Development of a Variant of the Yang Monti Technique in Ureteral Stenosis Surgery
- 1. Urology Department, Avicenne Hospital, University Hospital Center IBN SINA, University Mohammed V, Morocco
Summary
Our work aims to report our solution for the management of complex and extensive ureteral stenosis.
t concerns a 30 years old patient who consulted our Urology B Department of the University Hospital of Rabat, for febrile right renal colic. Paraclinical examinations revealed an extensive stenosis with a subjunctional stone.
In a first step, we diverted urine through a nephrostomy tube. Then in a second step the patient was taken back, with the placement of a Yang monti type urinary shunt using a jejunal graft. The postoperative course was simple. The patient was reviewed 3 months after surgery, there were no complaints except for thick urine due to mucus, a change of JJ probe was decided before its final removal 4 months after surgery. The control creatinine was normal and the control images at 1 and 2 years showed a very satisfactory result
Cite this article
Himmi Y, Amine S, Mouftah B, Tariq K, El Khader K, et al. (2022) Development of a Variant of the Yang Monti Technique in Ureteral Stenosis Surgery. J Urol Res 9(2): 1133.
INTRODUCTION
The treatment of extensive ureteral stenosis is complex. Replacement of the ureter with the bowel is indicated after failure of endoscopic treatments or other ureteral plasty techniques using the urinary tract
In this article, we propose a simple and effective solution for the management of extensive and complex ureteral stenosis: uretero-jejunoplasty.
Patient and observation
This is a 30-year-old patient who consulted our urology B department at the University Hospital of Rabat for febrile right renal colic.
In his history, there was a notion of mictional burns and low back pain dating back 4 months.
The physical examination revealed sensitivity of the right upper ureteral point and the lumbar contact.
Biologically, hemoglobin was 14.5 g/dl, white blood cells 12,000/mm3 and platelets 200,000/mm3 , creatinine 88.6 µmol/l, urea 0.27 g/l, sodium 136 mEq/l, kalaemia 4.5 mEq/l, and cytobacteriological examination of the urine isolated multisensitive Escherichia Coli.
The Uroscanner revealed a right ureterohydronephrosis upstream of a sub-junctional calculus (Figure 1).
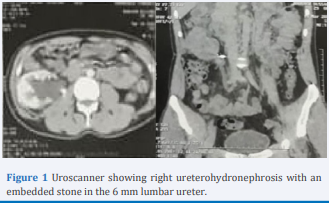
Figure 1: Uroscanner showing right ureterohydronephrosis with an embedded stone in the 6 mm lumbar ureter.
A temporary urinary diversion by nephrostomy tube was performed after failure of diversion by a JJ probe. Antibiotic therapy was initiated and the patient was seen again one month later with urine sterilization.
The indication for a Yang Monti type urinary shunt replacing the stenotic portion of the ureter was given.
The approach was median intraperitoneal, the ascending colon had to be detached, and the intestinal graft was passed through the mesocolon.
In contrast to Monti, which uses a 2-3 cm pedicled and tubulated ileal segment [1], our variant advocates the use of a 3 cm jejunal graft (Figure 2). It is imperative to ensure that there is no traction. Restoration of intestinal continuity was achieved by means of a jejuno-jejunal anastomosis in front of the graft. Then the mesenteric defect is closed. (Figure 2)
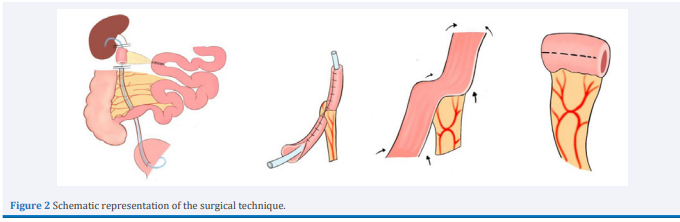
Figure 2: Schematic representation of the surgical technique
A Monti is made with 4-0 PDS, then the neo-ureteropylar anastomosis followed by the neo-uretero-ureteral anastomosis on a double J tube is made terminally on spatulated ends with 4-0 resorbable thread, and finally a drainage of the lodge by redon drain.
Her evolution was marked by simple after-effects, a resumption of gas transit on Day 2, by stools on Day 4, and removal of the bladder catheter and the Redon drain on Day 5.
The anatomical-pathological examination of the urethrectomy specimen revealed a non-specific chronic inflammation.
The patient was seen again 3 months after the operation, he had no complaints apart from slightly thick urine containing mucus. The creatinine was normal and the uroscanner showed a continuous shunt with no impact on the upper tract. The JJ catheter was changed and removed four months after the operation.
The patient was reviewed at 6 months, 1 year and 2 years with follow-up images that were normal (Figure 3(A-B-C)).
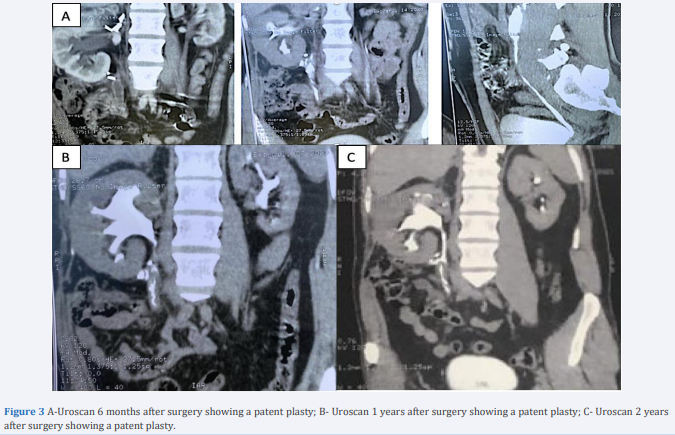
Figure 3: A-Uroscan 6 months after surgery showing a patent plasty; B- Uroscan 1 years after surgery showing a patent plasty; C- Uroscan 2 years after surgery showing a patent plasty.
DISCUSSION
Ureteral pathologies requiring replacement are represented mainly by iatrogenic stenosis secondary to lithiasis surgery, gynecological procedures or post radiation.
Ureteral stenosis can occur as a result of direct injury or focal ischemia of the ureter [2]. Other etiologies may include retroperitoneal fibrosis, specific urinary tract infections (tuberculosis and bilharzia) and excretory tract tumors. A rarer indication is the removal of cutaneous ureterostomies [3].
The predominance of males is clear in all series [4]. This was the case for our patient who was male. This gender predominance will not be significant as this was an observation. Low back pain was the most frequent reason for consultation, i.e. 40% of cases according to Galifer et al [4].
As a general rule, endo-urological treatment is carried out as a first-line treatment in the face of ureteral stenosis. If endoscopic techniques fail, surgical correction is performed [5]. This is consistent with our treatment approach, as the ureteral stenosis was greater than 2 cm and old
The first uretero-ileoplasty in men was performed in 1906 by SHOEMAKER [6]. Several authors have subsequently adopted this technique to treat ureteral stenosis [7]. Replacement of the ureter by the intestine is indicated after failure of endoscopic treatments or other ureteral plastic surgery techniques using the urinary tract.
Interposition of the bowel in the urinary tract can be complicated by hyperchloremic acidosis [8,9]. These electrolyte disturbances are observed especially when there is urine stasis in the graft or when the length of the graft is large. The reabsorption of urinary constituents by the intestinal tract has been studied experimentally in the dog. In the jejunum, chlorine and sodium losses are less than in the ileum [10]
The absence of metabolic disorders in our case is explained by the good selection of the patient (normal renal function), the reduction of the size of the absorbing surface and a good implantation of the reconfigured jejunal tube which allowed to decrease the contact of urine with the jejunal mucosa.
This technique is safe with acceptable morbidity and mortality [11,12]. The patient reported thickening of the urine in the first week due to hyperproduction of mucus requiring a change of JJ tube.
The main objective of any ureteral replacement technique is to preserve renal function. Therefore, before proposing ureteroileoplasty, it is important to ensure that renal function is not impaired [13].
The follow-up of our patient revealed a stabilization of his creatinemia. Authors who have used the Monti principle have also reported preservation of renal function during their shortterm follow-up [11,12].
CONCLUSION
The use of the Yang-Monti principle in ureter replacement is an adequate solution. It is safe and effective in treating extensive and complex ureteral stenosis.
REFERENCES
1. Savoie P H, et al. Réparations chirurgicales des lésions de l’uretère. EMC-techniques chirurgicales-urologie 2013; 6: 1-15.
6. Melinkoff A.E. Sur le remplacement de l’urete?re par une anse isole?e de l’intestin gre?le. Rev. Clin. Urol., 1912, 1, 601-604.
13.Alem CE, Huffman JL, Lieskovsky G, Boyd SD, Skinner DG. Long term clinical success for ileal ureteral substitution. J Urol. 1995.









































































































































{kind=link}