Review on the Economic Impacts of Lumpy Skin Disease of Cattle and Its Prevention and Control Strategies in Ethiopia
- 1. Addis Ababa University College of Veterinary Medicine and Agriculture, Ethiopia
Abstract
Lumpy skin disease (LSD) is an infectious disease of cattle, caused by a Lumpy Skin Disease Virus. It is an economically important viral disease of cattle affecting all ages and breeds that can be prevented by vaccination in endemic regions including Ethiopia. LSD is an OIE listed disease because of considerable financial losses and in Ethiopia due to the endemic nature of LSD; the country is facing serious difficulties in exporting live cattle and their products. In addition, this situation contributes a negative impact on the national economic growth through the loss of meat and milk production and poor quality of skin and hides. Serious economic losses can follow outbreaks that have a high morbidity and high mortality rates of 40 percent or more have been encountered. There is no specific antiviral treatment available for LSD-infected cattle. The disease is now the problem of almost all the regions and agro ecological zones of Ethiopia. Major outbreaks of LSD have been occurred in different regions of Ethiopia. Two vaccines, however, Neethling and Kenya sheep and goat pox virus, have been used widely in Africa with success. Preventing movement the diseased animals along with vector control, regular annual vaccinations and awareness creation for cattle owners play great role in disease prevention and control. The disease outbreak was observed in the cattle regardless of previous vaccination with Kenyan sheep- and goat pox vaccine the occurrence of LSD outbreak scale, despite the use of a vaccination regime, is suggestive of vaccine failure. Apparent emerging vaccine failure is a serious problem for efficient control of LSD, as the disease has been manifested by high morbidity and mortality rates, regardless of vaccination status. Consequently continuous surveillance on the status of the disease and genetic information on circulating field viruses is mandatory in order to take effective measures for the control of the disease in the country.
Keywords
• Cattle
• Economic Impact
• Ethiopia
• Lumpy Skin Disease
• Prevention and Control
CITATION
Kassa ST (2023) Review on the Economic Impacts of Lumpy Skin Disease of Cattle and Its Prevention and Control Strategies in Ethiopia. J Vet Med Res 10(6): 1260.
INTRODUCTION
Ethiopia is believed to have the largest livestock population in Africa and livestock production constitutes a vital part of the agricultural system and it accounts about 40% of the agricultural gross domestic product (GDP) [1]. In Ethiopia, the livestock sector has been contributing considerable portion to the country’s economy, and still promising to bring together the economic development of the country. In relation to this, 85% of country’s population economy depends on farming and animal husbandry that rely on this population [2]. However, livestock diseases in the country pose a huge problem on fundamental sector that plays a crucial role to lift the country from poverty. Lumpy skin disease (LSD) is one of the most common viral diseases mentioned in hampering livestock production and productivity with its higher morbidity rate [3,4].
The disease is now the problem of almost all the regions and agro ecological zones of Ethiopia. Major outbreaks of LSD have been occurred in different regions of Ethiopia like Amhara and west Oromia Regions in 2000/2001, Oromia and Southern nation’s nationalities and people (SNNP) regions in 2003/2004 and Tigray, Amhara and Benishangul regions in 2006/2007. LSD is an OIE listed disease because of considerable financial losses and in Ethiopia due to the endemic nature of LSD; the country is facing serious difficulties in exporting live cattle and their products. In addition, this situation contributes a negative impact on the national economic growth through the loss of meat and milk production and poor quality of skin and hides [5]. The disease outbreak was observed in the cattle regardless of previous vaccination with Kenyan sheep- and goat pox vaccine the occurrence of LSD outbreak scale, despite the use of a vaccination regime, is suggestive of vaccine failure. Apparent emerging vaccine failure is a serious problem for efficient control of LSD, as the disease has been manifested by high morbidity and mortality rates, regardless of vaccination status. Consequently continuous surveillance on the status of the disease and genetic information on circulating field viruses is mandatory in order to take effective measures for the control disease in the country [6].
Control and prevention of LSD in endemic countries like Ethiopia is mainly by vaccination. In Africa and the Middle East countries several live attenuated CaPV vaccine strains are currently used for cattle and small ruminants. These include LSDV Neethling strain, Kenyan sheep and goat pox virus (KSGPV) O-240 and O-180 strains, Yugoslavian RM65 SPP strain, Romanian SPP and Gorgan GTP strains [7]. In Ethiopia there are problems related to lack of vaccine efficacy and continuous outbreaks in vaccinated animals [8].
Immunization of the susceptible animals is the effective methods to control the disease. The most commonly used live LSDV vaccines are derived either from the South-African LSDV Neethling strain or an attenuated LSDV field strain and are manufactured in South Africa [9]. In Ethiopia vaccine against LSD has been producing at the National Veterinary Institute (NVI), Bishoftu. The attenuated SPPV Kenya O-180 vaccine strain (referred to as KS-1) of Kenyan origin is used for the production of capripoxvirus vaccine, for small ruminants and cattle, by the NVI.
Ethiopia has been striving to control LSD using mass vaccination at a specified season as well as following a report of the case. Most research finding also characterise LSD virus following an outbreak. Yet few have checked for immune response of cattle after vaccination aiming mainly on different capripox vaccine comparison. Even the reported one mostly focused on stationed farm of crossbred cattle [10]. Additionally, different report has been coming out from animals’ owner and in LSD outbreak areas of Ethiopia about a suspected vaccine failure [2,11].
HISTORY OF LSD
The first description of the clinical signs of LSD was reported in 1929 in Zambia [12]. Same clinical signs were occurred in Botswana, Zimbabwe and the Republic of South Africa between 1943 and 1945, where the infectious nature of the disease was recognized in these outbreaks. In 1949 South Africa, LSD occurred as a panzootic, which affected eight million cattle. In1957, LSD was identified in East Africa in Kenya. In 1972, the disease was reported in Sudan and West Africa in 1974. Nowadays, LSD occurs in most of African continent [3]. In the Middle East, the outbreaks of the LSD were reported in Oman in 1984 and 2009 [13,14]. Kuwait in 1986 and 1991, Egypt in 1988 and 2006, Israel in 1989 and 2006, Bahrain in 1993 and 2002-2003, Yemen, United Arab Emirates in 2000 and the West Bank also reported LSD invasion [13,15]. LSD is exotic to the European Union (EU), but incursions of LSD have occurred in EU neighboring areas [16].
Initially, it was considered to be the result either of poisoning or a hypersensitivity to insect bites. Between 1943 and 1945, cases occurred in Botswana (Bechuanaland), Zimbabwe (Southern Rhodesia) and the Republic of South Africa. The infectious nature of the disease was recognized at this time. Until 1988 LSD was confined to sub-Saharan Africa, but then spread into Egypt. There have been only two laboratory-confirmed outbreaks of LSD outside Africa: in Israel in 1989, which was eliminated by slaughter of all infected and in-contact cattle, and vaccination and in Bahrain in 1993. There was an outbreak in 2000 in cattle imported into Mauritius; the diagnosis was confirmed by electron microscopy. And more recent outbreaks of LSD outside Africa have been reported in Israel (2006 and 2007), Palestine (2007 and 2008) and Bahrain (2006-2009) [17].
ETIOLOGY
LSD virus (LSDV) belongs to the family Poxviridae that is divided into two subfamilies, poxviruses affecting insects (Entomopoxvirinae) and vertebrates (Chordopoxvirinae). CaPVs represent one of eight genera within the Chordopox virus (ChPV) subfamily. The capripox virus genus consists of Lumpy skin Disease Virus, as well as sheeppox virus, and goatpox virus. The prototype of LSDV, Neethling strain, was isolated in South Africa. CaPV infections are usually host specific within specific geographic distributions even though they are serologically indistinguishable from one another [18].
LSDV as a member of CaPVs, it has a single serotype, do not cause persistent infection, have a limited host range and vaccines are available that may provide long term immunity. These attributes increase the prospect of successfully implementing regional control programs, leading to the elimination of the virus and conceivably global eradication. Control and prevention of LSD in endemic countries like Ethiopia is mainly by vaccination. In Africa and the Middle East countries several live attenuated CaPV vaccine strains are currently used for cattle and small ruminants. These include LSDV Neethling strain, Kenyan sheep and goat pox virus (KSGPV) O-240 and O-180 strains, Yugoslavian RM65 SPP strain, Romanian SPP and Gorgan GTP strains [7,19]. In Ethiopia there are problems related to lack of vaccine efficacy and continuous outbreaks in vaccinated animals [8].
EPIDEMIOLOGY OF LSD
Geographic distribution
Until the 1980s, LSD was only found south of the Sahara desert and in Madagascar, but in 1988, it spread into Egypt. It also occurs in other Middle Eastern countries. In 1989, an outbreak in Israel was eradicated by slaughter and vaccination and more recent outbreaks of LSD outside Africa have been reported in Israel (2006 and 2007), Palestine (2007 and 2008) and Bahrain (2006-2009). Some field outbreaks are associated with severe and generalized infections and a high mortality, while with others there are few obviously affected animals and no deaths but in general outbreaks are more severe with the initial introduction of the infection to a region and then abate, probably associated with the development of widespread immunity [17].
Lumpy skin disease (LSD) was first seen in Zambia in 1929, spreading into Botswana by 1943, and then into South Africa, where it affected over eight million cattle causing major economic loss. In1957, it entered Kenya, associated with an outbreak of sheep pox. In1970, LSD spread north into the Sudan; by 1974 it had spread west as far as Nigeria, and in 1977 was reported from Mauritania, Mali, Ghana and Liberia. Another epizootic of LSD between 1981 and 1986 affected Tanzania, Kenya, Zimbabwe, Somalia and the Cameroon, with reported mortality rates in affected cattle of 20%. The occurrence of LSD north of the Sahara desert and outside the African continent was confirmed for the first time in Egypt and Israel between1988 and 1989, and was reported again in 2006 [20]. In the past decade, LSD occurrences have been reported in the Middle Eastern, European and west Asian regions. Lumpy skin disease outbreaks tend to be sporadic, depending upon animal movements, immune status, and wind and rainfall patterns affecting vector populations. The principal method of transmission is thought to be mechanical by arthropod vector [21].
Occurrence of the disease
LSD is an endemic disease of most African countries particularly in those of the sub Saharan region. After 2012 it has spread rapidly through the Middle East, south-east Europe, the Balkans, Caucasus, Russia and Kazakhstan [22,23]. Mostly, field outbreaks can be severe and generalized infection with high morbidity and mortality rates, while in others there may be few affected animals and few or no deaths recorded but in general outbreaks are more severe with the initial introduction of the infection to a region and then will decrease, probably associated with the development of widespread immunity. Morbidity rates reach 80% during epizootics, but are nearer 20% in endemic areas [24].
Hosts and susceptibility
Domestic cattle and Asian water buffalo are the animals affected by LSDV naturally during field outbreaks [25,26]. Some strains may replicate in sheep and goats but to date no epidemiological studies have evidenced small ruminants as reservoirs for the virus [27].Very little is known about the susceptibility of wild ruminants to LSDV. The susceptibility of host animals mostly depends on immune status, age and breed rather than the virulence of the virus. European cattle breeds are generally more susceptible than indigenous African and Asian breeds [14].
Sources of the virus
Lumpy skin diseases virus is present in cutaneous lesions and crusts. Virus is also present in blood, nasal and lachrymal secretions, milk, semen and saliva, which may be sources for transmission. All secretions contain LSD virus when nodules on the mucous membranes of the eyes, nose, mouth, rectum udder and genitalia ulcerate. Shedding in semen may be prolonged since viral DNA has been found in the semen of some bulls for at least 5 months after infection. Approximately 50% of infected animals are likely to show clinical signs; the majority of experimentally infected animals become viraemic and source of the virus. In experimentally infected cattle LSD virus was demonstrated in saliva for 11 days, semen for 22 days and in skin nodules for 33 days, but not in urine or faces [3].
Transmission
Different types of biting and blood feeding arthropods (including mosquitoes and other flies such astabanids, Culicoides, biting midges and Glossinaspecies) are likely responsible for the mechanical spread of the LSD virus [28]. Disease incidence is highest in wet/warm weather. Incidence decreases during the dry season, which is possibly linked to decreases in insect vector occurrence/numbers. Minor sources of infection could include direct and indirect contact (e.g. through infective-saliva contaminated feed and water). Pox viruses are highly resistant and can remain viable in infected tissue for more than 120 days or probably longer time. The virus is also found in blood, nasal discharge, lachrymal secretion, semen and saliva, which considered as main sources for LSD transmission [29]. Other potential transmission routes include the milk of lactating cows and the semen of infected bulls, since the LSD virus can persist for extended periods of time in both [30].
CLINICAL SIGNS OF LSD
The actual incubation period of LSD under field conditions has not been reported, but following experimental inoculation of the virus is 6–9 days until the onset of fever. LSDV replicates inside the host cells such as macrophages, fibroblasts, pericytes and endothelial cells in the lymphatics and blood vessels walls leads to vasculitis and lymphangitis, in severe cases thrombosis and infarction may also develop [9]. In the acutely infected animal, there is initial pyrexia, which may exceed 41°C and can persist for 1 week. The superficial lymph nodes become enlarged and lesions may develop over the body, particularly on the head, neck, udder, scrotum, vulva and perineum between 7 and 19 days and the first ones usually appearing in the perineum. In lactating cattle there is a marked reduction in milk yield [22].
In experimental studies, the intravenous route develops severe generalized infection, while in the intradermal inoculation only 40-50% of animals may develop localized lesions or no apparent disease at all. A localized swelling at the site of inoculation after four to seven days and enlargement of the regional lymph nodes, develop after subcutaneous or intradermal inoculation of cattle with LSDV [9,31] (Figure 1).
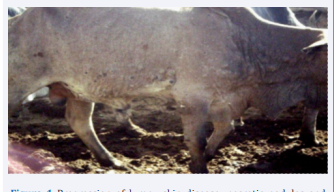
Figure 1: Progression of lumpy skin disease; necrotic nodules and formation of deep scab
Lesions of LSD are round and firm, 1 to 4 cm in diameter, and are flattened and the hair on them stands on end. They vary in number from a few to hundreds; they are intradermal and, mostly confined to the skin area. Lacrimation, nasal discharge, salivation, and lameness can also be observed in association with the pyrexia. Lesions in the nostrils and on the turbinates, causing mucopurulent nasal discharge, respiratory obstruction and snoring; plaques and ulcers in the mouth causing salivation, nodules on the conjunctiva, causing severe lacrimation can be observed in severe cases. Lymph nodes draining the affected area become enlarged and cause local edema [24,32].
DIAGNOSIS OF LSD
Diagnosis of CaPV is based upon clinical signs with laboratory confirmation by virus isolation, polymerase chain reaction (PCR) and electron microscopy. Field diagnosis of LSD is often based on characteristic clinical signs of the disease. However, mild and subclinical forms require rapid and reliable laboratory testing to confirm diagnosis [33,34]. Isolation of virus can be made from collected biopsy or at post-mortem from skin nodules, lung lesions or lymph nodes within the first week of the occurrence of clinical signs, before the development of neutralizing antibodies [35].
Laboratory diagnosis of LSD comprised either identification of the virus using: electron microscopy, egg inoculation, isolation in cell cultures, fluorescent antibody test; or detection of its specific antibody using serological tests. Several polymerase chain reaction (PCR) assays have been developed for more accurate and rapid detection of LSDV in suitable specimens [36]. PCR for the diagnosis of LSD is with a greater sensitivity and good specificity and it is most appropriate technique [37].
Samples submitted for laboratory diagnosis of LSD includes; take biopsy specimen at least two early lesions (for viral isolation), clipped and cleansed with a none-disinfectant soap; if a punch biopsy is used, specimens must be collected at the lesions edge. An enlarged LN can be aspirated aseptically with a syringe and 16- gage needle or a biopsy can be taken. Organ samples should be sealed in screw-caped vials and taped shut. Tissue specimens should include all organs with emphasis on those showing lesions i.e., skin turbinate?s, trachea, lung and lymph nodes. specimens should arriving to laboratory within 24 hours ship with wet ice; if more than one day shipment is required dry ice should be used [38].
Generally, LSDV diagnostic tests can be grouped into 3 categories (1) direct detection, (2) indirect examination (virus isolation), and (3) serology. In direct examination, the clinical specimen is examined directly for the presence of virus particles, virus antigen or viral nucleic acids. In indirect examination, the specimen into cell culture, eggs or animals in an attempt to grow the virus: this is called virus isolation. Serology actually constitute far the bulk of the work of any virology laboratory to demonstrate the presence antibody against the virus infection [39].
The polymerase chain reaction (PCR) is a scientific technique in molecular biology to amplify a single or a few copies of a piece of DNA across several orders of magnitude, generating thousands to millions of copies of a particular DNA sequence.
The conventional gel-based PCR method is a simple, fast and sensitive method for the detection of capripoxvirus genome. In EDTA blood, biopsy, semen or tissue culture samples. However, it does not allow differentiation between LSD and sheep and goat pox viruses. Primers for the viral attachment protein gene and the viral fusion protein gene are specific for all the strains within the genus Capripoxvirus. By the use of sequence and phylogenetic analysis; strains of virus can be identified [40].
STATUS OF LUMPY SKIN DISEASE IN ETHIOPIA
LSD was first reported in 1983 in the northwestern part of the country near Lake Tana [41]. There were frequent outbreak reports of LSD in the county that are highly associated with seasonal peak of mechanical vectors in wet and warm weather conditions [42].The disease has spread to almost all regions and agro-ecological zones of the country. Because of the wide distribution of the disease and the size and structure of the cattle population in Ethiopia, it is likely that LSD is one of the most economically important livestock diseases in the country. One of the recent outbreaks of LSD was occurred in central Ethiopia in 2007 to 2011. These outbreaks were described as active. It was investigated in four districts: Adama, Wenji, Mojo and Welenchiti. The totally 1,675 outbreaks were reported over 5 years period from 2007 to 2011, with 62,176 cases and 4,372 deaths. The Oromia represented the highest numbers of outbreaks (1,066), followed by Amhara (365) and the Southern Nations, Nationalities and People’s Region (123). The 2010 were reported the highest number of outbreaks that were frequently seen between September and December. The morbidity and mortality rates were 13.61% (296) and 4.97% respectively [2].
In Ethiopia LSD is the one of the most economically important livestock diseases. After the first occurrence in 1983 it has spread widely throughout the country and now it is the problem of almost all the regions and agro ecological zones [43,41]. Its spread was mainly enhanced by cattle movements, communal grazing and watering, and pastoralist ways of life [38,44].
In Ethiopia from 2007-2011 totals of 1352 disease outbreaks of LSD have been reported and highest frequency was documented in Oromia region and the least in Afar region [45]. Another study also showed that a total 3811 LSD outbreaks reported in Ethiopia between 2000 and 2015. Most of these outbreaks were from Oromia (54.5%), Amhara (27.9%), SNNP (10.1%) and Tigray regional states (3.6%) No out breaks were reported from Harari and Dire dawa. It also shows that LSD affects districts for one or two years and then spreads to other nearby areas with a susceptible cattle population with a trend of LSD outbreaks increased over time [46].
Since the country has no well-designed control strategy for this disease it is continuing to be a great problem. Even if the animal health authorities undertake vaccination campaigns when outbreak is reported, researches have shown that the different vaccines used in Ethiopia are not fully effective [47]. There have been repeated concerns reported to NVI on the insufficient protection provided by the vaccine, for cattle against LSDV. In addition to this, lack of genetic information on the circulating isolates in the field and their relation to the vaccine strain in use, which is essential for better vaccine matching, is also a great problem in the country [5].
ECONOMIC IMPACT OF LSD IN ETHIOPIA
LSD is an economically important disease of cattle, serious economic losses from outbreaks that have a high morbidity and can produce a chronic debility in infected cattle. LSD is usually considered economically important diseases due to its impact on livestock productivity. This is usually related with the prolonged effect on productivity of dairy and beef cattle through decreased body weight, mastitis, infertility (can be temporary or permanent) and abortion. Additionally, the lesions on animal skin can bring a permanent damage to the hides which affect the leather. There is a great loss of milk production since the disease is more severe in cows in the peak of lactation and causes a sharp drop in milk yield because of high fever caused by the viral infection itself and secondary bacterial mastitis predisposed by the development of lesions on the teats [48,24].
The office international des epizootics consider LSD as list A?? disease that has the potential for rapid spread with ability to cause serious economic loss. Morbidity and mortality of the disease vary considerably depending on the breed of cattle, the immunological status of the population and insect vectors involved in the transmission. Morbidity rates generally varying between 1% and 20%. In a few outbreaks it was reported to be more than 50% although the mortality rates are usually less than 10%. Cows in 1% to 7% of cases may abort. LSD causes severe economic losses due to permanent damage to hides, a prolonged debilitating clinical course, reduced weight gain, temporary or permanent loss of milk production, temporary or permanent infertility or even sterility in bulls, and abortion of pregnant cows [24,39].
Even though the mortality rates of LSD are usually low, it is an economically important disease of cattle in Africa because of the prolonged loss of productivity of dairy and beef cattle, use of the animals for traction, decrease in body weight, mastitis, severe orchitis, which may result in temporary infertility and sometimes permanent sterility [48,22,49]. A study done in Ethiopia has shown that the annual financial cost calculated as the sum of the average production losses due to morbidity and mortality arising from milk loss, beef loss, traction power loss, and treatment and vaccination costs at the herd level was estimated to be USD 6.43 (5.12–8) per head for local zebu and USD 58 (42–73) per head for HF/crossbred cattle [49]. Another study also showed that the average cost of a single ox dying from LSD was calculated as 9,000 Ethiopian birr (ETB), equivalent to US$477.7 (USD1 =18.84 ETB) [2].
In addition to quality degradation of skin and hides skin LSD induces associated economic losses due to reduction of wool quality, meat, losses as a result of culling and mortalities and related with cost of treatment and prevention of the diseases. Even though there are no specific antiviral treatments for LSD- infected cattle, there will be treatment cost for secondary bacterial infection. Treatment cost represents the expenses incurred by farmers for medication at the local public veterinary clinics when farmers bring their clinically sick animals for treatment [49]. Emaciation and a long convalescence period can also significantly decrease the growth rate in beef cattle [21].
LSD have been identified as one of the major impediments for genetic improvement of cattle populations and, consequently, for the development of intensive production units in Africa. It is well known that high producing dairy cattle, such as Holstein- Friesian (HF) and Jersey are more susceptible to CaPV infection than indigenous African and Asian cattle breeds [51,38]. The susceptibility of European cattle breeds and challenges facing dairy-genetics improvement in LSDV-endemic settings in Ethiopia was recently highlighted [49]. Currently live cattle export from Ethiopia is largely feedlot based. The introductions of LSD into feedlots certainly affect access to specific markets. For longer time, Middle East markets are the traditional destination of Ethiopian live bulls. However, the current health status of Borena bulls in market chain unquestionably becomes a challenge for the country’s future live cattle export opportunities to those countries [52]. Costly control and eradication measures such as vaccination campaigns as well as the indirect costs because of the compulsory limitations in animal movements also cause significant financial losses on national level [38,49,50].
In Ethiopia, the financial cost in infected herds was estimated to be USD 6.43 (5.12–8) per head for local zebu and USD 58 (42– 73) per head for HF/crossbred cattle. This economic loss was the sum of the average production losses from morbidity and mortality rate. This can be observed through milk loss, beef loss, traction power loss, treatment, and vaccination costs. However, effective vaccination against LSD can reduce the expenses by 17% per head in local zebu herds and 31% per head in Holstein Friesians/crossbred herds [49]. The other observation in to direct economic losses from animal death and treatment cost was estimated to be 9,000 Ethiopian birr (ETB), (US$477.7) and 16.50 ETB per animal, respectively [2]. Further study conducted by Abebe et al. [54], indicated the existence of significant economic losses. In this cases, largest components of the loss at herd level was from mortality (1000 USD) accompanied by milk loss (120 USD) while control costs were the least losses recorded at herd level.
PREVENTION AND CONTROL
Successful control and eradication of LSD relies on early detection of the index case, followed by a rapid and widespread vaccination campaign. Immunity acquired from natural infection of the disease might be lifelong and vaccination has been successfully used. LSD could be kept under control by vaccination of cattle every year [54]. Live, attenuated vaccines against LSD are commercially available. These have antigenic homology and there is cross protection among them. Local strain of Kenyan sheep and goat pox virus has been shown to effectively immunize sheep, goats and cattle against infection with capripoxvirus with a remarkable success. The next one is attenuated South African LSD virus (Neethling strain) vaccine derived from cattle, freeze dried product is also available. In countries where LSD is endemic, vaccination against this infection was successfully used by vaccinating animals every year. The efficacy of total stamping-out (killing all clinically affected cattle and unaffected herd-mates) and partial stamping-out (killing only clinically affected cattle) policies have been compared using mathematical modelling. The study found that total stamping-out and partial stamping-out resulted in a similar probability of eradicating the infection. The study also highlighted the importance of initiating vaccination campaigns ahead of virus entry [22].
The most likely way for LSD to enter a new area is by introduction of infected animals. Biting insects that have fed on infected cattle may travel and be blown for substantial distances. The movement of contaminated hides represents another potential means for this resistant virus to move. For countries free of the disease, the introduction of the disease can be prevented by restriction of the importation of the animals and their products but in those nations which experience the infection can limit the spread of the lumpy skin disease by restriction of the animal movement from one place to another, quarantine, keeping of sick animals well apart from the rest of the herd and must not share drinking or feeding troughs by making awareness creation of the farmers [54].
Vaccination is the only effective method to control the disease in endemic countries like Ethiopia. The experience in the major parts of the country showed that the vaccination approach is commonly chosen and is often that of ring vaccination around a local foci outbreak when it occurs. Animals that recover from virulent LSD infection generate lifelong immunity consisting both of a humoral and cell mediated protective immunity. Maternal immunity provides protection from LSD in calves at least for 6 months. In previously LSD-free countries, in the event of an outbreak, the rapid confirmation of a clinical diagnosis is essential so that eradication measures, such as quarantine, slaughter-out of affected and in-contact animals, proper disposal of carcasses, cleaning and disinfection of the premises and insect control and ring vaccinations can be implemented as soon as possible [55,24].
Live attenuated vaccines of different capripoxvirus strain origins are available to protect cattle, sheep and goats. Four live attenuated strains of capripoxvirus have been used as vaccines specifically for the control of LSD [20,56]. A strain of Kenyan sheep and goat pox virus passaged 18 times in LT or fetal calf muscle cells, Yugoslavian RM 65 sheep pox strain, Romanian sheep pox strain and lumpy skin disease virus strain from South Africa, passaged 60 times in lamb kidney cells and 20 times on the chorioallantoic membrane of embryonated chicken eggs. It is likely that many of these vaccine strains available in different parts of the world would be suitable for the prophylaxis of LSD. These live attenuated vaccines are mainly stimulating the cell mediated immune response [56].
The OIE Terrestrial Animal Health Code Chapter 11.11, (2017) on lumpy skin disease (caused by group III virus, type Neethling), establishes the international standards on disease control and safe international trade. Each country has its own national legislation applied to LSD. In Ethiopia Kenyan SGPV strain, Romanian sheep pox strain and South African Neethling vaccinal strains were used for production of LSD vaccine at the National Veterinary Institute (NVI). But in the current time only the vaccine that produced from Kenyan SGPV strain is widely used for vaccination of all cattle, sheep and goats populations in the country. Outbreaks can also be controlled by strict quarantines to avoid introduction of infected animals into safe herds, isolation and prohibition of animal movements, slaughtering of all sick and infected animals (Depopulation of infected and exposed animals), proper disposal of carcasses (Incineration), cleaning and disinfection of the premises and insect control [48,38].
For lumpy skin disease, control measures with the exception of vaccination are usually not effective. Vaccination will greatly reduce the morbidity and epizootics but may not completely limit the extension. In endemic countries, vaccination is considered the only economically feasible way to control the spread of LSD and improve cattle productivity [22,48]. Numerous live attenuated vaccines have been developed and used worldwide while inactivated vaccines are considered less effective [57]. In addition, live attenuated vaccines are currently available which are cheap and provide good protection if sufficient herd immunity (over 80%) is maintained by carrying out annual vaccinations [21].
Livevaccinescanhelp to control losses from lumpy skindisease in endemic areas. Four live attenuated strains of CaPVs have been used as vaccines specifically for the control of LSD [22,58]. These are: a strain of Kenyan sheep and goat pox virus, Yugoslavian RM 65 sheep pox strain, Romanian sheep pox strain and lumpy skin disease virus strain from South Africa [26]. In endemic regions vaccine failure is a great problem for the effective control of LSD [7]. It was also reported that CaPV vaccine strains produce a large local reaction at the site of inoculation in Bos taurus breeds which some stock owners find unacceptable. This has discouraged the use of vaccine, even though the consequences of an outbreak of LSD are usually more severe [22].
Immunity in cattle against lumpy skin disease
During the occurrence of infection with capripox virus including lumpy skin disease (LSD) virus; cell-mediated immune response plays a central role of protection though humoral immunity also play its own part. In cell-mediated immune response, different cells including lymphocytes appeared to be increased in their number to destroy the virus. Accordingly, Ahmed et al. [59], found out the increased lymphocyte proliferation in the presence of LSD antigen. Furthermore, Abdelwahab et al. [60], reported increment in lymphocyte in vaccinated cattle.
Cytokine, more specifically gamma interferon (IFN-γ) plays an important role in the defense mechanism from viral and microbial pathogens. It acts by the activation of the pathways that can directly inhibit virus [61,62]. In the finding of Charles et al. [63], IFN-γ was reported its detection until seven days post- vaccination. Additionally, this same study detected serum IFN-γ, IL-12 and other pro inflammatory cytokines except IFN-α. Viral spread from cell-to-cell usually occurs and countered by effector cells of cell mediated immune response. Accordingly, natural killer cells or cytotoxic T lymphocytes are responsible to prevent viral replication and spread by identifying and eliminating infected cells [64]. Furthermore, humoral immune response plays its own role orchestrating itself with cellular immunity for the complete protection. For example, a study on orthopox viruses showed the joint action of cellular and humoral immune response in the elimination of infection. Humoral immune response can stand and considered enough for the future re-infection [65].
LSD Vaccine types and vaccination in Ethiopia
Vaccines developed against LSD have different types including ‘live’ attenuated and inactivated vaccines. Comparatively, the inactivated one are considered to be less effective [57]. However, ‘live’ attenuated vaccines are relatively effective, cheap and available with recorded herd immunity (over 80%) through annual vaccination [65]. There are four CaPVs strains of ‘live’ vaccines namely Yugoslavian RM 65 sheep pox strain, Kenyan sheep and goat pox (KSGP) virus, Romanian sheep pox strain and LSDV strain from South Africa, used to control the spread of LSD [22]. Regardless of its availability and suggested efficacy, vaccine failure is reported in different areas that pose its effect on the effective control of LSD [7]. Even in effective vaccination outcome, the existence of large local reaction at injection site was reported as a side effect. The skin reaction sometimes can affect the cattle owners’ attitude and discourage the use of vaccine though the loss to the production and productivity from the disease outbreak is enormous [22].
In general control and prevention methods include vaccination, animal control movement and slaughter of affected and in contact animals. However, some of these methods are not affordable practices especially in developing countries. Vaccination is considered to be a realistic approach to control the disease in endemic regions and considered cost-effective compared to the abovementioned one [3]. LSD as endemic disease to Ethiopia is approached with annual vaccination scheme and following an outbreak [11]. Kenyan sheep and goat pox (KSGP) virus is a vaccine produced by Ethiopian National Veterinary Institute (NVI) and available when needed with affordable price [66]. However, there have been repeated complaints towards vaccine effectiveness due to the occurrence of outbreak in vaccinated cattle population [11].
CONCLUSION AND RECOMMENDATIONS
LSD is an important disease in cattle causing considerable economic loses. LSD is economically very important disease due to its large scale financial impact by downgrading skins, decreasing milk production, adding treatment costs, reduction in traction powers of oxen and death of the animals. LSD Causes considerable economic losses due to emaciation, damage to hides, infertility and, loss of milk production. Skin lesions result in severe and permanent damage to hides, while lesions in the mouth, pharynx and respiratory tract cause a rapid deterioration in condition and sometimes severe emaciation, which may persist for months. In Ethiopia, the disease is continuing to appear every year. Many studies found that the disease is highly prevalent in central Ethiopia. Regular and timely vaccination strategy is the best choice available for effective control of the disease accompanied with early detection of the disease. Successful control and eradication of LSD relies on early detection of the index case, followed by a rapid and widespread vaccination campaign. Immunity acquired from natural infection of the disease might be lifelong and vaccination has been successfully used. LSD could be kept under control by vaccination of cattle every year. Live, attenuated vaccines against LSD are commercially available. However, different disease outbreaks in vaccinated cattle raise a question on vaccine efficacy that needs a huge attention to look in to it. With this conclusive remark, the following points are recommended to enhance disease prevention and controlling strategies:
-
- Disease prevention and control measures such as vaccination, Vector control and animal movement restriction must be regularly applied in LSD endemic areas
- Further field challenge with circulating field strains should be undertaken on vaccinated cattle to understand the vaccine protection against the disease
- Extended period of follow up for post-vaccination should be exhausted to look when to fall down in the number of cattle with protective antibody
- Further assessment of the vaccine should be performed during transportation, storage and period of protection and time of vaccination.
- Strategic policies for effective control and eradication of the disease should be established
- Develop and implement quarantine system before new animals are introduced to the herd. Importation of livestock and their products should be prohibited from countries with LSD.
REFERENCES
- CSA (Central Statistic Authority): Federal Democratic Republic of Ethiopia Central Statistical Agency. Agricultural Sample Survey report on livestock and livestock characteristics. Volume II. Addis Ababa. 2017.
- Ayelet G, Haftu R, Jemberie S, Belay A, Gelaye E, Sibhat B, et al. Lumpy skin disease in cattle in central Ethiopia: outbreak investigation and isolation and molecular detection of the virus. Rev Sci Tech. 2014; 33: 877-887.
- Tuppurainen ESM, Oura CAL. Review: Lumpy skin disease: An emerging threat to Europe, Middle East and Asia. Transbound Emerg Dis. 2012; 59: 40-48.
- Molla W, Frankena K, Gari G, Kidane M, Shegu D, Jong MCM. Sero-prevalence and risk factors of lumpy skin disease in Ethiopia. Prev Vet Med. 2018; 160: 99-104.
- Gelaye E, Belay A, Ayelet G, Jenberie S, Yami M, Loitsch A, et al. Capripox disease in Ethiopia: Genetic differences between field isolates and vaccine strain, and implications for vaccination failure. Antiviral Res. 2015; 119: 28-35.
- Body M, Singh KP, Hussain MH, Rawahi AA, Maawali AM, Lamki KAet al. Clinico-Histopathological Findings and PCR Based Diagnosis of Lumpy Skin Disease in the Sultanate of Oman. Pak Vet J. 2011; 32: 2, 206-210.
- Gari G, Abie G, Gizew D, Wubete A, Kidane M, Asgedom H, et al. Evaluation of the safety, immunogenicity and efficacy of three Capri poxvirus vaccine strains against lumpy skin disease virus. Vaccine. 2015; 33: 3256-3261.
- Tilahun Z, Berecha B, Simenew K, Reta D. Towards Effective Vaccine Production: A Controlled Field Trial on the Immunological Response of Three Lumpy Skin Disease Vaccine Strains in Dairy Farms. Acad Jour of Anim Dis. 2014.
- Ben GJ, Klement E, Khinich E, Stram Y, Shpigel NY. Comparison of the efficacy of Neethling lumpy skin disease virus and x10RM65 sheep- pox live attenuated vaccines for the prevention of lumpy skin disease- The results of a randomized controlled field study. Vaccine. 2015;33: 4837-4842.
- Zenebe T, Bayisa B, Tilahun Z, Keskis S, Duguma AR, . Towards Effective Vaccine Production: A Controlled Field Trial on the Immunological Response of Three Lumpy Skin Disease Vaccine Strains in Dairy Farms. Acad Jour of Anim Dis. 2014; 3: 17-26.
- Molla W, Frankena K, Gari G, de Jong MCM. Field study on the use of vaccination to control the occurrence of lumpy skin disease in Ethiopian cattle. Prev Vet Med. 2017; 147: 34-41.
- Morris JA. Pseudo-urticaria. Northern Rhodesia Department of Animal Health. Annual Report. 1931; 1930: 12.
- Kumar M. An Outbreak of Lumpy Skin Disease in a Holstein Dairy Herd in Oman: A Clinical Report. Asian J Anim Vet Adv. 2011; 6: 851- 859.
- Tageldin MH, Wallace DB, Gerdes GH, Putterill JF, Greyling RR, Phosiwa MN, et al. Lumpy skin disease of cattle: an emerging problem in the Sultanate of Oman. Trop Anim Health Prod. 2014; 46: 241–246.
- Sherrylin W, Ahmed EI, Raffaele M, Markos T, Felix N, Eran R. Emergence of lumpy skin disease in the Eastern Mediterranean Basin countries. Empress Watch. 2013; 29.
- EFSA Panel on Animal Health and Welfare (AHAW). Scientific Opinion on lumpy skin disease. EFSA Journal. 2015; 13: 3986.
- Body M, Singh P, Hussain H, Al-Rawahi A, Al-Maawali M, Al-Lamki K, et al. Pakistan Veterinary Journal Clinico-Histopathological Findings and PCR Based Diagnosis of Lumpy Skin Disease in the Sultanate of Oman. Pak Vet J. 2012; 32: 2074-7764.
- Tulman ER, Afonso CL, Lu Z, Zsak L, Kutish GF, Rock DL. Genome of lumpy skin disease virus. J Virol. 2001; 75: 7122-7130.
- Babuik S, Bowden TR, Boyle DB, Wallace DB, Kitching RP. Capripox viruses: An Emerging Worldwide Threat to Sheep, Goats and Cattle. Transbound Emerg Dis. 2008; 55: 263-272.
- Brenner J, Haimovitz M, Oron E, Stram Y, Fridgut O, Bumbarov V, et al. Lumpy skin disease (LSD) in a large dairy herd in Israel. Israel Journal of veterinary Medicine. 2006; 61.
- Tuppurainen E, Venter EH, Shisler JL, Gari G, Mekonnen GA, Juleff N, et al. Review: Capri poxvirus Diseases: Current Status and Opportunities for Control. Transbound Emerg Dis. 2015; 64: 729-745.
- OIE. OIE Manual of Diagnostic Tests and Vaccines for Terrestrial Animals. Lumpy skin disease. 2017.
- Coezer J, Tuppurainen E. Lumpy skin disease Oxford University Press.Cape Town, Southern Africa. 2004; 2: 1268-1276.
- Radostits M, Gay C, Hinchcliff W, Constable D. veterinary medicine A text book of the diseases of cattle, horses, sheep, pigs and goats 10th ed. WB Saunders Co., Philadelphia, USA. 2006; 1424-1426.
- El-Nahas EM, El-Habbaa AS, El-Bagoury GF, Radwan MEI. Isolation and identification of lumpy skin disease virus from naturally infected buffaloes at Kaluobia, Egypt. Glob Vet. 2011; 7: 234-237.
- Al-Salihi KA. Lumpy Skin disease: Review of literature. MRVSA. 2014; 3: 6-23.
- Tuppurainen ES. Diagnostic assays for the detection of lumpy skin disease virus and antibodies. 2017.
- Chihota CM, Rennie LF, Kitching RP, Mellor PS. Attempted mechanical transmission of lumpy skin disease virus by biting insects. Med Vet Entomol. 2003; 17: 3: 294-300.
- FAO. Good Emergency Management Practices: The Essentials. Edited by Honhold N, Douglas I, Geering W, Shimshoni A, Lubroth J. FAO Animal Production and Health Manual No. 11. Rome. 2011.
- Irons PC, Tuppurainen ES, EH Venter. Excretion of lumpy skin disease virus in bull semen. Theriogenology. 2005; 63: 1290-1297.
- Abdulqa HY, Rahman HS, Dyary HO, Othman HH. Lumpy Skin Disease. Reproductive Immunology: Open Access. 2016; 1: 25.
- MacLachlan NJ, Dubovi EJ. Fanner’s Veterinary Virology. 4th edition Elsevier. 2011.
- Alaa A, Hatem M, Khaled A. Polymerase chain reaction for rapid diagnosis of a recent lumpy skin disease virus incursion to Egypt. Arab J Biotech. 2008; 11: 293-302.
- Knopvelsiekte N. Identification and diagnosis of lumpy skin disease.J Virology. 2008; 44:1-4.
- CFSPH. The Center for Food Security and Public Health, Iowa State University, College of Veterinary Medicine and Institution of International cooperation in Animal Biologics, an OIE collaborating center. 2008.
- Stram Y, Kuznetzova L, Friedgut O, Gelman B, Yadin H, Rubinstein- Guini M. The use of lumpy skin disease virus genome termini for detection and phylogenetic analysis. J Virol Methods. 2008; 151: 225- 229.
- Kholy AAE, Soliman HMT, Abdelrahman KA. Polymerase chain reaction for rapid diagnosis of a recent lumpy skin disease virus incursion to Egypt, Veterinary Serum & Vaccine Research Institute. Arab Journal of Biotechnology. 2008; 11: 293-302.
- Tuppurainen ES, Oura CA. Review: Lumpy Skin Disease: An Emerging Threat to Europe, the Middle East and Asia. Journal of Transboundary and Emerging Diseases. 2011; 59: 40-48.
- Vorster H, Mapham H. pathology of lumpy skin disease. Livestock Health and Production Review. 2008; 1: 16-21.
- Le Goff C, Lamien E, Fakhfakh E, Chadeyras A, Aba- Adulugba E, Libeau G, et al. Capripoxvirus G-protein-coupled chemokine receptor: a host-range gene suitable for virus animal origin discrimination. J Gen Virol. 2009; 90: 1967-1977.
- Mebratu GY, Kassa B, Fikre Y, Berhanu, B. Observation on the outbreak of lumpy skin disease in Ethiopia. Rev Elev Med Vet Pays Trop. 1984; 37: 395-399.
- Getachew G, Waret-Szkuta A, Grosbois V, Jacquite P. Risk Factors Associated with observed clinical lumpy skin disease in Ethiopia. PhD thesis. 2010; 68-84.
- Gari G, Waret-Szkuta A, Grosbois V, Jacquiet P, Roger F. Risk factors associated with observed clinical lumpy skin disease in Ethiopia. Epidemiol Infect. 2010; 138: 1657-1666.
- Gari G, Grosbois V, Waret-Szkuta A, Babiuk S, Jacquiet P, Roger F. Lumpy skin disease in Ethiopia: seroprevalence study across different agro-climate zones. Acta Trop. 2012; 123: 101-106.
- Gumbe A. Review on lumpy skin disease and its economic impacts in Ethiopia. JDVAR. 2018; 7: 39-46.
- Molla W, De Jong MCM, Frankena K. Temporal and spatial distribution of lumpy skin disease outbreaks in Ethiopia in the period 2000 to 2015. BMC Vet Res. 2017a; 13: 310.
- Molla W, de Jong MCM, Gari G, Frankena K. Economic impact of lumpy skin disease and cost effectiveness of vaccination for the control of outbreaks in Ethiopia. Prev Vet Med. 2017b; 147: 100-107.
- Abera Z, Degefu H, Gari G, Ayana Z. Review on Epidemiology and Economic Importance of Lumpy Skin Disease. International Journal of Basic and Applied Virology. 2015a; 4: 8-12.
- Gari G, Bonnet P, Roger F, Waret-Szkuta AS. Epidemiological aspects and financial impact of lumpy skin disease in Ethiopia. Prev Vet Med. 2011; 102: 274-283.
- Abera Z, Degefu H, Gari G. Assessment of Distribution and Associated Risk Factors of Lumpy Skin Disease in Selected Districts of West Wollega Zone, Western Ethiopia. Acad J Anim Diseases. 2015b; 4: 130-140.
- Bhanuprakash V, Hosamani M, Singh RK. Prospects of control and eradication of capripox from the Indian subcontinent: A perspective. Antiviral Res. 2011; 91: 225-232.
- Alemayehu G, Zewude G, Admassu B. Risk assessments of lumpy skin diseases in Borena bull market chain and its implication for livelihoods and international trade. Trop Anim Health Prod. 2012; 45: 1153-1159.
- Abebe WM, de Jong MCM, Gari G, Frankena K. Economic impact of lumpy skin disease and cost effectiveness of vaccination for the control of outbreaks in Ethiopia. Prev Vet Med. 2017; 147:100-107.
- Thomas L. Lumpy-skin disease, a disease of socioeconomic importance. Journal of Virolology. 2002; 76: 6054-6061.
- Tuppurainen ESM, Venter HE, Coetzer JAW. The detection of lumpy skin disease virus in samples of experimentally infected cattle using different diagnostic techniques. Onderstepoort J Vet Res. 2005; 72:153-164.
- Kitching RP. Vaccines for lumpy skin disease, sheep pox and goat pox. Dev Biol (Basel). 2003; 114: 161-167.
- Boumart Z, Daouam S, Belkourati I, Rafi L, Tuppurainen E, Tadlaoui KO, et al, M.E. Comparative innocuity and efficacy of live and inactivated sheeppox vaccines. BMC Vet Res. 2016; 12: 133.
- Brenner J, Bellaiche M, Gross E, Elad D, Oved Z, Haimovitz M, et al. Appearance of skin lesions in cattle populations vaccinated against lumpy skin disease: statutory challenge. Vaccine. 2009; 27: 1500-1503.
- Ahmed AM, Mukhtar MM, El Hussein A, Tageldin AMN, Fadol MA. Immune response of sheep vaccinated with Capripoxvaccine. Vet Res. 2007; 1: 12-16.
- Abdelwahab MG, Khafagy HA, Moustafa AM, Saad MA. Evaluation of humoral and cell-mediated immunity of lumpy skin disease vaccine prepared from local strain in calves and Its related to maternal immunity. Jour of Amer Sc. 2016; 12: 38-45.
- Strichman R, Samuel CE. The role of gamma interferon in antimicrobial immunity. Curr Opin Microbiol. 2001; 4: 251-259.
- Biron CA, Brossay L. NK cells and NKT cells in innate defense against viral infections. Curr Opin Immunol. 2001; 13: 458-464.
- Charles KN, Marszal P, Zhang Sh, Weingart HM. Innate immune response to rift valley fever virus in goats. PLoS Neg Trop Dis. 2012; 6: 1623.
- Seet BT, Johnston JB, Brunetti CR, Barrett JW, Everett H, Cameron C, et al. Poxviruses and immune evasion. Anu Rev Immunol. 2003; 21: 377-423.
- Tuppurainen ESM, Venter EH, Shisler JL, Gari G, Mekonnen GA, Juleff N, et al. Review: Capripoxvirus Diseases: Current Status and Opportunities for Control. Transbound Emerg Dis. 2017a; 64: 729-745.
- National Veterinary Institute (NVI). User manual for lumpy skin disease vaccine. 2019; 14.







































































































































{kind=link}