Spontenous Urethrovaginal Fistula after Advanced Pelvic Organ Prolapse
- 1. Department of Urology, University of Cincinnati, USA
Abstract
Urethrovaginal fistula is a rare occurrence with unknown prevalence, Common causes of urethrovaginal fistulas are complicated vaginal deliveries, damage to the urethra during vaginal surgery, (particularly excision of urethral diverticulum) and surgery of the anterior vaginal wall including synthetic slings [1]. Rare etiologies of urethrovaginal fistulas include vaginal hysterectomy, pressure necrosis from improperly managed long-term indwelling catheters, pelvic fracture injury causing laceration of the urethra, and local invasion from adjacent malignancies and radiation therapy [2].
Pelvic Organ prolapse (POP) is a common condition that accounts for about 400,000 surgeries annually in the United States [3]. The lifetime risk of having surgery for POP or urinary incontinence at the age of 80 is about 11.1 % [4]. Additionally, advanced POP is more likely to be symptomatic and in need for treatment. Reported POP related complications include: Recurrent urinary tract infections, urinary incontinence, urinary retention, hydronephrosis, and vaginal skin ulceration, this is in addition to the reported rare complication of bladder rupture [5-8]. In this study we present a case of spontaneous urethrovaginal fistula in an elderly lady, who didn’t receive treatment for procidentia for at least 8 years. To our knowledge this is the only reported case of urethrovaginal fistula in the presence of Pelvic Organ Prolapse.
Citation
Vinson MA, Mohamed MA, Mahdy A (2014) Spontenous Urethrovaginal Fistula after Advanced Pelvic Organ Prolapse. J Urol Res 1(3): 1014.
CASE PRESENTATION
A 79 year old woman was referred for 8 years history of POP (Figure 1).

Figure 1: Grade III pelvic organ prolapsed with Folye’s catheter in the urethra.
The patient’s past surgical history is positive for abdominal hysterectomy with bilateral salpingo-oophorectomy. She also has a history of ischemic heart disease with subsequent insertion of cardiac drug eluting stents. She was therefore kept on combination of aspirin and clopidogrel bisulfate. Given her medical condition, the referring physician attempted to treat the patient with vaginal pessary, which failed several times. Otherwise patient past history is negative for any previous vaginal or urethral trauma, surgery, infections or radiation. Few days prior to surgery, the patient developed urinary retention that was temporarily treated with Foley’s catheter. During the evaluation process, she was found to have complete procedentia with ulceration at the vaginal apex of about 2x2 cm as well as a urethral mucosal prolapse. There was also found a 1x1 cm urethrovaginal fistula. The fistula was seen at the proximal urethra and at site of deflection between the urethra and the prolapsed bladder base (Figure-2a). After extensive discussion with the patient regarding surgical options, she opted for full vaginal reconstruction because she is willing to be sexually active. After discussion with patient’s cardiologist, she was cleared for surgical correction of her prolapse. Additional work up included renal ultrasound and video-urodynamics. Renal ultrasound was negative for hydronephrosis and video urodynamics was positive for occult stress urinary incontinence and grade IV cystocele. Patient received anterior and posterior colporrhaphy, aneterior and posterior enterocele repair and bilateral sacrospinous ligament fixation. The urethrovaginal fistula was closed in layers with the utilization of the rectus fascia. The procedure was completed with perineoplasty (Figures 2-b through d). Voiding cystourethrogram (VCUG) was performed 3 weeks after surgery and confirmed absence of extravasation at the repair site. The urethral catheter was removed and patient voided to completion (Figure 2-e).
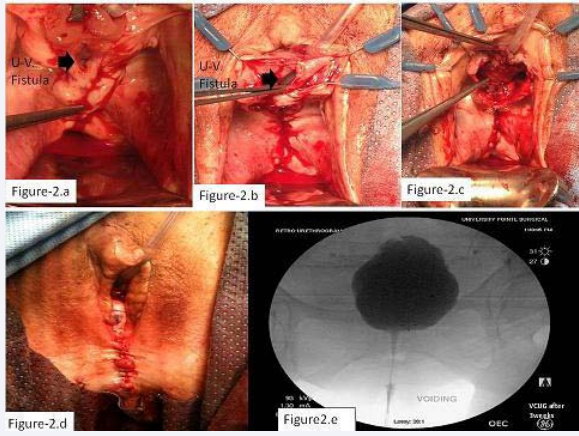
Figure 2
a) Intraoperative: urethrovaginal fistula after repair of POP.
b) Dissection of fistula margin from the periurethral fascia.
c) Rectus fascia sling (pointed to by forceps).
d) After completion of the procedure.
e) (VCUG) 3 weeks after surgery showing no evidence of extravasation, good reduction of prolapse and no evidence of bladder outlet obstruction.
The VCUG as well as vaginal examination confirmed absence of POP. After one year follow up, patient denied any urine incontinence. Vaginal exam revealed well-healed fistula site, grade I anterior vaginal wall prolapse and residual urethral caruncle. Both are asymptomatic (Figure 3-a and b). Post-void residual volume with bladder scan was 140 ml.
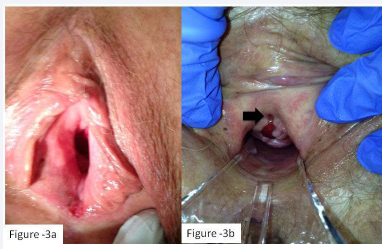
Figure 3 One year after surgery
a) Patient external genitalia.
b) Speculum examination showing granulation tissue at the 6 O’clock position of the urethral meatus and grade I Anterior vaginal wall prolapse.
DISCUSSION
Urethrovaginal fistula is an uncommon occurrence that can be a consequence of prolonged labor, complicated vaginal delivery, or injury during vaginal surgery [1]. In this case, the patient denied history suggestive of the known causes of urethrovaginal fistula. The patient has had hysterectomy which can be complicated by ureterovaginal or veiscovaginal fistula [9]. Hystrectomy is not a known cause of urethrovaginal fistula however. Furthermore, the patient has had hysterectomy several years ago and we would expect sudden onset urine incontinence after traumatic fistulas which were not the case in this patient. Vaginal pessaries were reported to cause vesicovaginal fistula, this could occur with large, long-term used pessaries [10]. Our patient has never been able to retain the tried pessaries and they all fell shortly after insertion because of her advanced POP. Traumatic catheterization is unlikely cause, because the catheter was inserted easily, urine was clear and catheter inserted only for two days.
We believe the long standing urethral kinking secondry to the advanced POP in this patient is the cause of her fistula. This conclusion is supported by the fact that her POP was of long duration. We hypothesis that prolonged urethral kinking led to local congestion and ischemia with subsequent tissue breakdown and fistula formation. This suggestion is supported by the location of the fistula site where the proximal part of the urethra was kinked. The diamond shape of the fistula also correlates with the sites of tissue folding and contact (Figure 2-b). Additionally, the edges of the fistula looked ischemic and poorly vascularized.
The patient received full reconstruction and rectus fascia sling. Given the patient age and cardiac history, one of the obliterative vaginal procedures would be the best option but the patient wanted to be sexually active which dissuaded us from vaginal obliterative surgery. She had occult stress urinary incontinence during video urodynamics so an incontinence procedure was also indicated. In the setting of fistula repair, synthetic slings are generally avoided so a rectus fascia sling was inserted in this patient. The rectus fascia sling was performed at the same time of reconstruction for different reasons; first, was to avoid the distressing post-operative urine incontinence after prolapse reduction. Second, is to utilize the sling tissue as an additional layer of support to the fistula closure. And third, is to avoid multiple visits to the operating room in this old and rather comorbid patient.
CONCLUSION
To our knowledge, this case is the first in the literature who developed urethrovaginal fistula as a complication of prolonged POP. This complication may be possibly added to the complication list of untreated POP especially if the prolapsed is prolonged and advanced.Also having this complication in mind aids in better evaluation, surgical planning and patient counseling.
REFERENCES
- Chapple CR. Urethral Diverticula, Urethro-Vaginal Fistulae, Vesico-Vaginal Fistulae. EAU Update Series. 2003; 1: 178-185
- Blaivas JG, Rajveer SP. Post-Traumatic Female Urethral Reconstruction. Current Urology Reports. 2008; 9: 397 – 404.
- Barbalat Y, Tunuguntla HS. Surgery for Pelvic Organ Prolapse: A Historical Perspective. CurrUrol Rep. 2012; 13: 256–261.
- Gerten KA, Markland AD, Lloyd LK, Richter HE. Prolapse and incontinence surgery in older women. J Urol. 2008; 179: 2111-2118.
- Dangerfielda DC, Smitha N, Snowb TM. Spontaneous Rupture of the Urinary Bladder Secondary to Total Uterine Prolapse. Clin Radiol Extra. 2003; 58: 25-26.
- Richardson DA, Bent AE, Ostergard DR. The effect of uterovaginal prolapse on urethrovesical pressure dynamics. Am J Obstet Gynecol. 1983; 146: 901-905.
- Hadar H, Meiraz D. Total uterine prolapse causing hydroureteronephrosis. Surg Gynecol Obstet. 1980; 150: 711–714.
- Tegersted G. Prevalence of symptomatic pelvic organ prolapse in a Swedish population. Int Urogynecol J. 2005; 16: 497–503.
- Ockrim JL, Greenwell TJ, Foley CL, Wood DN, Shah PJ. A tertiary experience of vesico-vaginal and urethro-vaginal fistula repair: factors predicting success. BJU Int. 2009; 103: 1122-1126.
- Kaaki B, Mahajan ST. Vesicovaginal fistula resulting from a well-cared-for pessary. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18: 971-973.









































































































































{kind=link}