Verification of a Mathematical Model of Mitral Chordae Length in Echocardiography as a Function of Their Manual Measurement
- 1. Department of Cardiology, Amiens Picardie University Hospital Center, France
- 2. Department of Cardiac Surgery, Amiens Picardie University Hospital Center, France
Abstract
Aim: In this study, we sought to verify a mathematical model, ME = 0.87 * MM + 4, by performing tests on a sample of individuals with known chordae length by echographic measurement.
Patients & methods: This report presents a retrospective analysis of 191 patients who underwent mitral valve repair.
This validation analysis was carried out with the same sample of participants that we previously published in the “Journal of Cardiothoracic Surgery” under the name “Modeling of mitral chordae’s length in echocardiography as a function of their manual measurement in the operating room”.
The entire sample (N = 191) was randomly divided into two subsamples:
→ Learning data: 70% (134) of the total sample and was used to train and develop the mathematical model.
→ Test data: 30% (57) of the total sample and was used to evaluate the performance of the predictive mathematical model.
Results: In our analysis, we obtained an RMSE of 1.108, indicating good model performance and validity.
We demonstrated by Student’s t-test that the model accurately predicts echographic mitral chordae length, and that there is no statistically significant difference between predicted and actual echographic values. echographically measured mitral chordae length.
We also visually demonstrated a linear relationship with no significant outliers, indicating good alignment between predicted and actual values of echographically measured mitral chordae length.
Conclusions: The results of this validation not only improve the applicability of the model, but also provide clinicians with a valuable tool for making informed decisions about patients’ cardiac health.
Keywords
• Correlation
• Linear Analysis
• Prediction
• Modelisation
• Mitral Tendinous Chordae
• Mitral Valve Repair
CITATION
GUN M, BARRY M (2023) Verification of a Mathematical Model of Mitral Chordae Length in Echocardiography as a Function of Their Manual Measurement. Ann Biom Biostat 6(1): 1040.
ABBREVIATIONS
TEE : Trans-Esophageal Echocardiography ; EM : Echographic Measurement ; MM : Manual Measurement ; RMSE : Root mean square error; R² : Determination coefficient; r : Correlation Coefficient Ho : Null Hypothesis ; H1 : Alternative Hypothesis; N : Total Population ; α : Alpha risk
INTRODUCTION
A mathematical model previously published in the “Journal of Cardiothoracic Surgery” has been proposed by GUN et all. [1] to estimate mitral chordae length, particularly in cases where preoperative echographic measurements are not possible due to patient-related contraindications to transesophageal echocardiography.
Neo-chordae implantation for mitral valve repair involves replacing broken or elongated chordae with artificial chordae made of Gore-Tex braids. This technique makes it possible to correct mitral leaks while preserving posterior valve mobility.
The model in the published article suggests that intraoperative manual measurements of mitral chordae can be used as a basis for estimating the length of artificial chordae to be implanted. This length corresponds to that of the echographic measurement.
In this study, we sought to verify the mathematical model by performing tests on a sample of individuals whose chordae length by echographic measurement is known.
PATIENTS & METHODS
To verify and validate the mathematical model, the patients recruited were among those who underwent immediate preoperative transesophageal echocardiography and mitral plasty by chordae substitution. This made it possible to accurately measure the length of their native mitral chordae.
This report presents a retrospective analysis of 191 patients who underwent mitral valve repair. The study population comprised 130 men and 61 women, giving a sex ratio (M/F) of 2.13. Mitral valve chordae measurements were therefore performed by transesophageal echographic immediately preoperatively, followed by manual measurements intraoperatively. The data collection period ran from January 2008 to December 2016, and patient medical records from the cardiology and cardiac surgery department of the Centre Hospitalier Universitaire d’Amiens in Picardy were used for analysis.
CONCLUSION
This report focuses on the validation and generalization of a mathematical model developed to estimate mitral chordae length in patients who cannot undergo transesophageal echocardiography (TEE) due to contraindications. Through rigorous validation and evaluation, we demonstrate the performance and reliability of the proposed model, presenting it as a promising alternative for estimating mitral chordae length. The results of this validation not only improve the applicability of the model, but also provide clinicians with a valuable tool for making informed decisions regarding patients’ cardiac health. In addition, to further strengthen the validity of the model, we describe our plan to apply it to a new representative sample, to ensure its ability to generalize to novel data.
ANALYSIS
Study design
The validation study was carried out with the same sample of participants. We randomly divided the total sample (N = 191) into two sub-samples:
Test data: This sub-sample constitutes 30% (57) of the total sample and was used to evaluate the performance of the predictive mathematical model.
Training data: This sub-sample constitutes 70% (134) of the total sample and was used to train and develop the mathematical model.
Setting up and fitting the model to the training data
We used a simple linear regression model to establish the relationship between the dependent variable (echographic measurements) and the independent variable (manual measurements). By fitting the model to the training data, we estimated the model parameters, including slope and intercept, which describe the linear relationship between the variables. The objective was to find the best-fit line that minimizes the sum of squared differences between the observed values of the dependent variable and the predicted values given by the linear equation. In our analysis, the resulting mathematical equation was ME = 0.87 * MM + 4, where EM equals the length of echographic measurements and MM, the length of manual measurements.
Model evaluation
To assess the performance of the mathematical model in estimating mitral chordae length, we compared the predicted values with the actual values of the dependent variable using the test data set. Two evaluation measures were used:
→ Root mean square error (RMSE): RMSE measures the mean deviation between predicted and actual values of the dependent variable. A lower RMSE indicates better model performance, while values close to zero indicate a perfect fit. In our analysis, we obtained an RMSE of 1.108, indicating good model performance and validity.
→ R-squared score (R²): The R² represents the proportion of variance in the dependent variable that can be predicted from the independent variable.
A higher R-squared value (closer to 1) indicates a better fit. In our analysis, we obtained a coefficient of determination of 0.81, indicating that 81% of the variation in echographic measurements can be explained by manual measurements.
Predictions on data test
Using the fitted model, we generated values predicted by test data. We estimated echographic measurements based on manual measurements of the test data. This enabled us to assess the model’s ability to generalize to new data, and provided valuable information for decision-making.
Visualization of results
To visually represent the model’s predictive performance, we have drawn a scatter plot of the predicted versus actual values of the dependent variable (echographic measurements) (Figure 1) from the test sample.
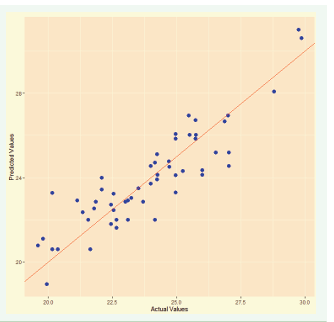
Figure 1: Visualization of the predictive and actual values of echographic measurements.
Each data point on the plot represents a pair of predicted and actual values. The more the points align with the diagonal line (y = x), the more the model’s predictions match the actual values. We observed a strong linear relationship with no significant outliers, indicating good alignment between predicted and actual values.
Data = testData = sub-sample of base population.
X = actual values of echographic measurements = observed values of the dependent variable.
Y = predicted values = estimated values of echographic measurements (dependent variable) generated by the model on the basis of the initial values of the independent variable (predictor variable).
We also used the Student’s t-test to assess the significance of the difference between the predicted and actual values of the “ echographic measurements” variable:
- Null hypothesis (H0): The mathematical model does not accurately predict the length of mitral chordaes measured echographically.
- Alternative hypothesis (H1): The mathematical model accurately predicts echographically measured mitral chordae length.
- Null hypothesis (H0): There is no significant difference between the predicted and actual values of the dependent variable (echographic measurements).
- Alternative hypothesis (H1): There is a significant difference between the predicted and actual values of the dependent variable (echographic measurements).
We have demonstrated by Student’s t-test that the model accurately predicts echographic mitral chordae length, and that there is no statistically significant difference between echographic predicted values and echographic actual values (p_value: 0.84).
STUDY LIMITATIONS
In presenting the outcomes of our study, we recognize the importance of addressing certain inherent limitations, acknowledging their significance in the context of our findings.
Surgical Measurement Considerations
While our investigation successfully demonstrated a noteworthy correlation between echocardiographic and surgical measurements of mitral chordae, it is crucial to consider the potential impact of perioperative factors on surgical measurements. Awareness of these nuances enhances the interpretative framework of our results.
Application Scope Contraindications to Cases without TEE
Our model, designed specifically for estimating mitral chordae length in patients with contraindications to transesophageal echocardiography (TEE), excels within this targeted population. Its implementation in diverse clinical scenarios should be approached judiciously, recognizing its exceptional utility within its designated scope.
Ongoing Positive Prospective Validation
Recognizing the evolving nature of our work, we wish to highlight the ongoing prospective validation of our model on a novel sample. This forward-looking validation process serves as a testament to our commitment to refining and enhancing the robustness of our mathematical model.
Consideration of Individual Variability
Despite meticulous control of variables, the inherent variability associated with individual factors in studies of this nature is acknowledged. This acknowledgment underscores our commitment to transparency, ensuring that readers and clinicians approach our findings with a nuanced understanding of potential individual influences.
In light of these considerations, we remain optimistic about the substantial positive impact our model brings to the realm of clinical decision-making. Embracing these limitations as opportunities for further refinement, we believe our work contributes significantly to the field.
DECLARATIONS
Ethics approval and consent to participate
The study protocol was approved by the Local Ethic Committee of the University Hospital of Amiens of Picardie, France, for the handling and analysis data (CEERNI-ID number: 114-January 29, 2013).
The trial has been registered under the following clinical trial registry number (clinicaltrials.gov): NCT03113552 and Protocol ID: PI2013_843_0002 with Primary Completion Date: July 4, 2025.
The declaration number to the Paris-CNIL (8 rue vivienne 75083 Paris, cedex 2): 1665485.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
Mesut GUN, Eng: ideation, database, writing, statistic ; Misbaou BARRY, MD, PhD : supervision, revision.
Authors’ information
Mesut GUN: Research engineer for the Heart-Chest-Vascular Center, University Hospital Center, Amiens, France
Misbaou BARRY: Heart-Chest-Vascular Surgery Center, University Hospital Center, Amiens, France








































































































































{kind=link}