights and hrs./night CPAP was used) |
| Main finding | Patient report of “routine use” of CPAP without claustrophobic symptoms at both follow up | Patient report of using CPAP nightly without anxiety | Statistically significant post-treatment increase in CPAP adherence measures |
Table 1 summarizes the current findings from outcome studies: to date, there have been no randomized controlled trials evaluating the effectiveness of this intervention.
For pediatric sleep apnea patients, graded exposure techniques incorporated as part of a behavioral treatment package have shown promise in promoting CPAP adherence [17, 18]. In these studies, however, it is impossible to disentangle the influence of the exposure technique per se from the other behavioral package components. Similar to adult sleep apnea patients, more research is needed to substantiate this intervention.
Desensitization Therapy: Desensitization therapy has not been systematically studied for CPAP-related claustrophobia. One study found that a treatment combination of education and progressive muscle relaxation improved CPAP adherence [19], suggesting that relaxation strategies may have therapeutic application with CPAP users. This finding, in consideration with the above noted positive findings regarding exposure therapy, suggests that desensitization therapy should be explored as a potential intervention in claustrophobic CPAP users.
DISCUSSION AND CONCLUSION
CPAP is the primary treatment for OSA, yet many patients struggle with using the device consistently. Claustrophobia is a common reaction to CPAP, typically described as a sense of feeling closed in or smothered. Exposure-based interventions show nascent promise for targeting CPAP-related claustrophobia. To date, such interventions lack rigorous scientific evaluation; the overall state of the research support is weak, with uncontrolled trials and small sample sizes. It remains to be determined whether variants of the exposure intervention (e.g., using exposure prophylactically to address anticipated claustrophobia prior to initiation of CPAP, adding relaxation techniques, or combining with other therapy techniques such as cognitive behavioral therapy or motivational enhancement) improves outcomes, at least for some individuals. Future studies with randomized controlled trials, larger sample sizes, objective measures of CPAP adherence, and long term outcomes are needed. Also needed are efforts directed toward formalizing the diagnosis of CPAP-related claustrophobia, standardizing measures of claustrophobia, and assessing predictors of outcome.
Despite these limitations, CPAP-related graded exposure therapy has become a routine part of our clinical sleep services due to its high demand and rewarding clinical outcomes. It can be translated easily into a group therapy format, increasing dissemination and optimizing use of resources. It is likely to be most effective when provided in the context of an integrated team approach which also incorporates managing other adherence barriers (e.g., nasal congestion, mask fit, pressure tolerance, etc.). A patient empowerment model, such as that proposed by Ciccone et al. [20] for patients with chronic health problems, advocates for patients engaging actively in the daily management of their health conditions, and provides one such framework with applicability to sleep apnea. Incorporated as part of a team approach, exposure therapy for CPAP-related claustrophobia offers an important option for the significant number of patients that can be expected to react to CPAP with claustrophobia.
REFERENCES
15. McCrae, Christina S, Ingmundson, Paul T. Using Graduated in Vivo Exposure to Treat a Claustrophobic Response to Nasal Continuous Positive Airway Pressure: Hispanic Male Veteran Associates Nasal Mask With Gas Masks Worn During Combat. Clinical Case Studies. 2006; 5: 71-82.
20. Ciccone MM, Aquilino A, Cortese F, Scicchitano P, Sassara M, Mola E, et al. Feasibility and effectiveness of a disease and care management model in the primary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc Health Risk Manag. 2010; 6: 297-305.









































































































































