Determinants of Open Defecation and Its Public Health Implications in Todee Health District, Montserrado County, Liberia
- 1. Adjunct Faculty of the CEPRES International University Student (PhD), Frontier University, Somalia
- 2. MRes (Community Health & Primary Care) Student, Frontier University, Somalia
Abstract
Background: Defecating in the Open field has become a common practice in most developing countries. This is a decision that is made by individuals or influenced by the environment.
Objective: The research aims to explore the determinants of open defecation and its implications on public health.
Methodology: The research employed the explanatory Sequential mixed methods design. We conducted a survey using purposive sampling, where we interviewed 51 persons from cross-sections of the District. We used these methods to conduct Key Informant Interviews with knowledgeable individuals about the research topic. The research participants included influential community members and healthcare providers. The interview was later followed by Focus group discussions, during which the district was divided into four strata, with four focus groups held. Each group had 7 participants aged 18 or older. Group one: age range 18-27; Group two: age range 28-37; Group three: age range 38-47; and Group four: age range 48 and above. The participants in the focal group discussion were all females.
Results: 33.33% of the respondents aligned open defecation with female insecurity. Limited sanitary infrastructure and highly entrenched tradition are identified as significant determinants of open defecation, with 41.18% and 39.22% of respondents reporting them, respectively. 47% of respondents prefer involving traditional leaders in reducing waste, while 16 respondents (32.4%) want more public latrines built in various communities.
Recommendation: The reintroduction of the CLTS program and the development of a monitoring and evaluation framework will significantly help achieve and sustain the program, and build a system of intersectoral collaboration involving the traditional leaders in the planning and implementation of community development programs.
Keywords
• Community
• Defecation
• Health
• Sanitation
Citation
Kehnel DW, Lamah SMT (2026) Determinants of Open Defecation and Its Public Health Implications in Todee Health District, Montserrado County, Liberia. Ann Biom Biostat 9(1): 1043.
BACKGROUND
Defecating in the Open field has become a common practice in most developing countries [1]. This is a decision that is made by individuals or influenced by the environment. While open defecation is a human decision, it primarily reflects a lack of sanitation infrastructure and services [2]. One hundred twenty-two million people were practicing open defecation globally in 2015 [3]. More than eight countries have more than 5 million people practising open defecation, including Nigeria, which ranks second in the World with 47 million people practising opendefecation [4]. Open defecation is one of the leading factors of disease-prone environments, including typhoid and diarrhoea [2-5].
Open defecation immensely contributes to stunting in children, which affects their physical and mental development. About 28 million children in the West and central African region are affected by stunting, which is derived from open defecation [6]. According to the World Bank, African countries lose billions of dollars each year due to inadequate sanitation [7].
We cannot argue the facts that open defecation is a significant public health challenge in many underdeveloped and developing countries, including Liberia. An estimated 35% of Liberian citizens practice open defecation [8]. This indicates the high prevalence of open defecation. People in rural settings practice open defecation the most. About 85% of the rural communities are affected by open defecation. At the same time, an estimated 15.6% of the population practices open defecation. Limited sanitary.
METHODOLOGY
The research employed the explanatory Sequential mixed methods design. We conducted a survey using purposive sampling, where we interviewed 51 persons infrastructure and economic disabilities are among the major contributing factors [9].
Todee Health District is one of the remote districts in Montserrado County. Todee district is one of the seven health districts in Montserrado and is remote. The district has nine health facilities, including seven public and two private. The district’s livelihood is centered on farming and coal burning. However, the district is highly entrenched, where acceptance of modernization remains a major challenge. The bushes and open fields are still used as the primary sites for defecation. The research aims to explore the determinants of open defecation and its implications on public health. It is bent on assessing public health outcomes and exploring environmental, cultural, and socio-economic factors. The research is optimistic about comprehensively understanding the factors determining open defecation in the Todee health district. It is also expected to identify significant health risks associated with open defecation, helping decision-makers make informed decisions that will improve the lives of inhabitants. We expect practical interventions that improve sanitation and improve lives from cross-sections of the District. We used these methods to conduct Key Informant Interviews with knowledgeable individuals about the research topic. The research participants included influential individuals, including community and healthcare providers. The interview was later followed by Focus group discussions where the district was divided into four strata, with four focus group discussions held. Each group had seven participants within the age range of 18 to above forty-eight years. Group one age range from 18-27, Group two from 28-37, Group three from 38-47, and Group four from 48 and above. The focal group discussion participants were all females. We decided dealing with a cross-section of females because they are more vulnerable to the effects of open defecation compare to male (Figure 1).
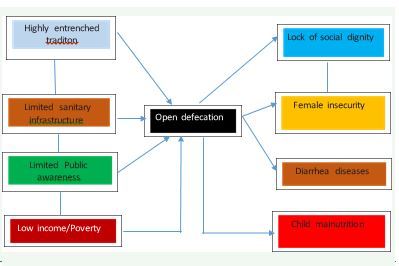
Figure 1 Conceptual Framework.
The qualitative data included cultural beliefs about open defecation and the associated public health implications in the district, while the quantitative data included socio-economic status, sanitation practices, and health outcomes. The data was collected from November 10, 2025 to December 13, 2025.
Ethical considerations
The research was done under the Supervision and approval of the Research and Ethics department of the CEPRES International University (CIU) Liberia.
DISCUSSIONS
Table 1: Demographic Information
|
Age of Respondents |
Frequency |
Percent |
|
18-27 |
16 |
31.37 |
|
28-37 |
13 |
25.49 |
|
38-47 |
12 |
23.53 |
|
48> |
10 |
19.61 |
|
Sex of Respondents |
|
|
|
Male |
21 |
41.18 |
|
Female |
30 |
58.82 |
|
Occupation of the Respondents |
|
|
|
Farmer |
10 |
19.61 |
|
Business persons |
6 |
11.76 |
|
Healthcare Workers |
3 |
5.88 |
|
Teacher |
3 |
5.88 |
|
Motor cyclist |
8 |
15.69 |
|
Security Personnel |
3 |
5.88 |
|
Ordinary community dweller |
10 |
19.61 |
|
Community leaders |
8 |
15.69 |
|
Time lived in the community |
|
|
|
<1 year |
2 |
3.92 |
|
1-3 years |
11 |
21.57 |
|
4-6 years |
17 |
33.33 |
|
7> |
21 |
41.18 |
|
Total |
51 |
100 |
Field data-2025
Table 1 demonstrates the demographic information of the research respondents. The mean age of respondents is 12.75 years; the largest share (31.37%) is in the 18-27 age range. Additionally, 25.49% of the respondents were in the age range of 28-37. The total number of interviews conducted for the quantitative study was 51.582% female and 41.18% male. The interview was conducted with people from different occupations, including farmers, businesspeople, and healthcare providers.
We also interview teachers, motorcyclists, security personnel, and community dwellers. Of the data presented, 19.61% are farmers and ordinary community dwellers, and 15.69% are motorcyclists and community leaders, respectively. We had 21 persons (41.18%) who had lived in the district for more than 7 years, 17 (4-6 years), and 11 (1-3 years), constituting 33.33% and 21.57% respectively.
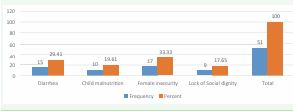
Figure 2 Public Health Implication of Open defecation
Figure 2 denotes the public health implications of open defecation. 17 respondents (33.33%) aligned open defecation with female insecurity, while 15 respondents (29.41%) associated it with diarrhea. 19.61% and 17.65% of the respondents aligned open defecation with lack of social dignity and child malnutrition, respectively. Open defecation reduces the dignity of girls and women, and exposes them to harassment and to the worst-case scenario, rape.
There is less privacy when someone uses the open field for defecation. Anyone could use that way at any given time and might harass you if not on the same page, in the future. In Liberia, mainly in the cultural settings, women feel that as long as a man has seen their exposed body at any time, he can go intimate with them if he wants, because there is nothing to hide anymore. This is a sentimental belief that requires revision. This belief has led most of the adolescents into early sex and marriage, thereby limiting them from reaching their full educational potential. This is a factor increasing the illiteracy rate in the country. These findings correlate with Saleem et al.’s (2019) article “Health and social impacts of open defecation on women.” Open defecation is the promoter of poor health in women with long-term negative effects on their psychosocial well- being [10].
Diarrhea is one of the diseases caused by open defecation. When individuals defecate in the open, their feces are exposed to flies and rodents. Flies sit on the feces and later come into contact with uncovered food and water, contaminating them. When ingested, it causes stomach upset that, in most cases, results in a trip to the hospital. Diarrhea is reported by the WHO as the third leading cause of death in children 1-59 months. It kills around 443,832 children under five years and an additional 50,851 children aged 5 to 9 years worldwide [11]. Diarrhoeal disease Deaths in Liberia reached 1,592 or 4.73% of total deaths. The age-adjusted Death Rate is 47.97 per 100,000 of the population, ranking Liberia #37 in the world [12].
Research has shown that open defecation leads to stunting growth and malnutrition. This is because the microorganisms that travel through the waterways and food make it unwholesome for human consumption. In urban settings, more attention is given to food preparation than in rural settings [13]. When the child continuously consumes unwholesome food and contaminated water, it breaks down the immune system and exposes the child to malnutrition as the body organs will not receive the necessary nutrients required for growth and repairs [14].
Table 2 details the determinants of open defecation. Limited sanitary infrastructure and highly entrenched tradition are seen as the significant determinants of open defecation, constituting 41.18% and 39.22% of the respondents, respectively. Nevertheless, low income is also flagged out as a determinant, as 15.69% aligned it with open defecation. The issue of “free things/services” has become a severe and growing stigma among Liberia’s doorsteps with no attached cost. According to the Water Foundation, “more than one-third of Liberians still practice open defecation, with almost half of the population lacking safe facilities. Todee district was among the first districts whose community achieved open defecation-free status in 2010. The first communities include Sackie, Gbokolleh, and Frank Town, which were previously part of the Caresburg health district.
Table 2: Determinants of Open Defecation.
|
What causes open defecations? |
Frequency |
Percent |
|
Limited sanitary infrastructure |
21 |
41.18 |
|
Highly entrenched tradition |
20 |
39.22 |
|
Limited Public Health awareness |
2 |
3.92 |
|
Low Income/Poverty |
8 |
15.69 |
|
How could we reduce open defection? |
|
|
|
Building more public latrines in the various communities |
16 |
31.4 |
|
Increasing Public health awareness |
5 |
9.8 |
|
Imposing Fines |
6 |
11.8 |
|
Involving the traditional leaders |
24 |
47 |
|
Total |
51 |
100 |
Field data-2025
The community-led Total Sanitation (CLTS) approach was introduced into Liberia’s health system on March 30, 2008, with a focus on transforming hygiene and sanitation behavior, rather than just building toilets. The main idea borrowed from Dr. Kamel Kar, the founder of CLTs, was to have Liberian communities initiate activities to address their sanitation issues through organized community efforts [15].
This approach worked well when a team of Environmental Health Professionals led community activities. The activities began to falter when nurses replaced environmental health professionals with little or no understanding of the approach; as a result, the approach shifted from sanitation and prevention to curative services.
This change has exponentially increased open defecation and made the open defecation-free communities return to open defecation communities. Continuous supervision has been the key to community dwellers building their own latrines. The CLTS program halted the construction of Public latrines, except for Public facilities such as government schools and health centers.
It now requires collaborative effort to further strengthen community initiative programs through the use of trained professionals. As the data indicate a highly entrenched tradition as one of the determinants, this suggests they had to return to their normal culture, as there is no external or driving force.
The typical lifestyle for the inhabitants has been to use the bushes and waterways for defecation. This was practical because most of the activities were centered around farming, where you would not have to leave the farm, which is an hour or two walk to the town for defecation purposes. On the contrary, there are now limited farm activities. People spent most of their time around the commercial towns, which required sanitary facilities that would promote health and prevent diseases.
Table 2 also provides ways to reduce open defecation. Twenty-four respondents, constituting 47% of the respondents, prefer involving the traditional leaders in the reduction, while 16 respondents (32.4%) want the building of more public latrines in various communities. However, six respondents (11.8%) prefer imposing fines, and five respondents (9.8%) prefer increasing health awareness. The district is a traditional and cultural one; they obey the traditional council/leaders more than any other authorities. Hence, involving the conventional leaders has the potential to raise the bar. However, if this must work, it means that the traditional leaders should take the lead in building their own latrines first. If this does not happen, the others will not take it seriously, and there will be no enforcement as expected.
The construction of public latrines in communities is key in the data, but who takes ownership of ensuring they remain sanitary and functional? This was the first approach that did not materialize and became a failed project for NGO and INGOs. The CLTS, when combined with the Participatory Hygiene and Sanitation Transformation (PHAST), has proven to work better over the years as it encourages self-reliance and responsibility. It empowers individuals and communities to take their sanitation into their own hands.
From all indications, combining public health awareness is key. Behaviour change is a process, not an event, so it is necessary to remind inhabitants about hygiene and sanitation continuously. According to the trans-theoretical model, (TTM) “ behavior change is a cyclical process with individuals moving through distinct stages.” considering the history of the district being part of the CLTS program in which some of its towns were declared open defecation free, reintroducing the program could start with the district on a contemplation stage of the TTM model [16]. The success of any community health program lies in health education and awareness.
Open defecation exposes females to insecurity. It increases the risk of sexual violence and physical harrassment. violence and physical harassment. It creates mental trauma and fears of being rape [17]. This statement is true because whenever a female is sexually harassed during open defecations, and the perpetrator succeeds, it instils the fear of even going to free themselves when jammed, as their mind will continue to reflect the previous experience.
Cultural beliefs and the associated public health implications of open defecation
A respondent from the focus group discussion said that they were born in the district and their eyes were open to using the bushes and open fields for defecation, hence, it has become their way of life more besides, even if there are toilet facilities in the various towns, it will still be challenging to stop open defecation, as they spend much time on the farms, which have no toilet facilities. However, another respondent said that “as long as we can manage to build toilets in our towns, we are able to build them on the farm where we spend most of our time, for it is from the farm that we get those local materials to build in the various towns”. A respondent narrated that she felt embarrassed on an occasion where a group of men went to their farmland to brush, in the process, she felt the urge to defecate, but the surroundings were not conducive as the presence of the people could not permit her, she had to walk a little distance “bush away from bush” to free herself. Another respondent also said that she nearly got bitten by a snake while using the bush for defecation. Moreover, she said she is becoming convinced that the health education given by healthcare providers every time they go to the clinic about drinking “pupu water” is correct, because she and her children most often suffer from “running stomach”. One participant also added by saying “ my son, the health people can really talk ot us when we go to the hospital, but when we return, we start to do the same thing because we stay long doing it, and so it is not easy to forget about it.

Figure 3 CLTS Communities Status in Todee Health District.
Considering the information in Figure 3 from the Liberia Ministry of Health, National Technical Coordinating Units (MOH-NTCU) master Community Led Total Sanitation (CLTS) data-based 2025. The Todee health district has 96 CLTS communities. By August 2016, 76 of the communities had achieved Open Defecation- Free (ODF) status, with 20 still practising Open Defecation (OD). The focus group discussion revealed that this achievement was the result of the constant monitoring and supervision by the Government and the passionate staff of Global Communities, an International non-profit Organisation whose mission is to empower local communities to take the lead in their own development. Nevertheless, since the closure of NGO operations, most of the declared open defecation-free communities have reverted to their previous states. Citizens are no longer feeling obligated to lead their sanitation activities.
Since the community approach has a long-standing track record of changing negative cultural phenomena, there is an emerging need to restructure the community component of health to yield maximum results. Behaviour change is a long process that requires consistency and commitment. According to Adabya et al (2023), in the title “Changing a Community: A Holistic View of the Fundamental Human Needs and Their Public Health Inpacts” high-quality education and job training are essential for promoting community safety when aiming to enable equitable access to critical aspects of the community [18].’ Achieving a sustainable, positive impact requires innovation, motivation, and using a variety of theories and methods, as a single method might not solve most problems across different communities.
Open defecation has numerous associated effects, predominantly affecting females and children under five, including child malnutrition and lack of social dignity. For example, when open defection is done, and rain falls, it washes away the faeces into any nearby water. This is dangerous, especially for those in rural areas who use running water for drinking and other domestic activities. The faeces travels with many bacteria, looking for a susceptible host to reproduce [19]. Worm infections, along with diarrhoea, are among the primary causes of malnutrition and stunting among children under five.
CONCLUSION
Open defecation remained a major challenge in Liberia as traditional and cultural influences continued to serve as a stumbling block. Limited resources and commitment to duties cannot be overemphasised, as there is less commitment, which keeps depleting the efforts of donor funds. The situation is the leading cause of significant health implications, primarily in women of childbearing age and children under five.
Recommendations :
- Build a system of intersectorial collaboration involving the traditional leaders on the planning and implementation of community development programs.
- The reintroduction of the CLTS program and the development of a monitoring and evaluation framework will significantly help achieve and sustain the program.
- We recommend that Environmental Health Professionals be given the necessary support to reinforce community supervision.
- We also recommend the training of healthcare providers in using a multidimensional approach to address the sanitation issue of the district, including the participatory hygiene and sanitation transformation (PHAST) approach.
REFERENCES
- Jaehyang So, Spears D. Ending Open Defecation, Not by Evidence Alone. World Bank Blogs. 2013.
- Ismail AM, Ibrahim MA, Abdi MM, Geremew A, Mulugeta Y, Ayele DM, et al. Open defecation practice among households with latrines in rural communities of Ararso District, Somali Region, Eastern Ethiopia. Front Public Health. 2024; 12: 1394351.
- UNICEF. Ending Open Defecation | UNICEF. 2017.
- Akindayo D. Tackling open defecation in Nigeria. 2025.
- Ismail AM, Ibrahim MA, Abdi MM, Geremew A, Mulugeta Y, Ayele DM, et al. Open defecation practice among households with latrines in rural communities of Ararso District, Somali Region, Eastern Ethiopia. Front Public Health. 2024; 12: 1394351.
- Luke N, Acharya Y, Faytong-Haro M, Yang D, Xu H, Oommen AM, et al. Open Defecation, Livestock Ownership, and Child Nutritional Status in India. Am J Trop Med Hyg. 2024; 110: 1263-1269.
- World Bank. Inadequate Sanitation Costs 18 African Countries Around US$5.5 Billion Each Year. 2012.
- Baddianaah I, Naazie GK, Amaning AWZ, Terkper P. Women’s sanitation matters: Unpacking the conundrums associated with open defecation among women in Harper City, Liberia. Environ Chall. 2024; 16: 100965.
- Bhatt N, Budhathoki SS, Lucero-Prisno DEI, Shrestha G, Bhattachan M, Thapa J, et al. What motivates open defecation? A qualitative study from a rural setting in Nepal. PLoS One. 2019; 14: e0219246.
- Saleem M, Burdett T, Heaslip V. Health and social impacts of open defecation on women: a systematic review. BMC Public Health. 2019; 19: 158.
- WHO. Diarrhoeal disease. 2024.
- World Life Expectancy. Diarrhoeal diseases in Liberia. World Life Expectancy. 2020.
- Sahiledengle B, Petrucka P, Desta F, Sintayehu Y, Mesfin T, Mwanri L. Childhood undernutrition mediates the relationship between open defecation with anemia among Ethiopian children: a nationally representative cross-sectional study. BMC Public Health. 2024; 24: 1484.
- Morales F, Montserrat-de la Paz S, Leon MJ, Rivero-Pino F. Effects of Malnutrition on the Immune System and Infection and the Role of Nutritional Strategies Regarding Improvements in Children’s Health Status: A Literature Review. Nutrients. 2023; 16: 1.
- Raihan N, Cogburn M. Stages of Change Theory. In: StatPearls. StatPearls Publishing; 2025.
- Tallman PS, Collins S, Salmon- Mulanovich G, Rusyidi B, Kothadia A, ColeS. Water insecurity and gender-based violence: A global review of the evidence. WIREs Water. 2023; 10: e1619.
- Adabanya U, Awosika A, Moon JH, Reddy YU, Ugwuja F. Changing a Community: A Holistic View of the Fundamental Human Needs and Their Public Health Impacts. Cureus. 2023; 15: e44023.
- Balasubramanian C. What is the chain of infection & how to break it? Explainer. GIDEON. 2023.









































































































































{kind=link}