Unusual Presentation of Prostatic Adenocarcinoma with Neuroendocrine Differentiation Prior to Therapy in a Nigerian: A Case Report
- 1. Department of Pathology, University College Hospital, Nigeria
- 2. 2 Department of Anatomic Anatomy, Ekiti State University, Nigeria
- 3. Department of Surgery, University College Hospital, Nigeria
Absract
Prostatic adenocarcinoma with neuroendocrine differentiation is uncommon.We present a case of prostatic adenocarcinoma with metastasis to the skull diagnosed at autopsy in a 79 year old man. The clinical assessment was varied and the differential diagnosis included benign prostatic hypertrophy, carcinoma of the prostate, carcinoma of the bladder and colorectal carcinoma. Abdomino- pelvic ultrasound showed a poorly defined huge pelvic mass which measured 19.6x12.8x 12.3 cm and the volume was 1607cm3. The serum prostate specific antigen (PSA) was 2.9ng per ml.
Autopsy findings revealed a huge tumour mass encircling the base of the urinary bladder and was adherent to it. The mass and the urinary bladder together weighed 1,650gms and measured 22x19x9.5cm. There were metastases to the inner surface of the frontal skull bone, dura and the left lung. Histologic evaluation of the tumour showed an adenocarcinoma of the prostate with a Gleason’s score of 8. It was immunoreactive to PSA, AE1/AE3, S100 protein and neurone specific enolase (NSE) which indicated neuroendocrine differentiation.
This case illustrates the challenges of diagnosis clinically and the possibility of neuroendocrine differentiation of prostatic adenocarcinoma prior to therapy. The aggressive nature and poor prognosis of the tumour are also illustrated by this case.
Keywords
Prostatic adenocarcinoma; Neuroendocrine differentiation; Nigerian
Citation
Babatunde TO, Omonisi AE, Ogun GO, Takure AO, Ajamu OJ (2017) Unusual Presentation of Prostatic Adenocarcinoma with Neuroendocrine Differentiation Prior to Therapy in a Nigerian: A Case Report. J Urol Res 4(1): 1079.
INTRODUCTION
The incidence of prostate cancer varies worldwide, with the highest rates found in the United States, Canada and Scadinavia, and the lowest rates found in China and other parts of Asia [1,2]. These differences are caused by genetic susceptibility, exposure to unknown external risk factor on differences in healthcare and cancer registration, or even a combination of these factors [3].
The vast majority of prostate cancers are acinar adenocarcinoma [3]. The variants of usual acinar adenocarcinoma defined in 2004 by the World Health Organization (WHO) include atrophic, pseudo hyperplastic, foamy, colloid, signet ring, oncocytic and lymphoepithelioman-like carcinomas [4]. The second group of non-acinar carcinoma histological variants of prostatic carcinoma account for 5-10% of carcinoma that originate in the prostate. These include sarcomatoid carcinoma, and neuroendocrine carcinoma3.
We report an usual case of a 79 year old man with prostatic adenocarcinoma with neuroendocrine differentiation with metastasis to inner surface of the frontal skull and other uncommon clinical manifestations.
CASE PRESENTATION
A 79 year old man retired male engineer who was referred from a private health facility and presented at the University College Hospital, Ibadan on the 3rd of September 2012 with 2years history of difficulty in micturition and 3 weeks history of body swelling. The was associated by increased frequency and nocturia which increased from D/N of 2-3/1-2 to 3-4/5.
There was urgency, terminal dribbling and a feeling of incomplete bladder emptying but there was no history of dysuria, hematuria, supra-pubic or loin pain. He was placed on some drugs at the referral centre without much improvement in symptoms and he later resorted to herbal concoction.
Three weeks prior to this presentation, he was noticed to have bilateral leg swelling, facial swelling but there was no intermittent hiccup, vomiting, change in bowel habit or sensorium and there was no skin change. He was not a known hypertensive, diabetics or asthmatic patient. There was no previous history of hospital admission or surgery. He neither smoked cigarette nor drank alcohol.
On examination at presentation revealed an elderly man with facial puffiness? He was afebrile, not pale, well hydrated but had bilateral pitting edema. Cardiovascular examination revealed a pulse of 72 beats per minute, of good volume and blood pressure of 110/60mmHg. Abdominal examination revealed a 20 weeks size suprapubic mass; one could get above it but not below it. There was no palpably enlarged organ. The chest and central nervous system examinations were essentially normal.
Digital rectal examination revealed an enlarged right lateral lobe of the prostate, firm to hard in consistency. It was not tender and the median groove was not appreciated.
A clinical diagnosis of chronic urinary retention in a patient with bladder outlet obstruction? carcinoma of the prostate with renal impairment was made.
Investigations carried out include the prostate specific antigen assay (PSA) was 2.9ng/ml. The abdomino pelvic ultrasound showed a poorly defined huge pelvic mass? prostate?? bowel. The mass measured 19.6x12.3cmm, where of 1607cm [3]. Both kidneys showed mild to moderate pelvicalyceal fullness, suggestive of back pressure changes.
On the 26th March 2013 he was brought into the resuscitation room of the emergency unit of the UCH unconscious and gasping for respiration. Active cardiopulmonary resuscitation measures were immediately commenced but all efforts at resuscitation proved abortive and he was certified dead at 6:07pm. Autopsy was requested for because the case was a coronal cases and to ascertain the diagnosis.
THE AUTOPSY FINDINGS
At autopsy, the review of the organ systems revealed a huge and firm tumour encircling the base of the urinary bladder. The tumour weighed 1,650g with multiple nodules of various sizes and shapes. Cut surface shows variegated appearance. Microscopic sections of the tumour showed an infiltrating adenocarcinoma with Gleason grade V. The tumour cells were immunoreactive to PSA, AE1/ZE2, S100, neurone specific enolase (NSE) which suggested a neuroendocrine differentiation (Figure 1-3).
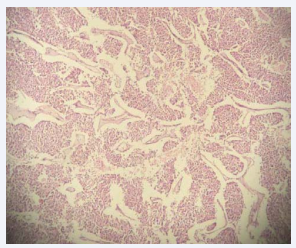
Figure 1 Photomicrograph of the prostate showing sheets and ribbons of cells.
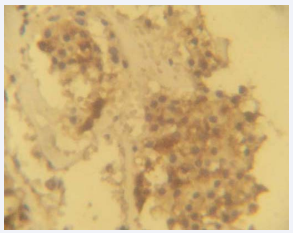
Figure 2 Photomicrograph showing positivity of the tumour cells to prostatic specific antigen (PSA) immunohistochemical staining.
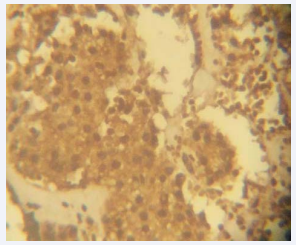
Figure 3 Photomicrograph showing the positivity of the tumour cells to Neuron Specific Enolase (NSE); a neuroendocrine marker.
There are associated calvarial metastases (Figure 4).

Figure 4 Photograph of the skull showing calvarial metastases.
The urinary bladder was dilated and had a hypertrophied wall which measured 2cm in thickness. The mucosa of the urinary bladder showed moderate to severe congestion.
The left kidney was enlarged weighed 205g and the right which weighed 100g. The capsules of both kidneys strip with ease to reveal smooth subcapsular surfaces. Cut sections showed good and poor corticomedullary differentiation on the left and right sides respectively and multiple dilated calyces which ranged in diameter from 1cm to 2.5cm.
Microscopically, section of the kidneys showed glomerulosclerosis (30%), hyalinization of some tubules, and thickening of the arterial walls. Interstitial inflammation and fibrosis. There is periglomerular fibrosis.
Both lungs show evidences of pulmonary metastasis
DISCUSSION
This case is unique because its presents some unusual manifestations of prostatic adenocarcinoma with dural metastasis, lung metastasis and skull fracture. This uncommon ways of manifestations pose some challenges in diagnosing prostate cancer. Prostate cancer is the most common malignant tumour in men and is a major research focus of pathologists, urologists and uro-oncologists [4]. The index patient in this case report first presented with history of difficulty in micturition and body swellings. In most cases of prostate cancer, a difficulty in micturition and other obstructive symptoms are the commonest clinical presentations [5]. The wall of the urinary bladder showed hypertrophy in this case.
This was a compensatory mechanism of the urinary bladder to the development of obstructive uropathy. Cancer of the prostate have been reported to initially present clinically with features of disseminated intravascular coagulopathy [6,7] and other uncommon presentations such as massive ascites and peritoneal metastasis, generalized lymphadenopathy and recurrent acute renal failure [8-10].
Certainly, the Gleason grading and scoring system since introduction by Donald Gleason in 1966 has been very useful in staging of prostatic adenocarcinoma. The essential histomorphological diagnostic attributes of the various histological variants of prostate adenocarcinoma have clinical significance [3]. The important histologic subtypes of prostate cancer are the mucinous carcinoma, signet ring cell carcinoma, adenosquamous and squamous cell carcinoma, basaloid and adenoid cystic carcinoma, sarcomatoid carcinoma, lymphoepithelioma-like carcinoma and neuroendocrine carcinoma [11].
Neuroendocrine cells were first systematically characterized in the 1980s and have been increasingly recognised as an important component of the prostate [12]. The histologic section of the tumour stained with haematoxylin and eosin as shown in Figure (3), showed the typical ribbons disposition of the tumour cells typical of neuroendocrine carcinoma. The high power examination of the tumour cells as shown in Figure (1), showed prominent nucleoli and eosinophilic cytoplasm; characteristic of neuroendocrine carcinoma. Neuroendocrine carcinoma demonstrate unique immunohistochemical staining features with antibodies against neuroendocrine markers such as chromogranin A, synaptophysin, neuron specific enolase [12].
Immunohistochemical studies as shown in Figures (2&3) showed that the tumour cells in this case shown strong, diffuse PSA positivity which confirmed a prostatic origin. The tumour cells also showed strong neuron specific enolase (NSE) positivity which is a neuroendocrine marker.
Cancer of the prostate with neuroendocrine differentiation is rarely associated with pathologic fracture of skull with intracranial metastasis [13]. This case as shown in Figures (4) shown calvarial metastases. This explained why the patient had a poor prognosis and low chance of survival because the disease was advanced at the time of presentation.
CONCLUSION
Although increasing numbers of pathologists, urologists and uro-oncologists have shown interest in prostate cancer research and management, the diverse histomorphological variants of the disease and unusual manners of presentation of prostate cancer continues to pose serious challenges to the early recognition of the disease.
This case report basically highlighted the unusual presentation of prostatic adenocarcinoma with neuroendocrine differentiation.
CONSENT
Written consent was obtained from the living next of kin of the patient before doing the autopsy.
AUTHORS’ CONTRIBUTIONS
BTO, OAE, OGO are the pathologists who performed the autopsy, examined the histology and immunohistochemistry slides. They are also involved in the writing of the manuscript. TAO and AJO are involved in the primary management of the patient.









































































































































{kind=link}