An Unusual Case of Large Ascending Aortic Aneurysm with Severe Aortic Insufficiency
- 1. Department of Cardiology, Hospital de Santa Marta, Portugal
- 2. Department of Cardiothoracic Surgery, Hospital de Santa Marta, Portugal
ABSTRACT
The etiology of ascending aortic aneurysms includes genetic, degenerative, inflammatory and infectious causes. We present a case of a 49 year-old male patient without any known cardiovascular risk factors, who presented mainly with fatigue of increasing severity. The physical examination revealed a grade IV decrescendo, blowing aortic diastolic murmur, as well as an Austin Flint murmur and water hammer peripheral pulses. Imaging methods (echocardiography and computed tomography angiography) showed a large (8.6 cm) ascending aortic aneurysm with corresponding severe aortic insufficiency. In this context, he underwent surgical implantation of an aortic tube graft and mechanical prosthesis in aortic position, with good final result. Surprisingly, the histopathological diagnosis of the surgical specimen was compatible with atherosclerosis.
KEYWORDS
• Ascending aorta
• Aneurysm
• Aortic insufficiency
• Atherosclerosis
CITATION
Nogueira MA, Branco LM, Galrinho A, Laranjeira Á, Oliveira JA (2016) An Unusual Case of Large Ascending Aortic Aneurysm with Severe Aortic Insufficiency. J Surg Transplant Sci 4(3): 1031.
ABBREVIATIONS
BNP: Blood Natriuretic Peptide; CTA: Computed Tomography Angiography; MRA: Magnetic Resonance Angiography; TEE: Transesophageal Echocardiography; TTE: Transthoracic Echocardiography
INTRODUCTION
Thoracic aortic aneurysms have an incidence of 10/100 000 person-years and approximately 60% affect the ascending aorta [1]. The etiology of ascending aortic aneurysms includes genetic (such as Marfan, Loeys-Dietzor Ehlers-Danlos syndrome; bicuspid aortic valve), degenerative (atherosclerotic), inflammatory (for instance, giant cell arteritis) and infectious causes (Treponema pallidum, Staphylococcus aureus, Salmonella spp., among others) [1]. Nevertheless, atherosclerosis is the main cause of descending but not ascending aortic aneurysms [1]. The clinical presentation is variable, with most of the patients remaining asymptomatic for a long period of time. The symptoms are usually related to aortic insufficiency, heart failure, local compression of adjacent structures (cough, dyspnea, odynophagia or dysphagia, hoarseness due to left laryngeal nerve palsy) or even systemic embolization [1,2]. However, the first manifestation may correspond to the most feared complications: dissection (acute deep, aching or throbbing chest pain that can spread to the back, buttocks, groin or legs) and rupture (that can lead to sudden death) [1,2]. According to the Global Burden Disease 2010 project, the overall global death rate from aortic aneurysms and aortic dissection increased from 2.49 per 100 000 to 2.78 per 100 000 inhabitants between 1990 and 2010, with higher rates for men [2]. The main predictors of rupture are aneurysm size >6.5 cm and its expansion rate >5.5 mm per year, but and history of bicuspid aortic valve or Marfan syndrome are also determining factors of expansion rate [3,4]. Baseline laboratory assessment includes cardiovascular risk factors and albeit laboratory testing plays a minor role in the diagnosis of acute aortic diseases, it is useful for differential diagnoses [2].
The aorta is a complex geometric structure and, consequently, there are some limitations inherent to all imaging techniques (TTE, TEE, CTA or MRA). No imaging modality has perfect resolution and the precise depiction of the aortic walls depends on whether appropriate electrocardiogram (ECG) gating is employed [2,5].
In this regard, it is recommended that maximum aneurysm diameter be measured perpendicular to the centerline of the vessel with three-dimensional (3D) reconstructed CTA scan images whenever possible [2]. In fact, CT plays a central role in the diagnosis, risk stratification and management of aortic aneurysms [2]. Regarding treatment, aneurysms are repaired when the risk of rupture or dissection exceeds the risk of repair. The size thresholds for repair are determined by the underlying etiology of the aneurysm (usually >55 mm), with lower thresholds for those with genetic aortopathies (45 mm for Marfan’s syndrome and 50 mm for bicuspid aortic valve) [1,5-7].
CASE PRESENTATION
We present the case of a 49 year-old male patient who lived in Cape Verde, Africa and worked in the construction field. This patient had no relevant past medical story and no identifiable cardiovascular risk factors (arterial hypertension, smoking, hyperlipidemia, diabetes, family history of early cardiovascular disease) what so ever. Nevertheless, he started complaining mainly of progressively worsening fatigue and sporadically some chest discomfort (never described as pain), in the past few months. The patient was initially observed in his homeland and the physical examination revealed a grade IV decrescendo, blowing aortic diastolic murmur, as well as an Austin Flint murmur and water hammer peripheral pulses, suggestive of aortic insufficiency. After a brief workup, the patient was evacuated to Portugal, in order to investigate more thoroughly his condition and decide the best treatment. Regarding laboratory tests, the main results are depicted in Table, with only a slight elevation of BNP levels as a remarkable abnormality. The first imaging exam performed was a chest X-ray that showed both enlarged cardiac silhouette and aortic notch (Figure 1).

Figure 1: Chest radiograph (PA = posterior-anterior).
The TTE, using both multi planar and 3D acquisition (Figure 2a),
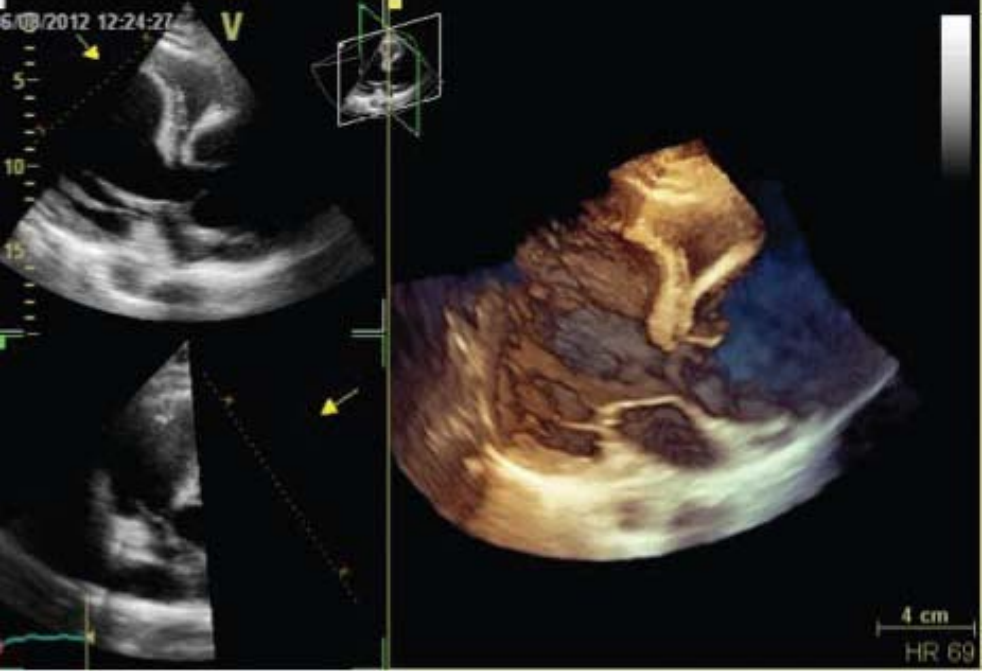
Figure 2a: Transthoracic echocardiography with 3D acquisition of aortic valve.
showed a severe aortic insufficiency [tricuspid valve; vena contracta = 8.3 mm, pressure half-time = 234 ms (Figure 2b),
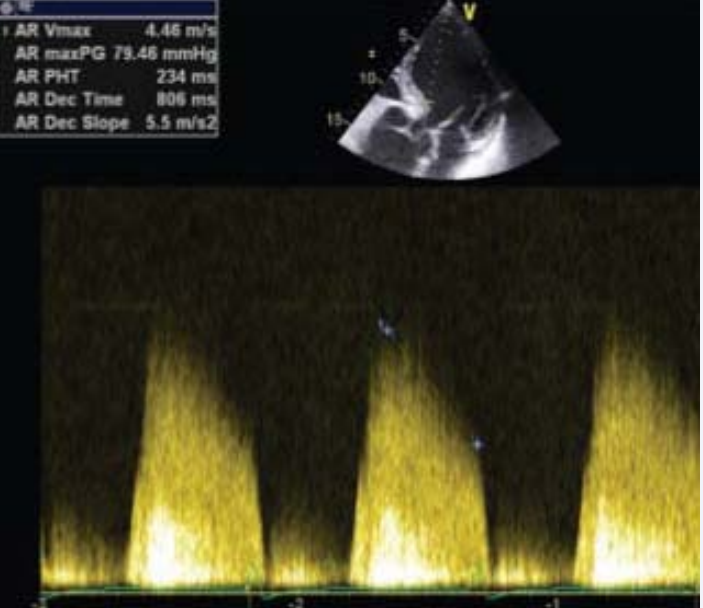
Figure 2b: AR PHT = Aortic Regurgitation Pressure Half-Time = 234 ms: obtained using continuous wave Doppler.
effective regurgitant orifice area = 0.9 cm2 and regurgitant volume = 164 mL (Figure 2c)],
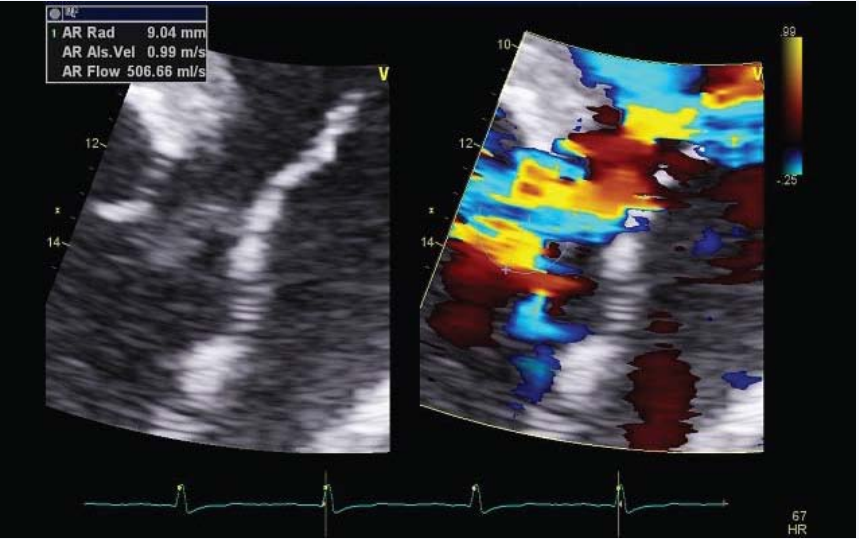
Figure 2c: PISA (Proximal IsovelocitySurfaceArea) method for aorticregurgitationquantification.
secondary to a large ascending aortic aneurysm (Figure 2d),
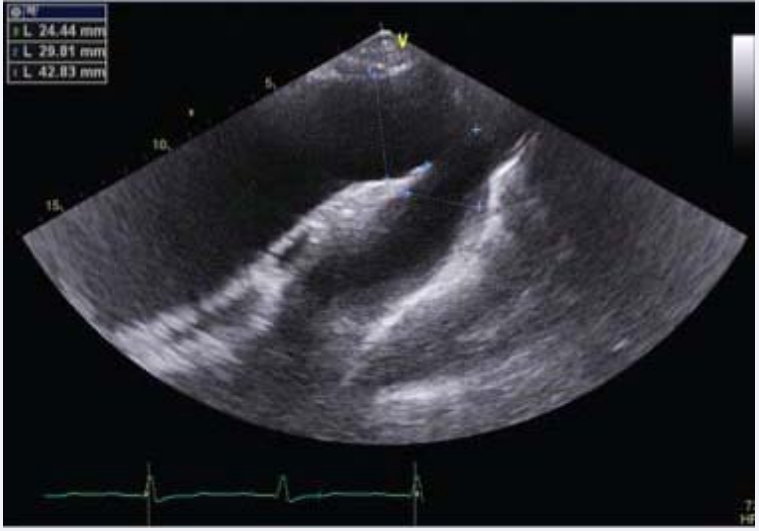
Figure 2d: Transthoracic echocardiography – suprasternal view, showing a dilation only of the ascending aorta.
with the following 2D measures: aortic ring = 4.1 cm, Valsalva sinuses = 5.18 cm, sino-tubular junction = 7.1 cm and ascending aorta = 8.7 cm. The left ventricle was enlarged, with ejection fraction (calculated by Simpson’s method and using 3D software) of 41% and global longitudinal strain of -14.4% (Figure 3).
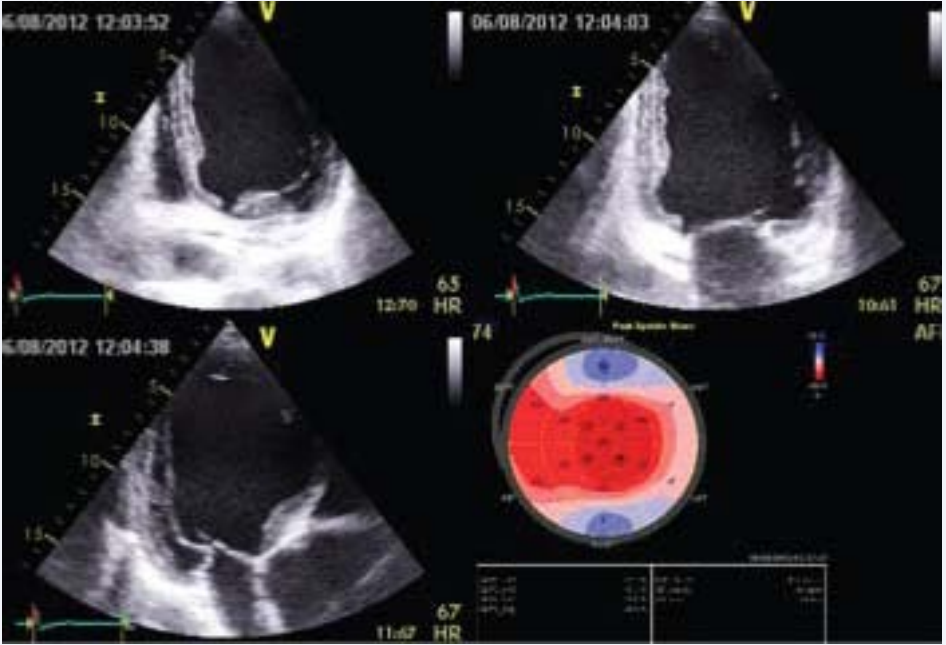
Figure 3: Global longitudinal strain of left ventricle.
Subsequently, the patient had a CTA (with 3D reconstruction) that confirmed the large ascending aortic aneurysm with 8.6 cm (Figures 4a, 4b and 4c).
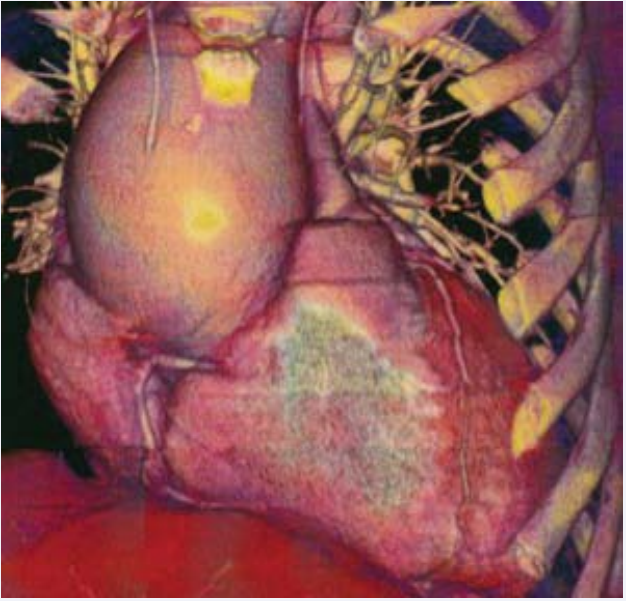
Figure 4a: Computed Tomography Angiography with 3D reconstruction – anterior view.
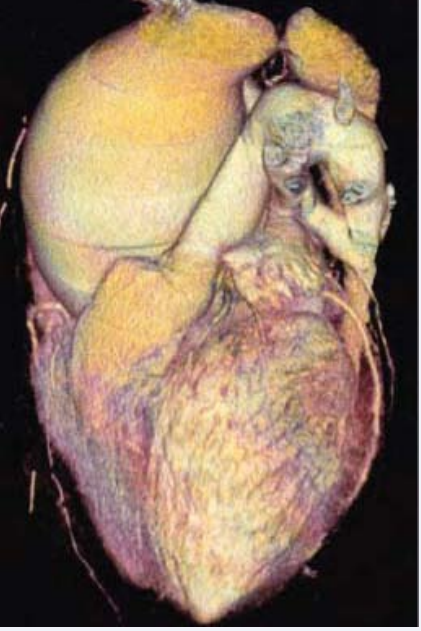
Figure 4b: Computed Tomography Angiography with 3D reconstruction – lateral view.
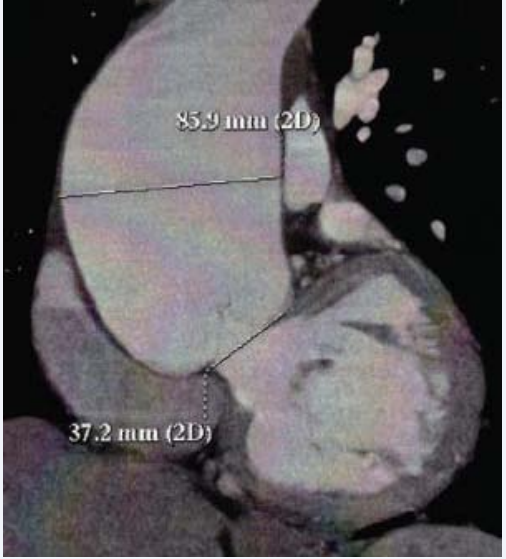
Figure 4c: Computed Tomography Angiography with measurement of the diameter of the aneurysm and aortic ring.
Additionally, it is important to underline that the calcium score was zero, there were no identifiable coronary lesions and there were no other aneurysms identified.
In this context, the patient underwent surgical resection of the aneurysm (Figure 5a),

Figure 5a: Picture of the ascending aortic aneurysm in the operating room.
with implantation of an aortic tube graft Jotec® # 30 (Figure 5b) and mechanical prosthesis in aortic position St. Jude® # 25 (Figure 5c), with good final result.
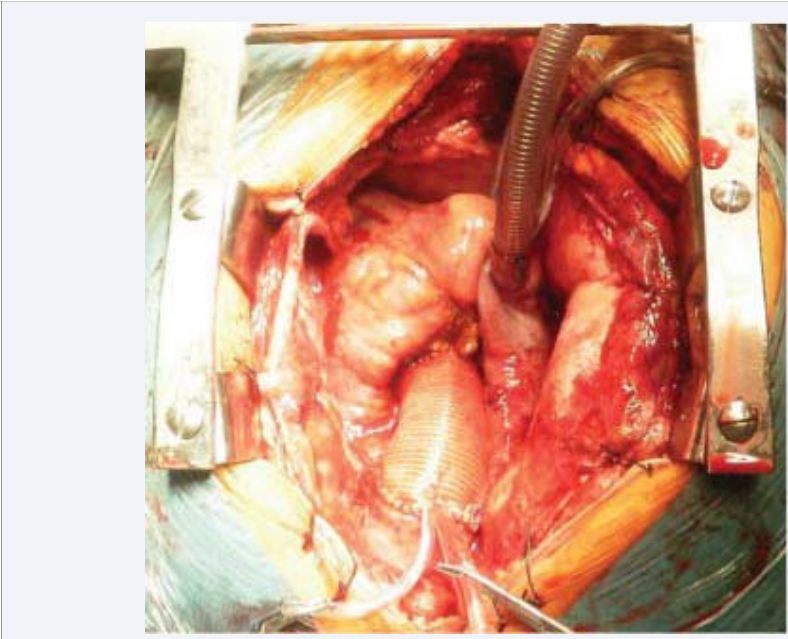
Figure 5b: Aortic tube graft Jotec® # 30 in place.

Figure 5c: Implantation of mechanical prosthesis in aortic position St. Jude® # 25.
Finally, the histopathological diagnosis of the surgical specimen was compatible with atherosclerosis (disruption of elastic fibers and smooth muscle cells that were partially replaced by extracellular matrix and lipids).
DISCUSSION
Ascending aortic aneurysms may present with symptoms related to aortic insufficiency, heart failure, local compression of adjacent structures or even systemic embolization [1-2]. However, considering that most aneurysms remain silent for a long period of time, harboring as they grow an increased risk of rupture and sudden cardiac death, it is extremely important their timely diagnosis (with an imaging exam, preferably CTA with 3D reconstruction) and adequate treatment (surgery when indicated) [2]. The size thresholds for surgical repair are determined by the underlying etiology of the aneurysm, with lower thresholds for those with genetic aortopathies [5-7]. In younger people, the most common causes of ascending aortic aneurysms are genetic (especially Marfan syndrome), but with time atherosclerosis becomes more prevalent [6]. On the contrary, atherosclerosis is the main cause of descending aortic aneurysms [1]. This case illustrates a large ascending aortic aneurysm with secondary severe aortic insufficiency and subsequent dilation of the left ventricle with discrete systolic dysfunction, extensively studied both by TTE and CTA. The surgical indication was straightforward and the patient underwent resection of the aneurysm with successful implantation of an aortic tube graft and mechanical prosthesis in aortic position. Considering his age (49 years old), absence of cardiovascular risk factors, localization of the aneurysm (ascending aorta) and country of origin, atherosclerosis was not a likely diagnosis. In fact, syphilis was formerly the main cause of ascending aortic aneurysms, but nowadays, in developed countries, it is much less common following the introduction of effective antibiotics [8]. On the opposite, in developing countries such as Cape Verde, infectious causes remain an important issue. This etiology was, indeed, excluded both by laboratory testing and histopathological exam. Nevertheless, the histopathological exam also excluded connective tissue disorders (CTD), like Marfan syndrome, that typically includecystic medial degeneration (characterized by fragmentation of elastic fibers, smooth muscle cell loss, increase in collagen deposition and replacement with intersticial cyst of mucoid appearing basophilic-staining ground substance) [1]. Considering the histological report and the absence of phenol typical manifestations characteristic of Marfan syndrome and other CTD, we decided not to perform any genetic testing. Despite the absence of known cardiovascular risk factors and of macroscopic plaques according to CTA, the final diagnosis of atherosclerotic origin has been made based on the histopathogical exam. On the one hand, the pathogenesis of atherosclerosisis multifactorial, envolving genetic predisposition and riskfactors (such as dyslipidemia, smoking, diabetes, systemic hypertension) that accelerate this process [1]. Nonetheless, there may be other potential risk factors contributing to the development of atherosclerosis, as recently suggested, like trimethylamine (present in many dietary compounds: meat, milk and other foods of animal origin) [9]. On the other hand, histologic examination shows considerable distinction between occlusive atherosclerotic disease - such as coronary arterydisease (CAD) – and aneurysmal disease [1], which means that the absence of CAD does not exclude the possibility of an aneurysm of atherosclerotic cause.
In conclusion, this case illustrates a large ascending aortic aneurysm with severe aortic insufficiency that turned out to be of atherosclerotic origin, against all odds, probably due to a genetically determined predisposition and/or an unrecognized vascular risk factor. To the best of our knowledge, this is the first case report published with the finding of such a large ascending aortic aneurysm due to atherosclerosis in a patient without any known cardiovascular risk factors
ACKNOWLEDGEMENTS
The authors would like to thank to Ms. Filipa Pereira for her valuable help regarding the pictures that illustrate this case report.









































































































































{kind=link}