Emphysematous Pyelitis Secondary to Obstruct if Stone in a Healthy Adult Woman
- 1. Department of Urology B, Ibn Sina teaching hospital, Morocco
- 2. Faculty of Medicine and Pharmacy, Mohammed V University, Morocco
Abstract
Emphysematous pyelitis is a rare infection characterized by the presence of gas exclusively in the renal collecting system. Obstruction represent its main predisposing factor. Computed-tomography scan represents the modality of choice to characterize distribution of gas. The treatment is based on effective antibiotic therapy associated with drainage of excretory cavities if obstructed. The authors report a case of a young women presenting with fever and left lumbar pain. Computed-tomography revealed an emphysematous pyelitis in a left obstructed kidney. Effective antibiotic therapy associated with drainage of excretory cavitiespermitted symptoms improving. Through our case we illustrate particularities of this rare entity with an emphasis on differences from emphysematous pyelonephritis. As opposed to emphysematous pyelonephritis, emphysematous pyelitis is a benign condition of an excellent prognosis.
Keywords
Emphysematouspyelitis; Calculi; Upper urinary tract infection
Citation
Jabbour Y, Touzani MA, Karmouni T, El Khader K, Koutani A, et al. (2018) Emphysematous Pyelitis Secondary to Obstruct if Stone in a Healthy Adult Woman. J Urol Res 5(3): 1106.
INTRODUCTION
Gas in the urinary system is a rare and unusual finding observed during uro-digestive fistulas or following endo-urologic procedures [1-3].
Presence of gas in urinary system can also be seen during acute renal infections with gas-producing organisms corresponding to a life-threatening medical and surgical emergency called emphysematous pyelonephritis (EPN) characterized by presence of gas within the renal parenchyma or perirenal tissues. This rare entity was firstly reported by Kelly and MacCullum in 1898 and was reported to be of worse prognosis especially if tardily diagnosed [4].
Its incidence is raising with the spread use of computed tomography permitting its detection in early stages. Emphysematous pyelitis representing an early stage of EPN is even rarer. Thus, few series in the literature have been devoted to EP.
Derouiche et al., reported only 6 cases of EP in a periode of ten years [2].
CASE PRESENTATION
We report the case of young 34-years-old women with no particular medical or surgical history admitted to emergency department for a worsening of left lumbar pain with an onset of fever. She reported no associated urinary complains.
Clinical examination revealed a 38,8 fever with other vital signs within normal limits and left renal angle tenderness in abdominal examination.
KUB X-ray revealed presence of calcification within the left renal area. Abdominal ultrasonography reveled hydronephrotic left kidney upon an obstruct if renal pelvic stone A subsequent abdominal computed tomography showed an enlarged left kidney measuring 16271 mm with important pelvicalyceal dilatation (anterior–posterior renal pelvic diameter of 52mm) upon an obstruct if stone lying within ureteropelvic junction measuring 8×12×13mm in length and 1400 U.H in density (Figure 1).
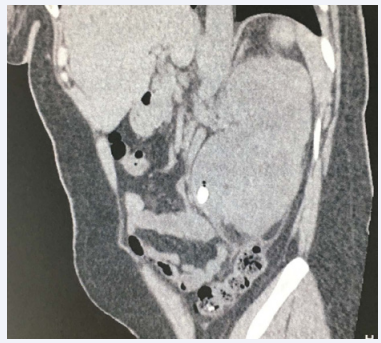
Figure 1: Sagittal non-enchased computed tomography scan showing small pockets of air in an obstructed and enlarged left kidney with upon an obstruct if stone lying within ureteropelvic junction.
Perirenal fat thickness was noted. In addition to those features computed tomography revealed presence of multiple foci of air in the dilated leftrenal pelvis with no similar finding in the left renal parenchyma or perinephric region (Figure 2).
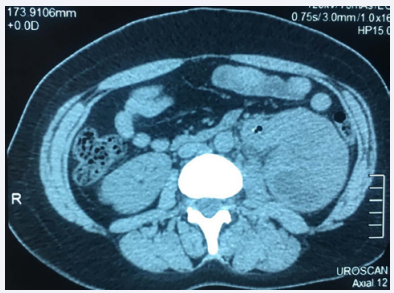
Figure 2: Transversal non-enchased computed tomography scan showing small pocket of air within renal pelvis without parenchymal or perinephric extension.
The patient denied any previous urological interventionor urinary tract catheterization.
Laboratory findings showed normal renal function, high white blood cell count of 9200 cells/ml, low hemoglobin level of 9.7 g/dl, and normal platelet count of 410 cells/ml, C-reactive protein at 222,50 mg/ml. Her urine analysis showed small blood, high rate leukocyturia (560/mm3 ) and bacteriuria (620,25.103 UFC/ml). Urine culture yielded growth of a resistant Eschericia coli.
The patient was not known to be diabetic and her fasting blood sugar and glycated hemoglobin levels remained within normal limits.
With above findings, we concluded to diagnosis of emphysematous pyelitis.
Patient received initially a ceftriaxone and amikacin based systemic antibiotherapy. A double j stent was inserted to relief obstruction.
Three days later the fever resolved and her symptoms improved. Inflammatorymarkers returned to baseline within five days.
The patient was discharged under oral antibiotherapy and was planned for ureteroscopy with laser lithotripsy for management of her renal pelvic stone.
DISCUSSION
EPN is divided into four classes determined according to the extent of the gas expansion. Emphysematous pyelitis (EP) represent a sub class of EPN when when gas is only limited to the collecting system (pelvicalyceal system, ureters or in the urinary bladder) [4].
Organism found in emphysematous pyelonephritis are mainly bacterial. is the most common, followed by Klebsiella pneumoniae, Proteus mirabilis and Pseudomonas aeruginosa [6]. Despite sharing same pathogenesis literature data reveal several differences between EPN and EP concerningpredisposing factors, clinical presentation, therapeutic management, prognosis and outcome.
Distinction between both entities is important since it has implication on management and prognosis [7].
EPN and EP are commonly seen in womenpresumably because of their increased susceptibility to urinary tract infections. Uncontrolled diabetes and urinary tract obstructionrepresent their major predisposingfactors. However, EP seems to have a lower association with diabetes counting for only 50% of patients compared to 90% of patients with other subclasses of EPN [7,8].
In the present case urinary tract obstruction and female sex were the predisposing factors associated with EP. Clinically EPN can present with serious manifestation as acute renal failureor shockwhereasclinical features of EP are mostly similar to classical acute pyelonephritis (hematuria, fever with chills, lumbar tenderness) [3,5,10].
Computerized tomography is currently the most sensitive and specific imaging modality for diagnosis of emphysematous urinary tract infections and also for characterization of the location of gaz (intracalyceal, intraparenchymal, perinephric, or pararenal) [9]. In our case neither ultrasonographynor KUB X-ray revealed emphysematous pyelitis.
EPN is a life-treating infection with high rate of mortality of 50 % if not timely identified and early treated. EPhave a more favorable outcomewith much lower overall mortality rate not exceeding 20% [7,8].
Current evidence shows that EPNcan be treated successfully with concervat if approach by means of timely antibiotic treatment, glycaemic control and adequate drainage of the collecting system either percutaneously or with placement of double-J stents. Although some cases may requireemergencynephrectomyas salvage procedure. On the other hand, EPinvolves only medical management, with a drainage procedure when obstruction coexists [2,3,10].
CONCLUSION
Owing to widespread availability of better investigative radiological tools, early detection even of small pockets of air in kidneys of patients with urinary tract infection has become possible as demonstrated by our case.
This lead to early diagnosis and management preventing the evolution of the gasogenic process, allowing kidneys preservation and improving significantly the prognosis.
REFERENCES
- Maiti A, Saha D, Das A. Emphysematous Pyelitis: An Entity Distinct from Emphysematous Pyelonephritis. Am J Med Sci. 2017; 353: 505.
- Derouiche A, El Attat R, Hentati H, Blah M, Slama A, Chebil M. Emphysematous pyelitis: epidemiological, therapeutic and evolutive features. Tunis Med. 2009; 87: 180-183.
- Roy C, Pfleger DD, Tuchmann CM, Lang HH, Saussine CC, Jacqmin D. Emphysematous pyelitis: findings in five patients. Radiology. 2001; 218: 647-650.
- Schultz EH Jr, Klorfein EH. Emphysematous pyelonephritis. J Urol. 1962; 87: 762-766.
- Huang J, Tseng C. Emphysematous Pyelonephritis Clinicoradiological Classification, Management, Prognosis, and Pathogenesis. Arch Intern Med. 2000; 160: 797–805.
- Alansari A, Borras MD, Boma N. “I have chicken fat in my urine!” A case of Candida tropicalis induced emphysematous pyelitis. Med Mycol Case Rep. 2015; 10: 27–28.
- Hiremath R, Mahesh, Padala KP, Swamy K, Pailoor A. A Rare Case of Pneumoureter: Emphysematous Pyelitis versus Emphysematous Pyelonephritis. J ClinDiagn Res. 2015; 9: TD03–TD05.
- Wiesel S, Gutman A, Abraham JE, Kiroycheva M. Foley Follies: Emphysematous Pyelitis from Instrumentation in Obstructive Uropathy. Cureus. 2017; 9: e1612.
- Bohlman ME, Sweren BS, Khazan R, Minkin SD, Goldman SM, Fishman EK. Emphysematous pyelitis and emphysematous pyelonephritis characterized by computerized tomography. South Med J. 1991; 84: 1438-1443.
- Sokhal AK, Kumar M, Purkait B, Jhanwar A, Singh K, Bansal A, et al. Emphysematous pyelonephritis: Changing trend of clinical spectrum, pathogenesis, management and outcome. Turk J Urol. 2017; 43: 202–209.








































































































































{kind=link}