Intrapelvic Hematoma Following Low-Energy Osteoporotic Pubic Ramus Fracutre: A Rare Case Report
- 1. Department of Orthopedic Surgery, Randers Regional Hospital, Denmark
Abstract
Osteoporotic pelvic fractures are common in the elderly and most often treated with pain management and mobilization. Pelvic hemorrhage rarely occurs but can prove life-threatening. An 86-year-old woman was admitted in the emergency department due to a fall from own height and sustained a displaced fracture of the superior ramus of the pubic bone. The patient presented with decreasing low blood pressure and tachycardia, and a CT-scan revealed an intraperitoneal bleed and pelvic hematoma. She was treated with intravenous fluids, fibrinolytic inhibitors and monitoring in the intensive care unit. A renewed CT-scan showed no active bleeding.
Only few case reports of pelvic hemorrhage in osteoporotic pelvic fractures exist. There is no consensus on treatment regimen. Choice of treatment ranges from various conservative measures through to embolization.
We emphasize, that it is essential to be aware of this rare but potentially life-threatening complication after low energy-traumas and report good results with conservative management.
Keywords
• Intrapelvic Hematoma
• Osteoporosis
• Pelvic Fracture
• Pelvic Hemorrhage
CITATION
Thorninger R. (2023) Intrapelvic Hematoma Following Low-Energy Osteoporotic Pubic Ramus Fracutre: A Rare Case Report. J Trauma Care 8(1): 1039.
ABBREVIATIONS
ED: Emergency Department; BPM: Beats Per Minute; GCS: Glascow Coma Score; ICU: Intensive Care Unit; CT: Computed Tomography
INTRODUCTION
Osteoporotic pelvic fractures are common in elderly patients following minimal trauma and often conservatively treated with sparse mobilization and pain relief. Complications such as life threatening bleeding might occur [1].
Pelvic hemorrhage due to dislocated fractures of either the superior- or inferior rami are well described in the setting of high-energy traumas [2]. Few reports in the case of low-energy fractures have been described with corresponding treatment consisting of various conservative measures or more invasive procedures, such as vascular coiling [3,4].
We report a case of a conservatively managed intrapelvic hematoma and hemorrhage following osteoporotic pubic ramus fracture due to a fall incident in a patient receiving platelet inhibiting anticoagulatory treatment.
CASE PRESENTATION
An 86-year-old woman presented to an ED at Randers Regional Hospital in Denmark, sustaining a low energy dislocated pubic ramus fracture due to a fall from her own height. The patient received treatment for hypertension, hypercholesterolemia, osteoporosis and received platelet-inhibitor treatment due to prior stroke (Clopidogrel, 75mg x 1 daily). The initial symptoms were pain in the lower left abdominal quadrant and ipsilateral hip, leaving the patient unable to ambulate. The patient was found with no displacement of the limbs. During admission the patient’s vital parameters rapidly declined, as she developed a decreasingly low blood pressure down to 67/40mmHg and a tachycardia of 110 BPM and raising respiratory rate upwards of 20 breaths/min. The patient was found to be pale and sweaty, but fully conscious with a GCS of 15. The abdomen was found tense and enlarged in the left lower quadrant. Abdominal stethoscopy proved regular bowel sounds. Initial arterial blood gasses revealed a hemoglobin of 7.8, a lactate of 1.7 and a pH-value of 7.355. The patient promptly responded to intensive Sodium Chloride fluid replacement therapy with a corresponding systolic blood pressure ranging from 80-100mmHg and lessening of previously reported tachycardia to below 100 BPM.
An abdominal CT scan with venous phase contrast showed a minor amount of free intraperitoneal blood and a pelvic haematoma in the left fossa in close relation to a left sided pubic ramus fracture with a cranially displaced fragment – but no signs of active bleeding (Figure 1).
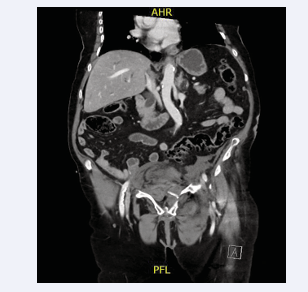
Figure 1: Abdominal CT-scan depicting intrapelvic heamatoma and displaced left-sided pubic rami fracture.
Interventional radiologists deemed these injuries unfit for coiling. Thus, the patient was treated conservatively with intensive intravenous fluid replacement therapy and close monitoring at the ICU. Tranexamic acid (1g/day for two days) was added as anti fibrinolytic treatment, and the patient received opioids to manage the pain. Renewed abdominal CT-scan the following day revealed regression of the hematoma and no signs of renewed bleeding or progression. Following two days at the ICU, the patient was adequately stable to be transferred to the Orthopedic Department for further pain management and mobilization. During the latter part of the hospitalization the patient suffered a left-sided pulmonary embolism that was treated with oxygen and Dalteparin. At no point during the hospitalization did the hemoglobin level drop below 6,0 and the patient received no blood transfusions. The patient was dismissed to local rehabilitation after 12 days of hospitalization.
DISCUSSION
In this case we present a very rare bleeding complication due to an osteoporotic pubic rami fracture. The patient was treated conservatively and responded well to the treatment.
To the best of our knowledge, there are only a handful of case reports describing similar cases and often in patients receiving intensive anti-coagulation treatment or bleedings necessitating endovascular coiling. [1,3].
Pelvic fractures are a common condition in elderly patients that is rarely complicated by life-threatening bleeding. The condition can prove difficult to diagnose due to the concomitant comorbidities in patients of this age group and atypical presentation. The timing and choice of the treatment might prove life-saving.
Treatment of this condition ranges from conservative management consisting of fluid-replacement, blood-transfusions, anticoagulation and pain relief to active embolization.
Sandri et al presented a similar case with an osteoporotic pubic ramus fracture requiring blood-transfusions due to arterial injury and corresponding anemia in a patient receiving more aggressive anticoagulatory treatment (Warfarin) [1]. Cases by Wee et al and Martin et al described similar conditions, however these patients were treated with embolization [4,5]. The literature is ambiguous on the matter of embolization versus conservative treatment, although some data show a reduced mortality rate in embolized patients [6]. However, complications to embolization itself are to be considered, as this in some cases can present a greater risk than the outcome [6]. Albeit the literature on the topic is scarce, there seems to be no correlation between the treatment with tranexamic acid and lung-embolisms in patients with pelvic fractures [7].
It is of utmost importance to be aware of the risk of life-threatening bleeding in the case of low-energy trauma patients presenting with atypical pain localizations, such as the abdomen. There is little to no literature describing morbidity of this complication and no standardized treatment program is established. Despite lack of consensus regarding treatment regimen, we report good results of conservative treatment in the reported case.
Our case warrants the importance of early suspicion for diagnosis and rapid treatment of this condition. Further research is warranted as to clarify whether these conditions are best treated conservatively or with embolization.









































































































































{kind=link}