Acquired Abdominal Intercostal Hernia: A Rare Incidence
- 1. Department of Surgery, Maharishi Markandeshwar Institute of Medical Sciences and Research, India
ABSTRACT
Acquired abdominal intercostal hernia (AAIH) is protrusion of abdominal viscera through an intercostal space under an intact diaphragm and is a very rare condition. In most cases the disease is acquired post trauma or surgery. The main presentation being swelling over the chest with or without pain. Complications like incarceration or strangulation may occur if left untreated. Computer tomography remains the gold standard investigation and AAIH should be always suspected when chest swelling occurs after a trauma or surgery. Surgery remains the only modality of treatment with tension free mesh repair being the preferred method either done via open or laparoscopic technique. We present one such rare case report of acquired abdominal intercostal hernia through the defect between 10th and 11th rib over the left upper abdomen over a previous surgical scar.
KEYWORDS
• Intercostal Hernia
• Traumatic hernia
• Acquired
CITATION
Choudhary K, Zaman M, Kaur G, Shah A, Yadav R, et al. (2018) Acquired Abdominal Intercostal Hernia: A Rare Incidence. J Surg Transplant Sci 6(2): 1067.
INTRODUCTION
Acquired abdominal intercostal hernia (AAIH) is a condition in which the intra-abdominal contents reach the intercostal space directly from the peritoneal cavity through an acquired defect in the abdominal wall musculature or fascia. The incidence of this disease is very rare [1]. Etiology is related mainly to trauma or previous surgery. The intercostal defects were mostly located under the 9th rib without significant differences as to side [2]. We present one such encounter with this rare case.
CASE REPORT
A 40 year male presented to us in emergency department with severe pain, swelling in the left upper abdomen over an old healed scar (Figure 1,2).

Figure 1: Swelling in the left upper abdomen.

Figure 2: Swelling with old healed scar.
Initially swelling was painless for 5 month which has now started pain for one day. He gave history a swelling over the left upper abdomen for which excision was done but exact nature of swelling was not given nor did patient have previous medical records. No history of nausea, vomiting, abdominal distension. Patient was passing stool, flatus. His B.P was 130/70mmhg, pulse 102/minute. On examination a swelling of around 8x8cm seen in the left lumbar region with an old healed scar over the swelling. Overlying skin was found to be normal. On palpation swelling was tender with no cough impulse and fluctuation. Rest abdomen was soft, no distension, no guarding. USG swelling was done showing collection of around 2x3 cm with edematous subcutaneous tissue. Probable diagnosis of obstructed incisional hernia was made in spite of the USG finding suggesting of abscess. Patient was resuscitated and taken up for exploration under general anesthesia in left lateral position. Intraoperative finding were single hernia sac between the 10th and 11th ribs left side. Hernial sac contained omentum as content (Figure 3).
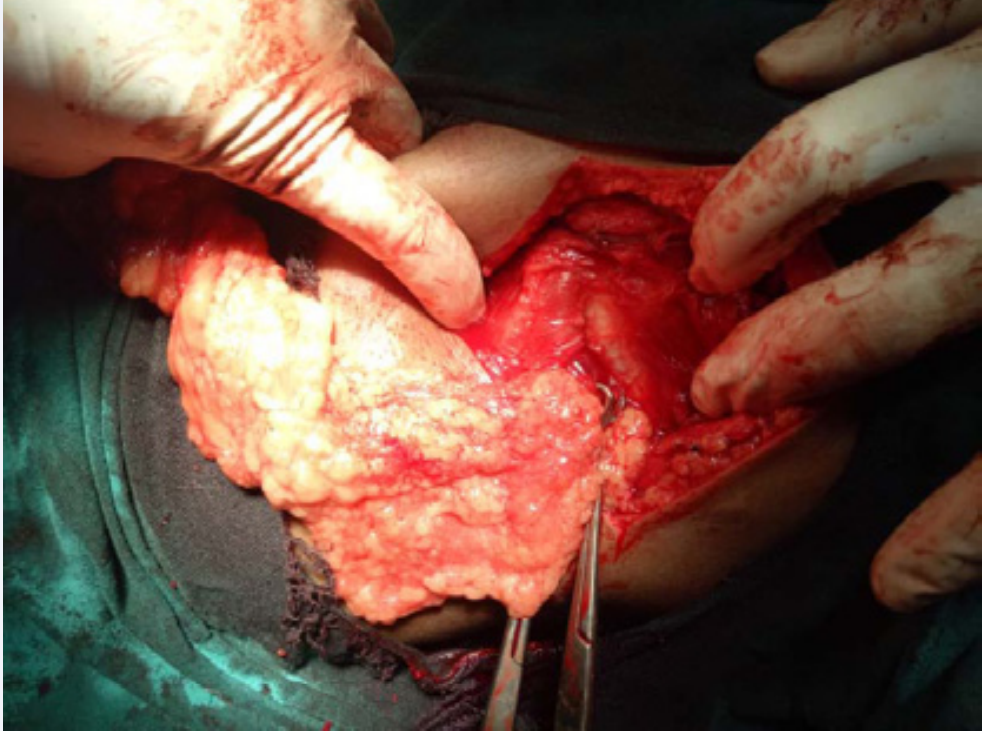
Figure 3: Intercostal defect with omentum as content.
Omentum reduced and defect of size 3x2 cm between 10th and 11th rib clearly visualized (Figure 4).

Figure 4: Content reduced clearly visualizing the defect.
PTFe mesh used to reinforce the defect intraperitoneally and intercostals muscles approximated over the mesh. Post operative period was uneventful and patient discharged on day 3. Sutures removed after 10 days. In routine follow up till 1 year he was asymptomatic.
DISCUSSION
Intercostal hernias are rare presentations caused by a disruption or weakness in the thoracoabdominal wall musculature resulting in herniation of fascia layers between adjacent ribs [1].
Intercostal hernias have been divided into two types: those with a diaphragmatic defect called transdiaphragmatic intercostal hernia (TIH) and those without a diaphragmatic defect called acquired abdominal intercostal hernia (AAIH) [3]. In most cases the disease is acquired post trauma or surgery. Rarely, they occur spontaneously or with congenital syndromes [1]. Specific areas of the chest wall are more vulnerable to herniation than others due to inherent weakness in certain anatomical zones like anteriorly from the costochondral junction to the sternum, as it lacks the support of the external intercostal muscle & posteriorly, the internal intercostal muscles are absent from the costal angle to the vertebrae [4,5]. The intercostal defects are mostly located under the 9th rib. The main symptoms remain chest swelling, often associated with discomfort or pain. Acute complications such as incarceration and strangulation can occur [2,6]. CT is the best diagnostic tool, since it not only provides excellent visualization but also offers a reliable means to establish a preoperative plan to repair the defect [7]. Surgical management is necessary in nearly all cases due to risk of incarceration and strangulation of organs except in elderly patients with multiple co morbidities who pose a high surgical risk in which conservative management is warranted [8]. Techniques to repair the defect include primary closure, absorbable and nonabsorbable meshes and patches, and prosthetic mesh reinforced by cable banding either by open or laparoscopic means [9]. The direct intercostal approach has been shown to be effective and safe [10]. The application of prosthetic reinforcement is favored in most cases, especially for very large or recurrent defects, since the absence of prosthetic support is associated with higher rates of recurrence [11]. Comprehensive literature review on AAIH reports that recurrences occurred in 28.6% of cases and were seen in up to 12 months [2]. Theories explaining the high recurrence rate are missed diaphragmatic tear, ripping of sutures, or the development of another defect from the jagged edges of rib fractures [12].
CONCLUSION
AAIH should be always suspected when chest swelling occurs after a trauma or surgery, and CT must be promptly performed to rule out diaphragmatic or abdominal viscera injury. This condition requires surgery to prevent serious complications; the first-choice technique should be mesh tension-free repair.









































































































































