Knnowledge, Attitude and Practices on Anthrax among Animal and Human Health Professionals in Kellem Wollega Zone of Oromia Regional State, Ethiopia
- 1. Kellem Wollega Zone, Sayo Woreda Agricultural Office, Ethiopia
Abstract
Ethiopia has the 2nd largest human population in Africa and the largest livestock population on the continent. The country is mainly vulnerable to zoonotic diseases because its economy is primarily dependent on agriculture. Anthrax is a potentially fatal naturally occurring infectious disease of warm-blooded animals that primarily affects herbivorous mammals. Humans become infected incidentally through contact with diseased animals or contaminated animal products. The objective of this study aims to assess the animal and human health professionals’ knowledge, attitudes, and practices towards anthrax diseases in Kellem Wollega Zone starting from July to September, 2022. A cross-sectional study design using questionnaires were used to evaluate the animal and human health professionals of the study area on their knowledge, attitudes, and practices on anthrax starting from July to September, 2022.A total of 390 respondents participated in the questionnaire survey .Of these, 190 were animal health professionals while 200 were human health professionals working in government institutions. The overall knowledge of human health professional 59% (62%, 60.5% attitude and 56.4%) practice. The overall knowledge of Veterinarians 71% (77.8%, 67.7% attitude and 67.5%).In general, in some districts they considered anthrax as a forgotten disease. The KAP of the human health professional participants towards anthrax was lower than veterinarians. Moreover, there was no consistent understanding of the disease among the participants.
Keywords
Anthrax, Knowledge, Attitude, Practice, Kellem wollega
Citation
Getahun F (2023) Knnowledge, Attitude and Practices on Anthrax among Animal and Human Health Professionals in Kellem Wollega Zone of Oromia Regional State, Ethiopia. J Vet Med Res 10(1): 1243.
INTRODUCTION
Ethiopia has the 2nd largest human population in Africa and the largest livestock population on the continent [1]. The country is mainly vulnerable to zoonotic diseases because its economy is primarily dependent on agriculture. About 80% of households directly contact domestic animals, creating an opportunity for infection and spread of disease [2]. Zoonosis is any disease or condition naturally transmissible from vertebrate animals to humans and vice-versa [3]. Anthrax is a potentially fatal naturally occurring infectious disease of warm-blooded animals that primarily affects herbivorous mammals [4]. Anthrax is known by several names worldwide, such as charbon, wool sorter’s disease, rag pickers’ disease, malignant carbuncle, malignant pustule, and Siberian ulcer [5]. Due to its widespread distribution and its potential use as a biological weapon (bioterrorism), anthrax is also believed as a global public health threat [6]. It has a disproportionate impact on the livelihood of livestock owners. Mainly, the public health and livestock product quantity and quality in impoverished rural communities in anthrax-endemic countries are severely affected, resulting in devastating economic loss and loss of livestock product market due to reduced consumer confidence [7]. The causative agent of anthrax is Bacillus anthracis (B. anthracis), which primarily infects herbivores and secondarily humans [8,9].
The occurrence of anthrax outbreaks in a particular location mostly depends on multiple factors, which include unique characteristics of the bacterium, environmentally related features, animal densities and human activities [10,11]. Anthrax outbreaks have been associated with ecological, demographic, and sociocultural factors [12,13]. The occurrence of human cases is often highly correlated with animal anthrax outbreaks [14]. Anthrax seasons are typically characterized by hot-dry weather, with outbreaks often triggered by weather extremes such as heavy rain following a period of prolonged drought [15]. As such, a warming climate is predicted to increase anthrax risk in some areas of the world [16].During the dry season, the grass is short and animals are forced to graze closer to the ground, increasing the opportunity to ingest anthrax spores [17], especially when anthrax-infected carcasses and butchering waste have been disposed of in environments where ruminants live and graze [18]. Spores may also be spread in the environment through scavenging birds, animals, and water [19,20].
The disease is rapidly fatal in herbivores such as cattle, with some animals displaying characteristic signs of external bleeding from the nose, mouth and anus up on death. On exposure to air, bacteria released in blood and body fluids form environmentally resistant spores that can persist for decades in the soil [21]. Humans become infected incidentally through contact with diseased animals or contaminated animal products. In most (95%) cases, exposure occurs via cuts or abrasions in the skin following handling of infected animal products, such as hides or wool. This results in cutaneous lesions characterized by a raised vesicle that develops into a painless sore with black center (‘black eschar’) (WHO; 2008).Less commonly, ingestion of under cooked meat can lead to oropharyngeal or gastrointestinal disease with nausea, vomiting, abdominal pain and severe bloody diarrhea. Inhalation of spores can also lead to the respiratory form, characterized by flu-like symptoms, difficulty breathing and shock. Whereas treatment of cutaneous anthrax with antibiotics leads to recovery, ingestion and inhalation anthrax are often fatal [22].
In Ethiopia, sporadic anthrax outbreaks occur annually among livestock [23], posing health risks to people who come into contact with infected animals. Whilst the disease is recognized by Ethiopian farmers as one of the most important livestock diseases [24] and it is ranked second only to rabies according to the recent joint-ministerial zoonotic disease prioritization exercise (Pieracci EG, et al).
Generally, The KAP study conducted in Kellem Wollega zone towards anthrax disease among animal and human health professional showed that about 62% of human health professional have good knowledge, 60.5% attitude and 56.4 % practice. 77.8% Veterinarians have good knowledge, 67.7% attitude and 67.5% have good practice toward anthrax disease.
OBJECTIVE
This study aims to assess animal and human health professionals’ knowledge, attitudes, and practices (KAP) on anthrax in Kellem Wollega Zone.
MATERIALS AND METHOD
Study Area
The study were conducted in the randomly selected districts of Kellem Wollega zone; Oromia regional state, Ethiopia. Kellem Wollega Zone is found in the western part of Ethiopia. Its administrative city; the seat of administration, is called Dembi Dolo town, located about 652km to the west of Addis Ababa/ Finfinnee. The Agro ecology of the study area is Highland (26.1%), Midland (41.47%) and Lowland (32.49%). The study area is located between the latitude of 80 10’ 58” N-90 21’ 53” N and longitude 340 7’ 37’’ E-350 26’ 53” E. The annual rainfall of this zone ranges from 1200-1600ml. The total area of the zone is 10488 km2 , accounting for about 2.9% of Oromia regional State and its altitude ranges from 500-1500 meters a.s.l. The average temperature of the Kellem Wollega zone is 270 C. The study area has a huge livestock population, comfortable climate conditions for breeding animals, and most of the community is dependent on mixed Agricultural system. The zone has 12 administrative Districts and 279 Peasant Associations/Kebeles. According to the administrative data collected from all 12 districts of the zone in April/2022, the study area’s livestock population is 1,229,303 cattle (local 1,228,220 and 1,083 hybrid), 758,399 Sheep, 472,152 goats, 186,614 Equines and 2,312,300 poultry (local 1,266,321 and hybrid 1,045,979, and human population of this zone is 147,306 from which the number of male is 135,861 and that of female is 11,445. The zone has 344 veterinarians one “B” type clinic,12 type” C” clinics and 144 type” D” clinics. It has 1,114 human health professionals and 689 health extensions one general hospital and three primary hospitals, 51 health posts and 278 health gates [25,26].
Study Design
A cross-sectional study design using questionnaires were used to evaluate the animal and human health professionals of the study area on their knowledge, attitudes, and practices on anthrax starting from July to September, 2022. The question should also contain knowledge part (Causative agent, clinical sign on animal/human, transmission way on animal/human, zoonotic importance, prevention way, treatment option for animal/human, and controlling mechanism) attitudes part (awareness creation, importance of vaccination, prevention and control method) and practices part (outbreak history, biosecurity experience and biosafety experience) of the two professionals on the anthrax disease.
Study population
The study population was literate groups consisting of veterinarians and human health professionals living in selected 7 districts of Kellem Wollega zone. The larger group referred as target population covers those intellectuals living in 12 districts which represent the total districts of Kellem Wollega Zone.
Sample Size and sampling method: A total of 400 will be recruited for this study involving both animal and human health professionals consisting the sample size. The latter has been calculated considering the worst scenario on the population knowledge gap which is 50%, 95% confidence interval and 5% of desired error of the study using a formula of Thrusfield [27].
Where P expr = expected prevalence; n= is required sample; d= desired precision; and 1.96
Z-value = for 95% confidence level.Thus, the calculated total number of respondents was 384; but 16 respondents were added to increase the precision resulting 400 respondents as a total sample size.
To identify the sampling units three stage sampling technique was followed where 7 districts and 54 kebeles were identified purposively based on availability of animal and human health facilities.
The respondents were selected systematically while they get-in to their respective work station such as hospitals, health facilities, veterinary clinics and animal health posts. A total of 191 animal health and 209 of human health personnel were approached to administer the questionnaire (Table 1).
Table 1. Selected areas of the study and number of professional participate from each districts
| Selected District | Selected Keble | Animal health participant | Human health participant | Total |
| D/Dolo town | 7 | 17 | 24 | |
| Sayo District | 8 | 36 | 48 | 84 |
| Hawa Galan District | 8 | 32 | 38 | 70 |
| Sadi Chanka District | 7 | 27 | 18 | 45 |
| Dale Wabara District | 12 | 36 | 31 | 67 |
| Dale Sadi District | 12 | 32 | 35 | 67 |
| Lalo Kile District | 7 | 21 | 22 | 43 |
| Total | 54 | 191 | 209 | 400 |
METHOD OF DATA COLLECTION
Structured questionnaire were used to assess the animal and human health professionals’ knowledge, attitudes, and practices (KAP) regarding Anthrax. Besides, the respondents will be briefed about the project’s objective and will be asked for their consent before the commencement of the questionnaire. Therefore, the KAP tool should focus on the knowledge, (Causative agent, clinical sign on animal/human, transmission way on animal/ human, zoonotic importance, prevention way, treatment option for animal/human, and controlling mechanism), Attitude (awareness creation, importance of vaccination, prevention and control method) and Practice (outbreak history, biosecurity experience and bio safety experience).
Data Analysis
Both Quantitative and Qualitative data to be collected from the study area were entered into the MS-Excel spreadsheet, and each variable were analyzed using SPSS Version 26. Frequency and percentage will be taken by computing descriptive statistics. A Pearson Chi-square test will be used to determine the statistical association variables of the study, and a P-value <0.05 will be considered significant.
RESULTS
Socio-demographic characteristics of the respondents Of the total respondents 320 (80%) of them were male and 80 (20%) were Female. About 47% of the respondents were in the age group of 31-35-, 31% 25-30, 18 % 36-40 and 1% above 40. According to district level, 84 (21.5) were from sayo district followed by Hawa Galan 69 (17.7%), Dale Wabara 67 (16.9%), Dale Sadi 67 (16.2%), SC 45 (11.5%), Lalo Kile 43 (10.3%) and Dembi Dolo town 24 (6%). In related to respondent’s profession, 30 (8%) HO, 81 (20%) BSc Nurse, 94 (23.5) Diploma/Level 4 in nursing, 5 (1%) Medical. Laboratory, 19 (4.1%) DVM/MVSc, 24 (6%) BVSc, 148 (37%) diploma/level 4 in Veterinary were included in this study. The respondents for this survey were diverse and included from different professions, districts and Qualifications (Table 2).
Table 2. Knowledge of professionals on causative agent of anthrax, zoonotic nature and impact B. Anthracis spore in soil pose a direct infection for humans and livestock.
| Do you know Causative agent of anthrax | Knowledge on zoonotic nature | Do you think that B. Anthracis spores in soil pose a direct infection for humans and livestock? | |||||
| Variable | B. Anthracis | Others | Yes | No | Yes | No | |
| Sex(n=400) | Male | 274 | 46 | 293 | 27 | 215 | 105 |
| Female | 72 | 8 | 72 | 8 | 42 | 38 | |
| Age(n=400) | 25-30 | 104 | 21 | 117 | 8 | 72 | 53 |
| 31-35 | 160 | 28 | 166 | 22 | 127 | 61 | |
| 36-40 | 68 | 4 | 67 | 5 | 47 | 25 | |
| >40 | 14 | 1 | 15 | 0 | 11 | 4 | |
| Human health Profession(n=209) | Ho | 25 | 5 | 30 | 0 | 18 | 12 |
| BSC Nurse | 60 | 21 | 70 | 11 | 46 | 35 | |
| Diploma/Level 4 Nursing | 69 | 25 | 80 | 14 | 47 | 47 | |
| Laboratory | 3 | 2 | 5 | 0 | 2 | 3 | |
| Total | 157 (75.1%) | 53 (25.3 | 185 (88.5%) | 113 (54%) | |||
| Veterinarians (n=191) | DVM/MVSc | 19 | 0 | 19 | 0 | 19 | 0 |
| BVSc | 24 | 0 | 24 | 0 | 22 | 2 | |
| Diploma/level 4 vet | 146 | 2 | 137 | 10 | 103 | 44 | |
| Total | 189 (98.9%) | 180 (94%) | 11 | 143 (74.8%) | |||
Human Health Professionals
About 75% (157/209) of human health professional know causative agent of anthrax was bacteria called Bacillus anthracis and 20.5% (43/209) of them didn’t know. 88% (184/209) of professionals know as anthrax can affect animal and human while 12.4% (26/209) didn’t know. The number of professionals who know transmission ways of anthrax are 65.5% (137/209) who didn’t list ways of transmission 34.9% (73/209). Human case eating infected animal products 43.5% (87), contacting infected people and animal 25% (50). The number of professionals who know main clinical signs of anthrax on human are 64% (134) ,major of respondents list 14.6% (57) skin lesion ,7.9% (31) Fever,4.6% (18) coughing, 3.8%(15),Lack of appetite 3.3% (13) and the most preventive methods mentioned was vaccination of animal 43%(90/209) and Control methods vaccination and proper disposal of dead animals are the best ways for control (36.8% (77/209 and 18.5%(37) answer respectively. Those professionals suggests to prevent development t of anthrax spores,9.5% (19) avoid contact with infected people,9% (18) proper disposal of infected animal,1%(2) burn all infected animal,7% (14) environmental cleaning and 4.5% (9) health education described in Table 3.
Table 3. Knowledge of Human Health towards anthrax transmission, Clinical signs, Prevention and control methods and how to prevent development of spores.
| Variables | Frequency | % |
| (n=209) | ||
| Number who know anthrax transmission | 137 | 65.5 |
| Number who didn't know anthrax transmission | 73 | 34.9 |
| Eating infected animal products | 87 | 43.5 |
| Contacting infected animal | 50 | 25 |
| who know main clinical signs on human | 134 | 64 |
| Who didn’t know main clinical signs on human | 66 | 33 |
| Fever | 31 | 7.9 |
| Skin lesion | 57 | 14.6 |
| Coughing | 18 | 4.6 |
| Lack of appetite | 13 | 3.3 |
| Diarrhea | 15 | 3.8 |
| Who know prevention method | 140 | 66.9 |
| Who didn’t prevention method | 60 | 30 |
| Avoid contact with infected people | 41 | 20.5 |
| Isolation of sick animal | 9 | 4.5 |
| Vaccination | 90 | 45 |
| who know control Method | 114 | 54.5 |
| who didn’t know control Method | 86 | 43 |
| Vaccination | 77 | 38.5 |
| Proper disposal and burning of infected animal | 37 | 18.5 |
| Suggestion of professionals to prevent development of spore | 63 | 31.5 |
| Avoid contact with infected people | 19 | 9.5 |
| Proper disposal of dead animal | 18 | 9 |
| Burn all infected anthrax carcasses of animal | 2 | 1 |
| Environmental cleaning | 14 | 7 |
| Health education | 9 | 4.5 |
Veterinarians
About 98.9% (189/191) of veterinarians know causative agent of anthrax bacteria as it is Bacillus anthracis. All of Veterinarians know as anthrax can affect animal and human. The number of professionals who know transmission ways of anthrax are 73.8% (141/191) who didn’t list ways of transmission 25.7% (49/191). Animal case through contaminated soil 48.9% (93/191), drinking contaminated water5.2% (10) and 20% (38) inhalation and contact. The main clinical signs on animal 16.9% (66), un clotted dark red blood oozes from natural orifices, 16.7% (65) sudden death and 3.1(13) incomplete rigor mortis. Most of Veterinarians know prevention ways of anthrax are 83% (158/190), 67.3% (128) say vaccination is best way for prevention and others 2.1% (4) avoid contact with infected animals and 13.6% (26) isolation of sick animal was good method for prevention. About 71.5% (136) veterinarians know control method of anthrax,33.6% annual vaccination of animal,30.5% Burry and burn all suspected anthrax carcasses and 7.3% Quarantine.
Veterinarians suggests to prevent development of anthrax spore, 2.6% (5) avoid contact with infected animal, 44.2% (84) Bury all anthrax infected carcass, 13.6% (26) burn all infected carcass and 6.3% (Avoid opening of anthrax infected animal (Table 4).
Table 4. Knowledge of Veterinarians respondents towards anthrax transmission, Clinical signs, Prevention and control methods and how to prevent development of spores.
| Professionals Animal Health (n=191) | ||
| Variable | Number | % |
| Number who know anthrax transmission | 141 | 73.8 |
| Number who didn't know anthrax transmission | 49 | 25.7 |
| Drinking contaminated water | 10 | 5.2 |
| Through contaminated soil | 93 | 48.9 |
| Inhalation and contact | 38 | 20 |
| Number who know anthrax clinical signs | 144 | 75.78 |
| Number who didn't know clinical sigs | 46 | 24.2 |
| Sudden death | 65 | 16.7 |
| Un clotted dark red blood oozes from natural orifices | 66 | 16.9 |
| In complete rigor mortis | 13 | 3.1 |
| Number who know prevention methods | 158 | 83 |
| Number who didn't know prevention methods | 32 | 16.8 |
| Isolation of anthrax infected animals | 26 | 13.6 |
| Animal vaccination | 128 | 67.3 |
| Avoid contact with infected animal | 4 | 2.1 |
| Number who know controlling Mechanism | 136 | 71.5 |
| Number who didn't know controlling Mechanism | 54 | 28.4 |
| Annual vaccination | 64 | 33.6 |
| Bury and burn all suspected anthrax carcasses | 58 | 30.5 |
| Quarantine | 14 | 7.3 |
| suggestion of veterinarians to prevent development of spore | 127 | 66 |
| Avoid contact with infected animal | 5 | 2.6 |
| Bury all infected anthrax carcasses of dead animal | 84 | 44.2 |
| Burn all infected anthrax carcasses of dead animal | 26 | 13.6 |
| Avoid opening of anthrax infected animal | 12 | 6.3 |
Majority of professionals know as anthrax is zoonotic disease 92.5% human health and 94.7%veterinarians. About 35% of human health professional define zoonosis, as disease transmitted from animal to human and human to animal, 33.5% define only from animal to human and other dint know the definition of zoonosis.45.7% veterinarians define zoonosis disease trans mitted from animal to human and vice versa, 30.5% only transmitted from animal to human.9.5% of HHP said that anthrax is apriority disease of the area and 16.3% veterinarians said that as it is priority disease.49% of HHPS, Doxycycline is the best treatment for human anthrax, 22.5% Ciprofloxacillin, 7.5% immunization and about 5% generally state antibiotic. For animal anthrax 68% of veterinarians, Procaine penicillin is the best treatment, 22.1% pen-strep and 8.9% vaccination.51.5% HHP know concept of one health and 56.8% of veterinarians others didn’t know. Out of this only 24.5% and 22.6% know definition of one health they have low knowledge on this. 27 HHP and 23 veterinarians of Sayo district respondent say that as anthrax is subject of one health intervention in other district there is no one health initiative group.64% HHP and 59% veterinarians know as anthrax spore can be used as bioterrorism (Table 5).
Table 5. Knowledge of Professionals towards anthrax
| Variable | Frequency | |||
| % | Frequency | % | ||
| (n=209 | (n=191) | |||
| Do you think that anthrax can affect animal and human? | ||||
| Yes | 184 | 88 | 191 | 100 |
| No | 25 | 11.9 | 0 | 0 |
| Definition of Zoonosis | ||||
| Animal-Human and Vice versa | 70 | 35 | 87 | 45.7 |
| Only Animal-Human | 67 | 33.5 | 58 | 30.5 |
| Didn’t know definition | 63 | 31.5 | 45 | 23.6 |
| Is anthrax Priority disease in your area? | ||||
| Yes | 19 | 9.5 | 31 | 16.3 |
| No | 181 | 90.5 | 159 | 83.7 |
| Best treatment for human anthrax/Animal | ||||
| Antibiotic | 10 | 5% | ||
| Doxycycline | 98 | 49 | ||
| Ciprofloxacillin | 45 | 22.5 | ||
| Immunization/Vaccination | 15 | 7.5 | 17 | 8.9 |
| Procaine penicillin | 131 | 68 | ||
| Pen strep | 42 | 22.1 | ||
| Do you know the concept of one health? | ||||
| Yes | 103 | 51.5 | 108 | 56.8 |
| No | 97 | 48.5 | 109 | 57.3 |
| Definition of one health | ||||
| Collaboration between multi sectoral to prevent transboundary d/se and increase awareness | 49 | 24.5 | 43 | 22.6 |
| Who didn’t know | 151 | 76.5 | 147 | 78.4 |
| Do you know anthrax spore can be used for bioterrorism? | ||||
| Yes | 128 | 64 | 113 | 59.5 |
| No | 72 | 36 | 77 | 40.5 |
The last outbreak of the disease occurred in Sayo and Dale Wabara district in 2014Gc and 2017Gc respectively, there was 1 cattle in sayo and 3 cattle from dale Wabara district. The animal in the surrounding Kebeles were vaccinated and the community became aware that the disease was a serious. In human the last outbreak of the disease occurred in 2003GC in Sadi Chanka district.
Polio core group is one of the one health initiatives group works in Kellem Wollega Zone, it works in 5 districts found on the border. The aim of the organization is to educate human health professionals, veterinarians and community volunteers on one health approach. Through human health sector, diseases like polio, measles and tetanus, through animal health sector disease having zoonotic importance like anthrax, brucellosis and rabies since Jan/2020. According to the current study, only 25 Human health professionals and 23 animal health experts of sayo district experts were participated in polio core group. These professionals knowledge of anthrax is beyond that of the untrained district.
Professionals attitude, 59% of HHPs have good attitude to enhance anthrax surveillance by increasing public awareness whereas, 30.5% of them deploy animal and human health facilities. From selected District 88.9% of Veterinarians increase public awareness whereas, 8.9% of them deploy animal and public health personnel in each Keble to enhance anthrax surveillance. Both professionals have almost similar attitude to minimize livestock owners failing to report cases of anthrax by carrying out good awareness i.e. 62% and 86.3% respectively. For anthrax prevention both professionals have similar approach as vaccination has big role for prevention. Also they believe campaigning for vaccination encourages community participation in vaccination programs and vaccinating animal plays a big role in preventing anthrax from being transmitted from animals to humans. Additionally both of them advise suspected humans or animal anthrax cases to go to human and animal health facilities (90.5%, 97.9%). Both professional have good attitude on Collaboration between animal health and human health professional is good way for prevention and control of anthrax disease (81%, 89.5%).About 9.5% of veterinarians told that animal anthrax is a problem of their locality Table 6.
Table 6. Attitude and Practice of Veterinarians and Human Health Professionals
| Human Health (n=209) | Veterinarians | ||||
| (n=191) | |||||
| Question | Response | Frequency | % | Frequency | % |
| What do you think should be done to enhance anthrax surveillance? | Develop new technology | 21 | 10.5 | 4 | 2.1 |
| Increase public awareness | 118 | 59 | 169 | 88.9 | |
| Deploy animal and public | 61 | 30.5 | 17 | 8.9 | |
| health personnel in each Keble | |||||
| What do you think should be done with livestock owners failing to report cases of anthrax? | None | 60 | 30 | 8 | 1.6 |
| Aware | 124 | 62 | 164 | 86.3 | |
| Fine | 16 | 8 | 18 | 9.5 | |
| Where do you advise to go suspected humans or animal anthrax cases? | Traditional healer | 12 | 6 | 3 | 1.6 |
| Human and animal health | 181 | 90.5 | 186 | 97.9 | |
| Facilities | |||||
| Religious or other Practioners | 7 | 3.5 | 1 | 0.5 | |
| Does investing on public awareness for anthrax contributes for the prevention and control of the disease in your district or Keble? | Yes | 93 | 46.5 | 100 | 52.6 |
| No | 25 | 12.5 | 58 | 30 | |
| I don’t know | 82 | 41 | 32 | 16.8 | |
| Do you think that campaigning for vaccination encourages community participation in vaccination programs? | Yes | 159 | 79.5 | 165 | 86.8 |
| No | 30 | 15 | 3 | 1.6 | |
| I don’t know | 11 | 5.5 | 22 | 11.6 | |
| Do you think that vaccinating animal plays a big role in preventing anthrax from being transmitted from animals to humans? | Yes | 171 | 85.5 | 185 | 97.4 |
| No | 17 | 8.5 | 4 | 2.1 | |
| I don’t know | 12 | 6 | 1 | 0.5 | |
| Does Collaboration b/n animal and human health personnel is the best way for prevention and control of anthrax? | Yes | 162 | 81 | 170 | 89.5 |
| No | 18 | 9 | 20 | 10.5 | |
| I don’t know | 20 | 10 | 0 | 0 | |
| Do you think that animal or human anthrax is a problem in your locality? | Yes | 0 | 0 | 37 | 9.5 |
| No | 166 | 83 | 138 | 72.6 | |
| I don’t know | 34 | 17 | 15 | 7.9 | |
| Question for Practice | |||||
| Do you advise isolation of sick animals as an immediate and first measure to be implanted by livestock keepers to prevent the spread of anthrax? | Yes | 94 | 47 | 173 | 91.1 |
| No | 55 | 27.5 | 15 | 7.9 | |
| I don’t know | 51 | 25.5 | 2 | 1.1 | |
| What kind of precautionary measures do you think should always be in place to avoid occupational hazard? | Using PPE | 92 | 46 | 75 | 39.4 |
| Avoid opening of anthrax infected carcass | 35 | 18.4 | |||
| Who didn't list | 108 | 54 | 80 | 42.1 | |
| Do you think that dead animals from suspected anthrax should not be properly disposed; they rather should be left so that dogs and other scavengers eat them | Yes | 85 | 42.5 | 84 | 44.2 |
| No | 87 | 43.5 | 102 | 53.6 | |
| I don’t know | 28 | 14 | 4 | 2.1 | |
| Do you consider awareness creation of the community as an important initiative for prevention and control of anthrax? | Yes | 156 | 78 | 185 | 97.4 |
| No | 28 | 14 | 5 | 2.6 | |
| I don’t know | 16 | 8 | |||
| Have you had any experience of touching the blood of a severely sick animal without an adequate PPE? Or touching a patient’s wound/skin rush without adequate PPE? | Yes | 37 | 18.5 | 100 | 52.6 |
| No | 163 | 81.5 | 90 | 47.3 | |
More than 46% of human health professionals have low practice place to avoid occupational hazard by using PPE, 57% of veterinarians have good practice to avoid occupational hazard, 39% using PPE, 18.4% said that Avoid opening of anthrax infected carcass is good practice to avoid occupational hazard.81.5% of human health professional protect themselves touching a patients wound/skin rush without PPE.47.3% of veterinarians have low practice touching the blood of severely sick animal without an adequate PPE. (Figure 1).
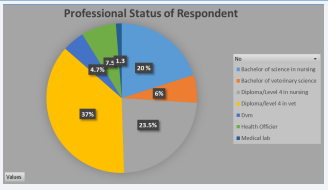
Figure 1: Professional status of respondent.
DISCUSSION
The current study applied on a broad concept towards anthrax disease knowledge, attitude and practices among Veterinarians and human health professionals of Kellem Wollega zone of Oromia regional state.
In the current study, 80% of professionals are male and 20% of them are female, it shows that males are more educated than female. Most respondents fall in age between 31-35% years of age (47%),
Over all knowledge of human health professional toward anthrax disease 62% and veterinarians,77.1%.The proportion of professionals who knew the cause, zoonotic nature, and knowledge of at least one (clinical signs mode of transmission, prevention methods and controlling methods) of the anthrax was 77.5%. Hence, when compared to other similar studies report of Asha A et al. [28], who reported (91%) in Sodo zuriya District of wolaita zone the result found is less than, but when compared with the Munang, et.al;2020 who reported 55.7% in Northern Ethiopia/Tigray Region, the result found to be much higher. 49% of HHPS, Doxycycline is the best treatment for human anthrax, Over all knowledge of human health professional toward anthrax disease 62% and veterinarians,77.1%.The proportion of professionals who knew the cause, zoonotic nature, and knowledge of at least one (clinical signs mode of transmission, prevention methods and controlling methods) of the anthrax was 77.5%. Hence, when compared to other similar studies report of Asha A et al. [28], who reported (91%) in Sodo zuriya District of wolaita zone the result found is less than, but when compared with the Munang, et.al;2020 who reported 55.7% in Northern Ethiopia/Tigray Region, the result found to be much higher. 49% of HHPS, Doxycycline is the best treatment for human anthrax, (Figure 2).
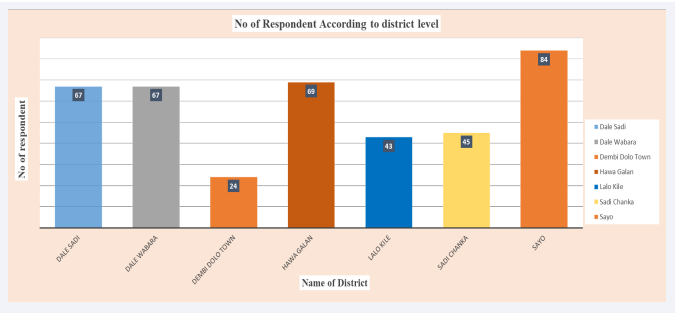
Figure 2: Number of respondent according to District.
Professional attitude, over all attitude of human health professionals who participated in this study 60.5% and veterinarians 67.7%. Generally, 73.5% have good attitude to enhance anthrax surveillance by increasing public awareness whereas, 20% of them deploy animal and human health facilities and 6.4% of them have an attitude of new technology should be invented to perform anthrax surveillance. Both professionals have almost similar attitude to minimize livestock owners failing to report cases of anthrax by carrying out good awareness. For anthrax prevention both professionals have similar approach as vaccination has big role for prevention. Also they believe campaigning for vaccination encourages community participation in vaccination programs and vaccinating animal plays a big role in preventing anthrax from being transmitted from animals to humans. Additionally both of them advise suspected humans or animal anthrax cases to go to human and animal health facilities. Both professional have good attitude on Collaboration between animal health and human health professional is good way for prevention and control of anthrax disease. About 9.5% Veterinarians told that animal anthrax is a problem of their locality. On the other hand, similar survey done in Tigray Region disclosed about 9.8% community members taught that animal anthrax was a severe problem of their locality. Romha G et al [29]. Knowledge, Attitude and Practice towards Anthrax in Northern Ethiopia:
In general, Over all practice of human health professional 56.4% while the veterinarians over all practice 67.5%.Totally, 68.4% of professional have good practice they advise isolation of sick animals as an immediate and first measure to prevent spread of anthrax.81.5% of human health professionals were using PPE while serving human but in case of animal health professional 47.3%.The finding of this survey also indicated that PPE usage among professionals was also found to be very low. However, the Proportion of human health professional workers using PPE was found to be better than animal health workers. This is similar with Asha A, et. al ;(2021) in Sodo zuriya District of wolaita zone. This could be because there will be insufficient PPE supply by government bodies in veterinary care institutions, lack of willingness of professionals to use PPE, and absence of strict directive, which enforce PPE usage in the veterinary clinic.
CONCLUSIONS AND RECOMMENDATION
In general, in some districts they considered anthrax as a forgotten disease. The KAP of the professional participants towards anthrax was lower than veterinarians. Moreover, there was no consistent understanding of the disease among the participants. The study also revealed that the participants did not get adequate and continuous training regarding the disease. The security problems in the area or in the zone have also impacted the KAP of the professionals towards the disease. For security reasons, various training projects are currently less involved in the Zone. It is the responsibility of the government and the experts to improve this problem. Based on the above, the following were recommended:
1. Institutional and human resource (veterinarians and medical professionals) capacity-building efforts should be strengthened to diagnose zoonotic diseases like anthrax for early outbreak detection and subsequent interventions.
2. Strengthen the collaboration between veterinarians and human health professionals trained on zoonotic diseases and strongly raise awareness about the diseases about how they are transmitted and their symptoms in animals and humans as well as prevention strategies.
3. Both professionals focus on a way to share information and make it clear.
4. There is an information gap in some districts, so coordinate and share data with others. example, outbreak occurrence recording
5. As much as possible, one health initiative group should create awareness for all districts in the same way.
REFERENCES
3. World Health Organization. Zoonosis. 2020
4. World Health Organization. Anthrax in humans and animals- 4th ed. [Internet] .Geneva, Switzerland: WHO; 2008.
5. World Organization for Animal Health. Anthrax. 2018
8. Hugh-Jones M, Black burn J. The ecology of Bacillus anthracis. Mol Aspects Med. 2009; 30: 356–67.
11. Hugh-Jones M, De Vos V. Anthrax and wildlife. Rev Sci Tech. 2002; 21: 359–83.
21. P.C.P. Turn bull WHO Anthrax working Group. Anthrax in humans and animals (4th Ed.) World health organization, Geneva (2008).
23. Bahiru G, Bekele A, Seraw B, Boulanger L, Ali A. Human and animal anthrax in Ethiopia: A retrospective record review. 2009–2013. Ethiop.Vet. J. 2016; 20: 75–85.
25. Kellem Wollega Zone Agriculture Office,2022
26. Kellem wollega Zone Human Health Care,2022
27. Thrusfield, M. Veterinary epidemiology. 2nd Edition, Blackwell Science, Oxford, 2005; 117-198.







































































































































{kind=link}