Modalities for the Management of Tumors in the Superior Urinary Extraction (About 17 Cases)
- 1. University Hospital Center Ibn Rochd, Morroco
Abstract
The (TVEUS) correspond to lesions developed at the expense of the pyelocaliciel cavities or the ureter, they are of urothelial type in more than 95% of the cases. Rare, representing only 5% of all urothelial tumors, hematuria is the main clinical sign. The euro-scanner is the reference examination for the exploration of the upper urinary excretory pathway. Nephro-ureterectomy with a bladder collar remains the standard treatment for TVEUS.
Method: The objective of our work: To study the epidemiological, clinical, paraclinical anatomopathological and therapeutic characteristics of our series and to compare them with the results of the literature For this we conducted a retrospective study on 17 cases collected between January 2010 and June 2015 performed in the A5 urology department of the Ibn Rochd University Hospital in Casablanca.
Conclusion: The place of endourology has increased on the international and even national level allowing the diagnosis of small tumors which can escape radiological detection The conservative treatment is possible if one respects the indications perfectly however it imposes a motivation large number of patients due to the surveillance imposed by frequent recurrences.
Keywords
Tumors, Upper urinary excretory route, Urothelial carcinoma, Treatment
CITATION
Walid B, Chadli A, Dakir, Debbagh A, Aboutaieb R (2020) Modalities for the Management of Tumors in the Superior Urinary Extraction (About 17 Cases). J Urol Res 7(1): 1119.
INTRODUCTION
Like the entire urinary tree, the upper excretory tract is lined with urothelial lining. It is a special multi-layered coating, also known as a “transitional” epithelium. Tumors of the Upper Urinary Excretory Route (TVEUS) correspond thus to lesions developed at the expense of the pyelocaliciel cavities or the ureter they are of the urothelial type in more than 95% of the cases.
Although of the same histological type and presenting characteristics common with bladder tumors, the main localization of urothelial carcinoma, TVEUS also have its own genetic and prognostic characteristics.
Because of this rarity and the heterogeneity of their clinical presentation, few studies have been conducted according to the established rules of evidence-based medicine.
The observation of equivalent survival rates between conservative and radical attitudes, as well as the possibilities of monitoring by improving radiological techniques are additional arguments for conservative treatment.
MATERIAL AND METHOD
This is a retrospective study, established through the use of the files of 17 patients over a 5-year period from the beginning of January 2010 to the end of June 2015. The patients were treated for TVES at the A5 urology department of the Ibn Rochd University Hospital Center in Casablanca.
During this study, we sought to compare the results of our series (in terms of epidemiological, clinical, paraclinical and anatomopathological and therapeutic characteristics) with the results of the literature, with the aim of highlighting any new data regarding the practice towards these tumors
The target population was made up of adult patients with urothelial tumors of the upper urinary tract. The excluded patients were those with a non-urothelial renal tumor lesion.
RESULTS
The age range of our patients was 40 to 85 years (50 to 75 years for women and 40 to 85 years for men). The average age was 65.3 years (64.7 years for women and 66 years for men).
The male sex was predominant with a sex ratio of 2.4. 9 of our patients (53%) were exposed to chemical poisoning from tobacco and 3 patients (17%), had a history of VT.
Gross hematuria remained the most frequent sign of these tumors 13 patients (76.4%). This hematuria was isolated in 46.1% of the cases and associated with other clinical signs in 53.9% of the cases. The discovery during the systematic follow-up of bladder tumor corresponded to the second mode of revelation in terms of frequency of these TVEUS (17.6%).
The other discovery circumstances are described in Table 1.
Table 1: Clinical sign.
| Clinical sign | Number of cases |
| Haematuria | 13 |
| Alteration of the general state | 2 |
| Lower back pain | 6 |
| Urinary tract infection and irritant sign | 2 |
| Systemic monitoring | 3 |
Regarding diagnostic delays, the average was 8 months (time between the first clinical sign and the discovery of the tumor) with extremes ranging from 3 months to 28 months
In the first intention, imaging by UROTDM was essential in this pan-compared series to UIV (70.5% vs 41.2% respectively).
The assessment highlighted 1 synchronous bilateral tumor (i.e. 5.8% of patients). The main signs found in CT and their frequency are summarized in Table 2.
Table 2: Signs found on the CT scan.
| Sign to the CT scan | Number of cases | Percentage |
| Intraluminal tissue mass | 10 | 83.4 |
| Parietal thickening | 3 | 25 |
| Ureterohydronephrosis | 2 | 16.6 |
| Lymphadenopathy | 2 | 16.6 |
A total nephro-ureterereomy was performed in 100% of the cases. the most used technique consisted of a double approach by lombotomy and against pelvic incision with removal of a bladder collar performed in 76.4% of the cases.
Segmental ureterectomy was performed in one patient, due to the bilaterality of the lesions and the presence of a synchronous infiltrating bladder lesion. Papillary-type urothelial carcinoma had been demonstrated in all of our patients. The right side was the most affected and represented (76.4%) of the cases. The single localizations concerned 14 patients or 82.3%. The multifocal localizations concerned only 3 patients or 17.7% of the cases (Graph 1).
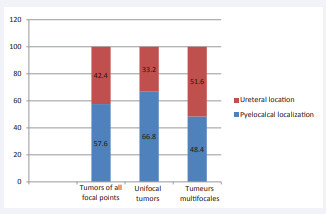
Graph 1: Representation of the frequency of tumor localizations within the ureter or pyelocaliciel cavities according to the multifocal character or not.
Low-grade tumors accounted for 41.2%
High-grade tumors accounted for 58.8%.
Lymph node involvement was found in three cases, a rate of (17.6%).
The distribution of stages and tumor grades in operated patients is described in Table 3
Table 3: Distribution of stages and tumor grades.
| Grade/Stade | PTa | PT1 | PT2 | PT3 | PT4 | CIS Isolé | Total |
| Bas grade | 1 | 3 | 3 | 0 | 0 | - | 41.20% |
| Haut grade | 0 | 2 | 0 | 0 | 0 | - | 58.80% |
| CIS isolé | - | - | - | - | - | - | 0 |
| Total | 1 (5.8%) | 5 (29.4%) | 3 (17.6%) | 8 (47%) | 0 | 0 | 20 (100%) |
The evolution was marked by the absence of post op deaths.
4 patients or 23.5% had presented operating complications:
• Renal failure due to pyelonephritis of the contralateral kidney
• Renal failure due to dysfunction of the contralateral kidney (nothing quite well differentiated with slightly laminated cortex)
• 2 cases of wall infection.
The long-term course was marked by a recurrent bladder in two of our patients
The average duration between TVEUS treatment and recurrence was 20 and 25 months
DISCUSSION
TVES is a rare tumor accounting for only 5% of the urothelial carcinomas identified worldwide. The peak incidence of TVES is between 70 and 80 years. The average age of diagnosis generally reported in historical series is 65-70 years [1].
More recent series report a tendency to diagnosis at a later age beyond 70 years in connection with the aging of the population. In Europe and the United States, the male / female ratio is 1.5 to 2.8 to 1 over the period 1997-2010 [2].
It is estimated that: approximately 12 to 30% of patients with TVES have a history of bladder tumor, approximately 8 to 13% have a synchronous bladder localization and finally 11% have both a history of bladder localization and a bladder localization concomitant with the diagnosis of TVES. The bladder recurrence rate after NUT was 31% in an international multicenter retrospective study including 1839 patients with a median follow-up of 45 months [1].
Multifocal tumor within the same upper excretory pathway is a frequent event (7-23% of cases). This multifocality can relate to a single segment of the ESV (ureter or pyelocaliciel cavities) or both [1].
Macroscopic hematuria is the most frequent symptom when diagnosing TVES (68 to 82% of cases) .On the other hand, the etiological assessment only highlights TVES in 0.3-5.3% of cases in progress isolated hematuria. The pain of the flanks and lumbar fossa represents the second symptom in terms of frequency (20 to 30% of cases). A palpable lumbar mass can correspond to very advanced pyelo-caliceal tumors or to a hydronephrotic kidney. The perception of a lumbar mass as the first clinical sign is rare and remains dependent on the morphotype of the patients. Irritant or infectious symptoms may also be present during the diagnosis. Tumors of the lower ureter prolapsed in the meatus or synchronous bladder locations (7-17% of cases), are often the cause of pollakiuria [3].
With regard to the radiological diagnosis, we have been logically witnessing for several years a decrease in the frequency of the realization of the IVU in the assessment of TVEUS. This is replaced positively and gradually by the CT scan. This goes hand in hand with the development of more precise uroscanner protocols, the appearance of multi-bar machines and the increase in performance in terms of spatial resolution [4].
Therapeutically the place of NUT was and remains preponderant in the management of TVEUS. This therapeutic gesture remains the standard treatment regardless of the location of the tumor in the excretory pathway, the surgical intervention always involves two stages. The first stage is the enlarged nephrectomy and the second stage, the ureterectomy with removal of a bladder collar [5].
Data from the literature estimates an 8.3% to 50% intra vesical recurrence rate in 50% of cases. Multifocal tumor within the same upper excretory pathway is a frequent event 7 to 23% according to the authors [6].
From a histological point of view, as suggested by the analysis of the American and Swedish registers, our findings point to an increase in the frequency of ureteral tumors over the past twenty years.
CONCLUSION
Since Albarran (1905), the understanding and management of urothelial carcinomas and TVEUS have evolved considerably. The identification of distinct carcinogenesis mechanisms between urothelial carcinomas of the bladder and those of the upper excretory pathway, in particular within the HNPCC syndromes, modifies the management of these tumors. If the epidemiological and clinical characteristics of the treated population do not seem to have changed significantly since previous local studies, the finding of an age at later diagnosis is reported here. The radiological assessment of patients with TVEUS saw the advent of sectional imaging (uroscanner) as a benchmark examination to the detriment of conventional projection imaging. The place of endo-urology has increased internationally allowing the diagnosis of small tumors which can escape radiological detection. Despite the abundant literature, it seems that the only prognostic criteria recognized today as significant are precisely the stage, grade and lymph node involvement. The standard treatment to date remains total open nephroureterectomy. The laparoscopic route seems to be equivalent in the less advanced stages.









































































































































{kind=link}