Intratesticular Pseudoaneurysm after Trauma: A Case Report
- 1. School of Health Sciences, Universidade Positivo, Brazil
Abstract
Intratesticular pseudoaneurysm is a rare and little discussed condition. It is characterized as a blood leak surrounded by a pseudocapsule and its treatment can be both conservative and surgical. Therefore, with few cases described in the literature, it is difficult to diagnose and choose the conduct to be chosen. Accordingly, this study aimed to report the case of a patient diagnosed with intratesticular pseudoaneurysm after blunt trauma in the scrotal region. Patient admitted to the emergency room with pain in the region, associated with edema in the scrotum. On ultrasound examination, an image suggestive of rupture of the tunica albulginea of the right testis, associated with vascular injury with pseudoaneurysm formation. Therefore, the patient underwent surgery with exploration of the hematoma, drainage and marsupialization. This is an extremely rare case, therefore, the literature still lacks sources to explain the best surgical or conservative treatment in relation to the chances of success.
Keywords
Pseudoaneurysm, Testicle, Trauma, Treatment
ABBREVIATIONS
US: Ultrasound
Cite this article
Schinke MR, Ronau Hadlich LE, da Silva Y, Meneghete BP, Cavalli MM (2022) Intratesticular Pseudoaneurysm after Trauma: A Case Report. J Urol Res 9(1): 1129.
INTRODUCTION
Scrotal trauma accounts for less than 1% of all traumarelated injuries. This is not an uncommon lesion due to its anatomy, location and mobility of the scrotum, which leaves it more exposed to direct trauma in the inguinal region. In addition, its highest incidence rate is in the age group of 10-30 years and, among all causes, sports activities are responsible for more than half of all cases of testicular injury [1].
It is important to mention that patients with scrotal trauma usually present emergently, and rapid and accurate diagnosis is necessary to guide treatment and prevent testicular necrosis [2].
Intratesticular pseudoaneurysm is a rare testicular complication, not only in trauma. It is characterized as a blood leak that is surrounded by a pseudocapsule [1,3].
There are only 4 reports of intratesticular pseudoaneurysms described in the literature, this being the second report after trauma. Thus, the authors seek, through this case report, to discuss the diagnosis, evidence indication for complementary diagnostic examination and the presentation of a rare case of intratesticular pseudoaneurysm, after blunt trauma in the scrotal region during sports practice.
CASE PRESENTATION
A 19-year-old male patient sought medical care 48 hours after blunt trauma to the scrotal region during a soccer match, complaining of pain in the region. On physical examination, he presented swelling of the scrotum on the right. Doppler echography of the scrotum showed: enlarged right testis, with mild diffuse hypoechogenicity, with an area of intratesticular hematoma in its lower portion measuring about 23 x 12 mm, containing an ectatic vascular structure inside the hematoma, with arterial flow and turbulent in the study with Spectral Doppler, suggesting vascular trauma with pseudoaneurysm formation. In addition, it was not possible to define the tunica albuginea on the image, as it was adjacent to the lateral portion of the hematoma, suggesting a focus of rupture. Testicular flow was preserved. A heterogeneous collection, with hematic aspect, measuring 5.7 x 3.8 x 6.7 cm (estimated volume of approximately 80 ml) was observed in the scrotum, adjacent to the right testis. The left testis had normal morphology, regular contours, homogeneous echotexture, with no signs of solid or cystic focal lesions in its interior. Both epididymis with apparently preserved morphology and dimensions.
Therefore, an image suggestive of rupture of the tunica albulgina of the right testis was concluded, associated with intratesticular hematoma and vascular lesion with formation of pseudoaneurysm. There was also mild/moderate hematocele. After the result, the patient was referred for surgery, in which the hematoma was explored with drainage and marsupialization. Drainage of the hematocele and orchidopexy was also performed.
A control examination, a Doppler ultrasound (US), of the scrotum (Image 4) was performed 48 days after the event, showing: right testis with a hypoechoic area in the lower portion measuring 10x5mm, without flow on Doppler study; left testicle, right epididymis and left epididymis showed preserved dimensions, contours and echotexture.
DISCUSSION
The main mechanism of blunt trauma injury is the crushing of the testicle against the pubic symphysis or between the thighs. The right testis is more likely to be injured by this mechanism, due to its anatomical location slightly superior to that of the left testicle in most men [4].
Intratesticular pseudoaneurysm is characterized by a rupture of the intima of the wall leading to a dilatation that is surrounded and contained only by the tunica adventitia, forming a pseudocapsule [5].
The main mechanism of injury from blunt trauma is crushing the testicle against the pubic symphysis or between the thighs. The right testicle is more likely to be injured by this mechanism, due to its anatomical location slightly superior to that of the left testicle in most men [4].
The intratesticular pseudoaneurysm is characterized by a rupture of the intima of the wall leading to a dilatation that is surrounded and contained only by the tunica adventitia, in order to form a pseudocapsule [5]. This can be presented on the US as a round hypoechoic image or an anechoic focus on the testis as seen in Image 1. With Doppler, it is possible to observe a mass with turbulent flow, with a vascular pedicle. The Blood flow enters the pseudoaneurysm in systole and leaves in diastole, producing the “yin-yan signal” (image 2) [3,4,6].
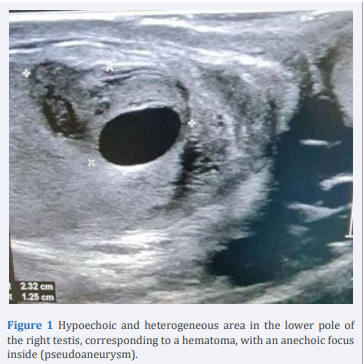
Figure 1 Hypoechoic and heterogeneous area in the lower pole of the right testis, corresponding to a hematoma, with an anechoic focus inside (pseudoaneurysm).
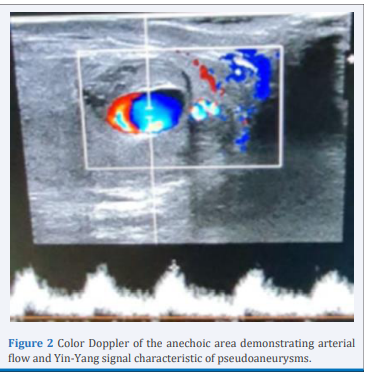
Figure 2 Color Doppler of the anechoic area demonstrating arterial flow and Yin-Yang signal characteristic of pseudoaneurysms.
There are few reports of this injury found in the literature, only one caused by trauma. This case was published in 2000, a patient victim of blunt trauma presented intratesticular hematoma on ultrasound without tearing the tunica albuginea. In addition, it revealed an anechoic area measuring 11 mm in diameter and turbulent arterial flow. The treatment of choice was conservative with periodic scrotal ultrasound [5].
Two other reported cases of intratesticular pseudoaneurysm were due to a secondary lesion to orchitis. The case reported by Bangash, the patient had a clinical picture of pain with a history of infection by the Coxsackie virus. On US examination, areas of heterogeneous echotexture and in the vicinity of turbulent arterial flow. In this case, conservative treatment with periodic US was also chosen. Repeat US at 3 weeks showed resolution of the pseudoaneurysm and reduction in size in the heterogeneous region [6].
The case published by Mujoomdar in 2007 is described as a ruptured intratesticular pseudoaneurysm in a patient who originally presented with clinical and imaging findings compatible with orchitis. The patient was admitted to the emergency department complaining of acute and progressive scrotal pain. In the first testicular US, it showed changes in echogenicity with increased blood flow to the lower pole of the left testis. After two days of evolution, the testicle was enlarged, painful and hard. The ultrasound examination showed an area of 3 cm of echogenicity and also a turbulent arterial flow. The findings were consistent with intratesticular pseudoaneurysm and hemorrhage. This patient underwent left orchiectomy to exclude a neoplastic lesion [7].
The treatment of intratesticular pseudoaneurysm can be conservative or surgical, depending on the size and severity of symptoms [4]. Patients who have the rupture surgically repaired within 72 hours have 80% testicular recovery, otherwise orchiectomy may be necessary in 50% of cases [5]. In conservative treatment, periodic scrotal ultrasound should be performed to monitor possible sequelae in patients who did not undergo surgery [5].
As found in the literature, in the four case reports of intratesticular aneurysm, both surgical and conservative treatment were instituted. The first, published in 1994 by Ohmori K. and Isokawa Y., refers to a 51-year-old patient with no history of trauma or inflammation, whose treatment was surgical [8]. Two cases of intratesticular aneurysms were secondary to orchitis, in one of them, by choice of the patient, the treatment was conservative with serial ultrasounds for follow-up, while in the other the choice was for orchiectomy to exclude a neoplastic lesion [6,7]. Finally, the last case found in the literature, similar to ours, caused by blunt trauma, was chosen for conservative treatment with periodic scrotal ultrasounds due to the integrity of the tunica albuginea [5].
In the case presented, the procedure defined by the clinical staff was to perform surgery (orchidopexy, drainage of the hematoma and marsupialization of the same) with conservative treatment of the pseudoaneurysm and testicular preservation.
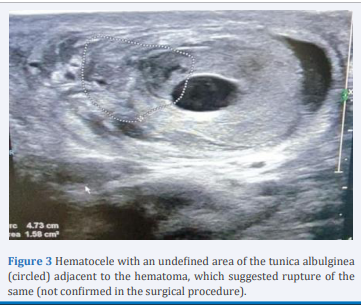
Figure 3 Hematocele with an undefined area of the tunica albulginea (circled) adjacent to the hematoma, which suggested rupture of the same (not confirmed in the surgical procedure).
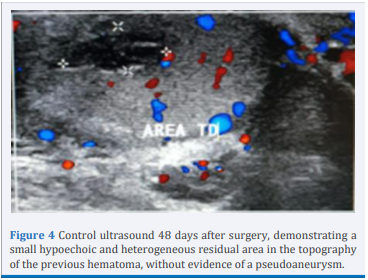
Figure 4 Control ultrasound 48 days after surgery, demonstrating a small hypoechoic and heterogeneous residual area in the topography of the previous hematoma, without evidence of a pseudoaneurysm.
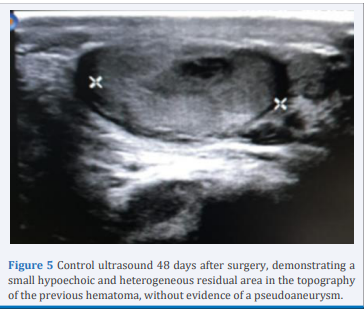
Figure 5 Control ultrasound 48 days after surgery, demonstrating a small hypoechoic and heterogeneous residual area in the topography of the previous hematoma, without evidence of a pseudoaneurysm.
ACKNOWLEDGEMENTS
Mariana RS, Laura ERH, Bruno PM and Mariana MC participated in the preparation of the manuscript. Yeda S guided the entire process. All authors participated in manuscript revisions, read and approved the final version of this article.









































































































































{kind=link}