Spontaneous Rupture of the Bladder in Postpartum Phase: A Catastrophic Life-Threatening Event
- 1. Depatment of OBG, Lady Hardinge Medical College, India
- 2. Department of Surgery, Lady Hardinge Medical College, India
Abstract
Spontaneous bladder rupture is an extremely rare condition. Patients may present with abdominal distension, fever, hematuria, oliguria, anuria, and deranged KFT. Early diagnosis and prompt management are the key to decreasing morbidity and mortality. Mainstay management for intraperitoneal bladder rupture is surgical repair and rest to the urinary bladder. In this case report we describe a case of spontaneous bladder rupture after a normal vaginal delivery, that presented 10 days after delivery and where, with timely diagnosis and management, the patient’s lfe could be saved.
Keywords
• Vaginal delivery
• Bladder rupture
• Spontaneous
• Anuria
CITATION
Muntaha, Aashita, Pawan, Manju (2023) Spontaneous Rupture of the Bladder in Postpartum Phase: A Catastrophic Life-Threatening Event. Med J Obstet Gynecol 11(4): 1180.
INTRODUCTION
Bladder rupture during labour or postpartum is a very rare condition [1]. Predisposing factors are increased visceral pressure, weakening of the bladder, and vesical catheterization.
Bladder rupture usually presents as ascites and acute abdominal pain; intraperitoneal rupture may lead to peritonitis or sepsis. Other presenting symptoms can be suprapubic pain, anuria, and haematuria.
Diagnosing bladder rupture is difficult, even by means of diagnostic modalities such as CT scans [2]. It is important to have a high index of clinical suspicion. Bladder traumas can be intraperitoneal where urine leaks into the peritoneal space and presents with the symptoms of uraemic ascites.
Surgery is the treatment of choice and consists of urine drainage from the peritoneal cavity and closing of the rupture.
CASE REPORT
In this case report we present a case of a 35-year-old woman P3L3 day 09 of Normal Vaginal Delivery, who presented to the emergency department with the chief complaints of pain abdomen, vomiting, non-passage of urine, and abdominal distension for one week. The patient was discharged after 48 hours of normal vaginal delivery once she passed urine and stools and her hospital stay was uneventful. The patient was apparently asymptomatic up to one week, after that she developed pain in the suprapubic region which was insidious in onset and gradually progressed to involve the whole abdomen, severe in intensity, and relieved only by injectable analgesics. She also had complaints of vomiting, which was nonprojectile, consisted of food particles, non-bilious, non-blood tinged. She gave a history of non-passage of urine and stool for 5 days. There was history of fever, burning micturition, cough, shortness of breath, jaundice, and clay stools. On examination, patient was conscious, alert, oriented to time place, and person, thin-built, and well nourished. Her BP was 130/70 mm Hg and pulse was 120/min, oxygen saturation was well maintained. There was no pallor, icterus, clubbing, cyanosis, LAN, edema. Systemic examination of heart, lungs and CNS was found normal. On abdominal examination, her abdomen was distended, tenderness was present all over, though bowel sounds were present. There was no rigidity and guarding. On digital rectal examination, the lumen was found collapsed, and fecal loading was there. Ultrasound whole abdomen was done, showing collapsed bowel loops, gross free fluid with echoes within the peritoneal cavity; rest of the organs were normal.
Blood investigations showed leukocytosis with a TLC count of 21000, with urea level of 221, and creatinine of 9.0. Ascitic tap was done with the urea of 253 and creatinine of 13.10 similar range of urine. Together the symptomatology and investigation results led us to a provisional diagnosis of bladder rupture with urinary peritonitis following normal vaginal delivery.
The patient was planned for emergency laparotomy after taking informed high-risk consent. Intraoperative 7 liters of urine-smelling fluid drained from the abdominal cavity. There was rent in the bladder at 2 sites one of 1x2 cm and the other 0.5x0.5 cm on the posterior wall of the urinary bladder so the margins were freshened, two-layered closure was done suprapubic catheter and Foley’s catheters were placed and retro vesical drain inserted. Postpartum uterus was bulky and was looking normal.
During the post-operativeperiod, patient was shifted to Surgical ICU and kept on mechanical ventilation, and injectable antibiotics were given. Intensive monitoring was done, patient was extubated on post operative day 2 and thereafter shifted to the ward. The postoperative phase was uneventful, and the patient was discharged on POD 7. The patient was followed postoperatively and was doing fine (Figure 1 and Figure 2).
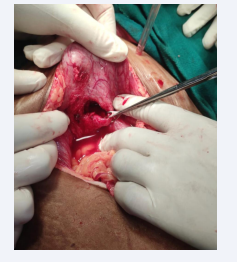
Figure 1: Intraop image showing bladder rent
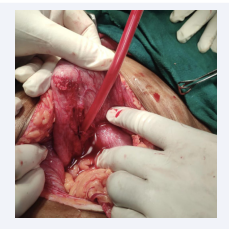
Figure 2: Intra-op image of bladder rent.
DISCUSSION
Ascitis with acute abdomen in the puerperal phase is very rare. Differential diagnosis include bowel perforation, hepatic artery thrombosis, postpartum pancreatitis, and rarely bladder rupture.
An isolated intraperitoneal bladder rupture following vaginal delivery like in the present case is very rare. The term “spontaneous rupture of urinary bladder- SRUB” was coined by Sisk and Wear [3]. Spontaneous rupture of the bladder represents a surgical emergency. Clinical signs and symptoms of bladder rupture are abdominal pain, tenderness, and anuria. Intraperitoneal urine accumulation may cause intestinal and peritoneal irritation [4]. If bladder rupture is suspected, ascitic fluid should be analysed for urea and creatinine.
Bladder rupture can be attributed to previous history of pelvic surgery, bladder diverticula, prolonged second stage and good size baby, which can impinge upon and compress the bladder against pubic symphysis and it can lead to vascular insult resulting into necrosis and then rupture. Spontaneous bladder rupture can be due to bladder disease or sudden increase in the intravesical pressure during second stage of labour or a neuropathic bladder. In our case no such history was there, except first trimester history of a single episode of UTI. In this case bladder rupture appeared to have been caused by a nerve injury which led to overdistension of bladder followed by bladder rupture and the presentation was quite late i.e 2 weeks postpartum, similar to the case of Singla R, Arora A, Bora G, et al. [5].
Kibel et al., in 1995 reported the first case of spontaneous bladder rupture in puerperium [6]. A.Farahzadi et al., reported a case of a nulliparous woman with abdominal pain and distension about 20 days after normal vaginal delivery, there was intraperitoneal rupture of bladder in dome of bladder which was sealed by jejunum [7].
Btissam Ouafidi et al also reported a case of a 34 year old patient who had non traumatic vaginal delivery who presented 7 days later with acute abdomen and anuria. Computed tomography showed free fluid in the peritoneal cavity. An intraperitoneal rupture of the bladder dome was detected, showing extravasation of contrast into the peritoneal cavity. An exploratory laparotomy revealed a perforation on the bladder dome that was sutured [8], similar to our case.
Faranak et al presented a case of 34 year old woman postpartum, who presented with acute abdomen, and there was evidence of renal failure, ultrasonography showed ascites. Her symptoms did not subside after dialysis. She underwent laparotomy, which revealed bladder perforation. Consequently, cystorrhaphy and cystoplasty were done without postoperative complications.
For diagnosis of bladder rupture usually non contrast CT with retrograde cystogram is advised [5]. CT cystogram and cystoscopy is confirmatory. Prompt intervention is very important to reduce the morbidity and mortality once the diagnosis is made. Decision for laparotomy should not be delayed for want of CT scan and other radiological investigations.
CONCLUSION
New onset ascites, oliguria/anuria, deranged KFT in a post- partum patient with uneventful immediate post-partum phase should raise a doubt of bladder rupture. It is a preventable condition. Early diagnosis and surgical treatment is important and reduces the morbidity and mortality in such cases.
REFERENCES
- Stabile G, Cracco F, De Santo D, Zinicola G, Romano F, De Manzini N, et al. Spontaneous Bladder Rupture after Normal Vaginal Delivery: Description of a Rare Complication and Systematic Review of the Literature. Diagnostics (Basel). 2021; 11: 1885.
- Hadian B, Nazarpoor S, Garshasebi M, Zafar Mohtashami A. Missed bladder rupture following vaginal delivery: Possible role of assessing ascitic fluid creatinine levels? Clin Case Rep. 2020; 8: 1247-1250.
- Malani K, Samant PY, Thakur H. Postpartum Urinary Bladder Rupture. JPGO. 2019; 6.
- singla R, Arora A, Bora G. Spontaneous isolated intraperitoneal rupture of urinary bladder after normal vaginal delivery presenting as puerperal sepsis. Int J Pregn and Chi Birth. 2021; 7: 141-143
- Zutshi V. International Journal of Reproduction, Contraception, Obstetrics and GynecologyZutshi V et al. Int J Reprod Contracept Obstet Gynecol. 2019; 8: 3794-3797
- Farahzadi A, Mohammadipour S. A Late Presentation of Spontaneous Bladder Rupture During Labor. Urol Case Rep. 2016; 8: 24-25.
- Ouafidi B, Bouab M, Kiram H, Jalal M, Lamrissi A, Fichtali K, et al. Spontaneous bladder rupture following non traumatic vaginal delivery in a multiparous woman: A rare case report. Int J Surg Case Rep. 2021; 87: 106349
- Faranak Olamaeian, Ali Tayebi, Sara Ghahari. A rare cause of acute abdomen: Spontaneous bladder rupture following normal vaginal delivery. Authorea. 2023.









































































































































{kind=link}