An unusual urethral foreign body: A case report and review of the literature
- 1. Department of Urology B, Mohamed V University, Rabat, Morocco
Abstract
Rare instances of foreign bodies entering the urethra are documented in a large number of medical literature papers. They frequently follow from sexual curiosity, mental health issues, or, very infrequently, an attempt to pass urine. Imaging aids in the clinical diagnosis. Most treatments are endoscopic, although occasionally open surgery could be required. The patient’s psychological evaluation needs to be systematically integrated with the treatment method. We describe the case of a 34-year-old guy who had inserted a steel wire into his urethra and had a history of behavioral issues. Under general anesthesia, surgical extraction was the method of management. The patient was recommended for mental consultation upon release.
Keywords
• Urethral foreign body
• Metalic wire
• Case report
CITATION
Anas M,Maachi Y, Fouimtizi J, sSlaoui A,Karmouni T, et al. (2024) An unusual urethral foreign body: A case report and review of the literature. J Urol Res 11(1): 1146.
INTRODUCTION
Male urethral foreign bodies that are self-inserted are an uncommon emergency that general and urology surgeons may encounter. It is an uncommon technique known to involve the introduction of any imagined object into the urinary tract. Males are 1.7 times more likely than females to do lower urinary tract foreign body insertions, which had a low incidence in a series of 20 adult cases over a 9-year period [1]. Individuals are 35.8 ± 20.0 years old on average [1].
The habit is most common when intoxicated, in stages of pathological masturbation, or as a result of psychological compounders [2].
Since the beginning of time, autoerotic stimulation with the help of self-inserted urethral foreign bodies has existed. Urologists are familiar with this unique but well-known appearance [2,3].
But the basic feeling of humiliation causes the presentation to be postponed. The most prevalent presenting signs among patients who seek medical attention are dysuria, haematuria, urine frequency, strangulation, and urinary retention [1-4]. Severe outcomes, including fatal sepsis, may result from such behavior in the case of a postponed medical consultation [2].
The example of a penile urethral steel wire that we report here is unusual, despite the literature on self-inserted urethral foreign bodies being available [5,6]. After describing the clinical presentation, examination, and management, the literature is reviewed.
CASE REPORT
The patient was a 34-year-old single man with no occupation, received in the emergency department for a urethral foreign body (metal thread), the patient arrived at the emergency of our hospital 12 hours after the incident. Questioning revealed an unspecified psychiatric history.
Upon examination, there was no urethrorrhagia, haematuria, bladder globe, or edema of the external genitalia. There was also a presence of two pieces of metal wire through the urethral meatus (Figure 1).
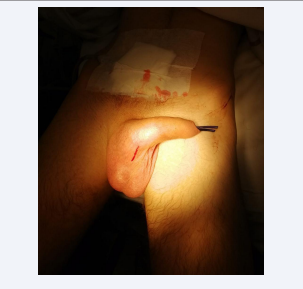
Figure 1: Two pieces of metal wire through the urethral meatus
There was urine leakage along the thread’s periphery and drip-like micturition.
A mass was palpated through the perineal urethra. A manual extraction attempt in the emergency department was unsuccessful, prompting a PSA, which revealed an opacity corresponding to the heads of the wire, with one of the knots visible.
The patient was finally referred to the operating room, an endoscopic treatment was envisaged, during the introduction of the cystoscope a knot in the metal wire at the level of the urethra was observed. The endoscopic extraction attempt failed. We decided to stop the endoscopic procedure.
Where he underwent surgery involving a Longitudinal skin incision on ventral penile surface (Figure 2).
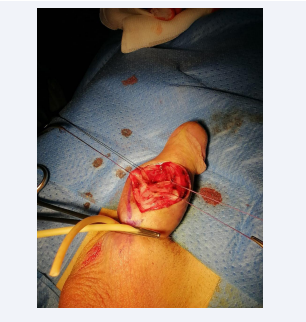
Figure 2: Longitudinal skin incision on ventral penile surface.
After the incision is made, the underlying tissues, such as the subcutaneous fat and fascia, may be dissected or separated to gain access to the structures or tissues requiring treatment or manipulation, enabling the thread to be extracted at the level of the knot (Figure 3).
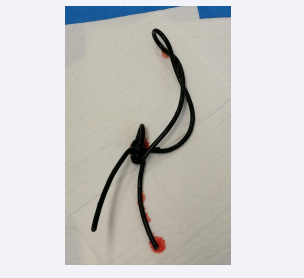
Figure 3: Entire wire after extraction.
Post-operative management was straightforward, with urinary drainage via urethral catheter for two weeks, and a psychiatric consultation .
The patient was seen again as an outpatient at one, three and six months, with no urinary disorders.
DISCUSSION
Most urinary tract foreign bodies are inserted during masturbation, but often in the context of mental illness with impulsive self-aggressive acts [7].
Patients, often embarrassed to seek medical attention, may make several attempts to extract the object with the risk of bladder migration and injury.
The symptoms induced by foreign bodies in the urethra are varied. In an acute situation, symptoms usually symptoms are dysuria [8] and macroscopic hematuria. In the chronic stage, there may be recurrent and dysuria [9].
Physical examinations are most frequently used to confirm diagnoses. It is easy to feel foreign bodies that are farther away from the urogenital diaphragm. A computerized tomography of the abdomen and/or pelvis, along with a pelvic X-ray, can be helpful in determining the location, orientation, and implications of a foreign body.
The physical characteristics and form of the foreign body indicate how best to retrieve it while minimizing urothelial damage and maintaining erectile function. Because a metallique wire is not encountered very often, there is not enough data to assess and contrast different treatment approaches. Since forceps, snares, and baskets can frequently be used to successfully remove foreign things distal to the urogenital diaphragm using endoscopic techniques, these procedures have taken precedence in medical care [1,2]. If the foreign body is removed by endoscopic treatment, cystourethroscopy is essential after extraction of the foreign body to check for any lesions following extraction [3].
More invasive foreign body extraction techniques, such as meatotomy or suprapubic cystotomy for posterior urethral foreign bodies or external urethrotomy for pendulous urethral foreign bodies, may be necessary on occasion [10,11]. Although they are uncommon, complications from the previous surgeries can result in diverticulum, infection, fistula, urethral stricture, and incontinence [11].
With a 5% incidence, urethral strictures are the most frequent delayed complication out of all of these [1]. As a result, proper follow-up is crucial to tracking the emergence of problems.
In our case, the diagnosis was obvious on inspection the end of the wire was visible at the level of the penis, prompting the emergency doctor to attempt manual extraction, which is not recommended.
Most foreign bodies in the urethra are removed by minimally invasive endoscopic techniques, and urethral manipulation or catheterization should be avoided until the exact type, shape, size, mobility and location of the object have been determined.
The exact type, shape, size, mobility and location of the object.
In certain complex cases, such as our patient’s (knot with several turns of the coil, calcified foreign body, etc.), surgery is certainly more invasive, but has the advantage of resolving the problem without great morbidity.
Foreign bodies come in a wide variety of forms, from metallic wire
In our patient’s case, but also tweezers, hairpins, tacks pins, thumbtacks, pebbles and paper clips.
CONCLUSION
This instance serves as a reminder of various crucial management guidelines in the event of an uncommon urological emergency. The form and position of the foreign body serve as guides for its extraction, which is frequently accomplished endoscopically but in some cases surgery is required to remove the foreign body, as in the case of our patient.
A more comprehensive approach to management is necessary, though, and this entails not only monitoring for delayed complications, minimizing the risk of infection, assessing and documenting any more serious underlying injuries, and preventing future episodes, but also thoroughly evaluating motivation and psychosocial issues, which in and of itself calls for attention and may prevent future episodes.
REFERENCES
- Mannan A, Anwar S, Qayyum A, Tasneem RA. Foreign bodies in the urinary bladder and their management: a Pakistani experience. Singapore Med J. 2011; 52: 24-28.
- Bedi N, El-Husseiny T, Buchholz N, Masood J. ‘Putting lead in your pencil’: self-insertion of an unusual urethral foreign body for sexual gratification. JRSM Short Rep. 2010; 1: 18.
- Rieder J, Brusky J, Tran V, Stern K, Aboseif S. Review of intentionally self-inflicted, accidental and iatrogenic foreign objects in the genitourinary tract. Urol Int. 2010; 84: 471-475.
- Moon SJ, Kim DH, Chung JH Jo JK, Son YW, Choi HY, et al. Unusual foreign bodies in the urinary bladder and urethra due to autoerotism. Int Neurourol J. 2010; 14: 186-189.
- Saito G, Abe T, Unoura A. Urethral foreign body fork: in a man inserted by himself in order to dilate his urethra: a case report. Nishinihon Journal of Urology. 2005; 67: 559-561.
- Stravodimos KG, Koritsiadis G, Koutalellis G. Electrical wire as a foreign body in the male urethra: a case report. J Med Case Rep. 2009; 3: 49.
- Hwang EC, Kim JS, Jung SI, Im CM, Yun BH, Kwon DD, et al. Delayed diagnosis of an intraurethral foreign body causing urosepsis and penile necrosis. Korean J Urol. 2010; 51: 149-151.
- Houlgatte A, Fournier R. Les corps étrangers de l’urètre. Ann Urol (Paris). 2004; 38: 45-51.
- Granados EA, Riley G, Rios GJ, Salvador J, Vicente J. Self introduction of uretrovesical foreign bodies. Eur Urol. 1991; 19: 259-261.
- Mitterberger M, Peschel R, Frauscher F, Pinggera GM. Allen key completely in male urethra: a case report. Cases J. 2009; 2: 7408.
- Poole-Wilson DS. The immediate treatment of urethral injuries. Proc R Soc Med: Section of Urology; 1956; 49: 685-689.









































































































































{kind=link}