Laparoscopic Treatment of Upper Urinary Tract Stones: About 33 Patients
- 1. Department of Urology B, Mohamed V University, Morocco
Abstract
Background: The aim of this study was to analyze the feasibility and effectiveness of laparoscopic treatment of upper urinary tract stones through the experience of urology department B.
Methods: We retrospectively and monocentrically selected patients who underwent laparoscopic treatment of upper urinary tract stones from January 2016 to December 2020. The collection was carried out on archived files. The endpoint was the occurrence of complications, the duration of the operation, the rate of SF and the length of hospitalization.
Results: A total of 33 patients were included in our series. The average age of our patients was 53 years old. There is a male predominance: 13 female patients (39.6%) for 20 male patients (60.4%). During the study period, 33 interventions involving the treatment of upper urinary tract stones were performed in our department, which is divided into 16 (48.5%) ureterotomy, 3 (9.1%) nephrotomy, 13 (39.4%) pyelotomy and 1 (3%) ureterotomy and pyelotomy. In our series, the mean operative time was 118.2 min. Estimated blood loss averaged 100ml with extremes of a few milliliters to 130ml. Intraoperative complications were reported in 2 (6.1%) patients, a conversion was necessary in 6 cases (18.2%). The postoperative period was simple in 28 (84.8%) patients with an average hospital stay of 4.8 ± 2.2 days with extremes of (2-15 days). It’s estimated that resuming normal physical activity takes an average of 3 weeks. The postoperative complication rate according to Clavien-Dindo was 15.1%. The rate of SF (Stone-free) in our series was 91%.
Conclusions: With a high SFR rate of up to 91% and a low complication rate, laparoscopic ureterotomy and pyelotomy are safe techniques that provide rapid recovery and may be the first treatment option for patients with large stones. Ureters, as well as for those with a history of primary treatment failure.
Keywords
• Laparoscopy
• Stone-free
• Urinary Stones
CITATION
Maachi Y, Boustani A, lalaoui AS, Slaoui A,Karmouni T, et al. (2024) Laparoscopic Treatment of Upper Urinary Tract Stones: About 33 Patients. J Urol Res 11(3): 1155.
ABBREVIATIONS
CT scan: Computed Tomography Scan; HU: Hounsfield Unit; LRPL: Laparoscopic Retroperitoneal Pyelotomy; PCNL: Percutaneous Nephrolithotomy; SF: Stone-free; SWL: Shock wave Lithotripsy; US: Ultrasonography.
INTRODUCTION
Urolithiasis is a common condition that affects a young population and is characterized by its frequent recurrences. The surgical treatment of urinary stones has changed considerably over the past 20 years. Advances in technology have revealed a new therapeutic arsenal, dominated by shock wave lithotripsy (SWL) and endourology, which have completely supplanted open surgery. The choice of which technique to use is guided by the characteristics of the stone, the route of excretion and the patient. In general, SWL and endourology can treat the majority of stones. Today, the emergence of laparoscopic surgery in urological practice by reproducing identically the basic gestures of open surgery, allows laparoscopy to establish itself as an attractive minimalist effective therapeutic alternative. It reduces complications related to conventional surgery with all the advantages of the laparoscopic approach which can be carried out either by transperitoneal abdominal way, or by retroperitoneal lomboscopic way. The purpose of this study is to study the feasibility and effectiveness of laparoscopic treatment of upper urinary tract stones and especially its complications through the experience of the urology department B of the CHU Ibn Sina.
MATERIALS & METHODS
We retrospectively analyzed a cohort of patients treated in our urology department B at Ibn Sina Hospital in Rabat for laparoscopic treatment of upper tract urinary stones between January 2016 and December 2020. During this study period, different surgeons operated 33 patients on. All procedures were performed by transperitoneal way. All patients admitted to urology department “B” for laparoscopic treatment of upper tract urinary stones (kidney and ureter) were included in this study. We reported intraoperative data as follows: length of stay, operative time, estimated blood loss, transfusion rate and intraoperative complications. The spectrophotometric analysis of stones was not available. All patients gave their free and informed consent. A rigorous statistical methodology made it possible to collect data concerning the parameters studied. Statistical analysis was performed using IBM SPSS Statistics 20 software. Quantitative values are expressed as mean (± standard deviation). Qualitative values are expressed as numbers (percentages).
RESULTS
The age of the patients is between 27 and 72 years old, a median age of 53 ± 13 years old. There is a male predominance: 13 female patients (39.6%) for 20 male patients (60.4%). The sex ratio is 1.53 male to female. The majority of patients had a medical history that included hypertension (high blood pressure) in 10 patients, diabetes in 6 patients, and chronic renal failure in 2 patients. Regarding the history of lithiasis, 10 patients had SWL and 3 patients had percutaneous nephrolithotomy (PCNL). Regarding the surgical history, only 4 patients had pyelotomy by open surgery. The most frequent clinical presentation is low back pain in 22 patients. They are isolated in 19 patients and associated with hematuria in 3 patients. Clinical examination found lumbar tenderness in 13 patients, while 20 patients had a strictly normal clinical examination.
The average creatinine is 22.8 ± 51.8 mg/l ranging from 6 to 257 mg/l. Abdominal radiography showed a stone on kidney area in 31 patients [Figure 1].
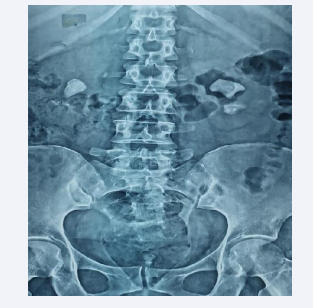
Figure 1: Abdominal radiography showing bilateral stones in the kidneys.
Renal ultrasonography (US) was performed in all patients; it revealed pelvic and calyx dilation and the presence of lithiasis in 15 patients, pelvic and calyx dilation without visible lithiasis in 18 patients. US was systematically supplemented by CT scan [Figure 2],
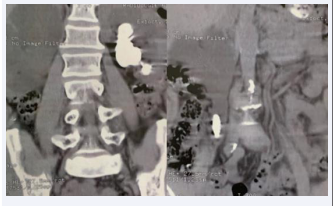
Figure 2: Frontal sections on uroscanner showing a left pyelic calculus and a right ureteric calculus.
which found pelvic stones in 14 patients, ureter stones in 16 cases, 1 pelvic-ureter stone and calyx stone in 2 patients. The mean size of the urinary stones was 26 mm ± 8.8 (between 13 and 55 mm), the mean density was 1064.7 ± 256 HU (ranging from 500 to 1520 HU), the number of stones was 1 to 3. Fourteen patients had a right localization while 18 had it on the left and bilateral localization in 1 patient. Hydronephrosis was present in 31 patients. The anatomical abnormalities observed are the single kidney in 2 cases and pelvic renal ectopia in 1 patient.
All patients were operated under general anesthesia. Twenty three patients received antibiotic prophylaxis before induction. Only 10 (30.3%) patients received antibiotic prophylaxis adapted to the antibiogram. Preoperative drainage was provided by the double J catheter in 29 (87.9%), nephrostomy in 3 patients and JJ and nephrostomy in 1 patient. Hasson procedure (open-coelio) was performed in 20 patients and the Veress needle puncture in 13 patients. The following parameters were studied for each patient: operative time, blood loss, intraoperative complications, postoperative complications and hospital stay. During the study period, 33 interventions involving the treatment of upper urinary tract stones were performed in our department, which is divided into:
- 16 (48.5%) ureterotomy
- 3 (9.1%) nephrotomy
- 13 (39.4%) pyelotomy
- 1 (3%) ureterotomy and pyelotomy.
The mean operative time was 118.2 ± 38.4 minutes with extremes of (72-240 minutes). Estimated blood loss averaged 100 ± 20 milliliters with extremes of a few milliliters to 130 milliliters. Intraoperative complications were reported in 2 patients (renal arterial trunk involvement and parenchymal hemorrhage) requiring conversion to open surgery. It was also performed in front of 2 cases of adhesions (at the time of dissection) due to peri-ureteritis, one case of stone migration and one case of intra-sinus renal pelvis. Postoperatively, all patients received a minor analgesic (paracetamol: 3g/day for 48 hours on average), without recourse to opioids. The average time for transit recovery was 2.40 ± 1.81 days with extremes of 1 to 5 days. All patients resumed a normal diet from the first day. The drain was removed within an average of 2.5 ± 0.81 days with extremes of 1 to 5 days. Bladder catheter was removed on the second postoperative day with a maximum delay of 20 days in patients with a urinary fistula. Postoperative follow-up was simple in 28 patients with an average hospital stay of 4.8 ± 2.2 days with extremes of 2 to 15 days.
DISCUSSION
Urolithiasis is a frequent and recurrent condition, which mainly affects young adults. It represents a public health problem generating significant expenditure. In the literature, surgery is no longer appropriate, its indications have greatly diminished; 5 to 10% of current indications while 90% of urolithiasis are treated by new technics [1].
Advances in endoscopic surgery and extracorporeal lithotripsy have made indications for open surgery rare. Since the advent of these modern techniques, open surgery for ureteric stones has become almost obsolete and is no longer perfomed in the majority of urology centers [2,3]. In developing countries, including Morocco; the cost, the lack of equipment and the number of operations necessary for the extraction of a stone by modern technics, namely: SWL, ureteroscopy and PCNL, mean that open surgery still has a place in the management of ureteric stones. However, the high morbidity is a major drawback of open surgery, which makes the laparoscopic approach a very effective minimally invasive alternative [4].
No difference in terms of analgesia, hospital stay, duration of return to activity and aesthetic result is noted between these minimally invasive surgical techniques [3]. Skrepetis [5], in 2001 compared a series of 18 laparoscopic transperitoneal ureterotomies with 18 open surgery ureterotomies. He found a net benefit in favor of the laparoscopic approach in terms of hospital stay and recovery. He concluded that laparoscopic surgery should be preferred over open surgery for teams experienced in laparoscopy. Goel and Hamel demonstrated the superiority of laparoscopic retroperitoneal ureterotomy over the open route in terms of analgesic consumption (41.1 mg Vs
96.6 mg pethidine), short hospital stay (3.3 days Vs 4, 8 days) and recovery (1.8 weeks Vs 3.1 weeks). The authors found no significant difference in terms of operative time and blood loss [5].
In our series, the first transperitoneal technique is the one we favor for all our patients, like FEYAERTS [6], from the Edinburgh team or EL FEEL [7], this is linked to the largest space and comfort offered by this technique. However, this approach still requires significant detachment and manipulation of the colon which is potentially dangerous. Intraoperatively, the volumes of blood loss reported are very low in most series as in ours (54 ± 49.64cc). The average running time ranges from 60-180mins, 165 ± 69.22min in our series. After stone extraction, closure of the ureterotomy is now systematic by all the authors. The ureteral catheter previously placed in the ureter allows more precise suturing of the ureterotomy. Most authors recommend drainage [3]. In our series, 30 patients underwent ureteral drainage by a double J stent and 3 patients underwent nephrostomy. In the series published by Gaur et al [8], of 101 cases operated on via the retroperitoneal route, the mean operating time was 79 minutes; the operation was successful in 93 patients. Non-opioid analgesics controlled the pain. Recently, Nouira et al. [9], reported 6 cases of retroperitoneal ureterotomy which were performed successfully. The average operative time was 160 minutes; the only complication was an urinoma. None of our patients benefited from this surgical approach and there is no comparative study in the literature concerning the trans and retroperitoneal routes.
PARK et al. [10], reported that for a stone of more than 1 cm treated with SWL, the rate of SF drops from 84% to 42%. The success rates evaluated for stones smaller than 1 cm were 85 to 87% for the proximal and middle ureter and dropped to 76% for stones larger than 1 cm [11].
To our knowledge, no study comparing ureteroscopy and laparoscopy has yet emerged, but the laparoscopic approach could be an alternative to stones inaccessible in ureteroscopy and to large stones (> 15 mm) where the rates of stone-free are low. The average stone size tolerated is 16 mm in the GAUR series [8], as in our series (15.83 ± 6.31 mm). The large hard stone blocked at the level of the pelvic-ureteral junction and above the crossing of the large vessels is currently a better indication for a laparoscopic approach [8-12,13]. The stone blockage time, localization as well as urinary tract integrity (stone embedded in the ureter) are arguments that may suggest laparoscopic surgery first. Laparoscopy is also indicated in obese patients and those with a morphological abnormality of the ureter.
Goel and Hemal [14], studied 16 cases of laparoscopic retroperitoneal pyelotomy (LRPL) and 12 cases of PCNL for pelvic stone. This study set initially to demonstrate the feasibility of pyelotomy by retroperitoneal approach, did not interest that much urologists, because over a period of 7 years, only 16 cases of LRPL were performed, while 500 cases of PCNL were performed. The retrospective comparison of these two groups showed that there was no significant difference in blood loss, length of hospitalization and recovery time which were (173.9 ml; 3.8 days and 12 .7 days) for LRPL versus (147.9 ml, 3 days and 9.8 days) for standard PCNL. However, if the success of the treatment of urinary stones is defined by the absence of a residual fragment whose existence increases the risk of recurrence beyond 50%, laparoscopic pyelotomy makes it possible to obtain a rate without stones identical to that of PCNL and significantly superior to open surgery.
In general, it is accepted that the trans and retro-peritoneal approaches of pelvic stones are equivalent in terms of surgical efficiency, if there are differences between the two, they must relate to postoperative morbidity and technical difficulties, their results are comparable to those of NLPC, and significantly better than those of open surgery.
CONCLUSIONS
With a high SFR rate of up to 91% and a low complication rate, ureterotomy and laparoscopic pyelotomy are reliable techniques that provide rapid recovery and may be the first treatment option for patients with large ureteral stones, as well as for those with a history of primary treatment failure. However, several multicenter prospective series may be necessary to validate these results.
REFERENCES
- Rezki H. Therapeutic aspects of urolithiasis Thesis of medicine, Casablanca, 2001, N° 53.
- Paik ML, Resnick MI. Is there a role for open stone surgery?. Urol Clin North Am. 2000; 27: 323-331.
- Kittinut K, Suthep P. Laparoscopic ureterolithotomy: its role and some controversial technical considerations. Int J Urol. 2006; 13: 206-210.
- Skrepetis K, Doumas K, Siagakas I, Lykourinas M. Laparoscopic versus open ureterolithotomy. A comparative study. Eur Urol. 2001; 40: 32-36.
- Goel A, Hemal AK. Upper and mid-ureteral stone: a prospective unrandomized comparison of retroperitoneoscopic and open ureterolithotomy. BJU Int. 2001; 88: 679-682.
- Feyaerts A, Rietbergen J, Navarra S, Vallancien G, Guillonneau B. Laparoscopic ureterolithotomy for ureteral stones. Eur Urol. 2001; 40: 609-613.
- EL Feel A, Abouel Fettouh H, M Abdel Hakim A. Laparoscopic transperitoneal ureterolithotomy. J Endourol. 2007; 21: 50-54.
- Gaur DD, Trivedi S, Brabhudesai MR, Madhusydhana HR, Gopichand M. Laparoscopic ureterolithotomy: technical considerations and long-term follow-up. BJU Int. 2002; 89: 339-343.
- Nouira Y, Kallel Y, Binous MY, Dahmoul H, Horchani A. Laparoscopic retroperitoneal ureterolithomy: first experience and review of literature. J Endourol. 2004; 18: 557-561.
- Park H, Park M, Park T. Two-years experience with ureteral stones: extracorporeal shockwave lithotripsy vs ureteroscopic manipulation. J Endourol. 1998; 12: 501-504.
- Yadav R, Kumar R, Hemal AK. Laparoscopy in the management of stone disease of urinary track. J Minim Access Surg. 2005; 1: 173-180.
- Kahn RI. Endourological treatment of ureteral calculi. J Urol. 1986; 135: 239-243.
- Hemal AK, Goel A, Goel R. Minimally invasive retroperitoneoscopic ureterolithotomy. J Urol. 2003; 169: 701-705.
- Goel A, Hemal A K. Evaluation of the role of retroperitoneoscopic pyelolithotomy and its comparison with percutaneous nephrolithotripsy. Int Urol Nephrol. 2003; 35: 73-76.
- Jeong B C, Park H K, Byeon S S, Kim H H. Retroperitoneal laparoscopic ureterolithotomy for upper ureter stones. J Korean Med Sci. 2006; 21: 441-444.
- Sahin S, Aras B, Eksi M, Sener NC, Tugcu V. Laparoscopic ureterolithotomy. JSLS. 2016; 20: 2016.
- Simforoosh N, Radfar M H, Valipour R, Dadpour M, Kashi A H. Laparoscopic pyelolithotomy for the management of large renal stones with intrarenal pelvic anatomy. Urol J. 2020; 18: 40-44.
- Abdel Raheem A, Alowidah I, Hagras A, Gameel T, Ghaith A, Elghiaty A, Althakafi S, et al. Laparoscopic ureterolithotomy for large proximal ureteric stones: surgical technique, outcomes and literature review. Asian J Endosc Surg. 2021; 14: 241-249.
- Choi J D, Seo S I, Kwon J, Kim B S. Laparoscopic ureterolithotomy vs ureteroscopic lithotripsy for large ureteral stones. JSLS. 2019; 23: 2019.
- Radfar M H, Dadpour M, Simforoosh N, Basiri A, Nouralizadeh A, Shakiba B, et al. Laparoscopic pyelolithotomy in patients with previous ipsilateral renal surgery. Urologia. 2021; 88: 41-45.









































































































































{kind=link}