Highly Suspicious Malignant Hyperthermia: A Case Report
- 1. Anesthesia Department of West China Hospital, Sichuan University, China
- 2. Ultrasonic Department of West China Hospital, Sichuan University, China
Abstract
Malignant hyperthermia (MH) crisis could be fatal during general anesthesia. We report a case of a 34-year old male who was scheduled to undergo bilateral tonsillectomy with diagnosis of left tonsil mass, chronic tonsillitis and obstructive sleep apnea-hypopnea syndrome (OSAHS). The patient inhaled 3% sevoflurane for 5 minutes mask ventilation with bag was well for his pre-oxygenation procedure. During induction of anesthesia, the patient developed masseter muscle rigidity (MMR) rapidly following administration of succinylcholine, but laryngoscopy was still available. Low-flow sevoflurane was inhaled after the intubation. The patient suffered from hypercapnia (55mmHg), slightly increase of temperature, sinus tachycardia, combined metabolic-respiratory acidosis during intraoperative period. The patient was temporary diagnosed with malignant hyperthermia and treated accordingly. Further the patient was carefully monitored and investigated to exclude other possible conditions in postoperative period. The patient was highly suspected MH according to the DNA analysis. He was discharged from the hospital without any complication and discomfort.
Keywords
• Malignant hyperthermia (MH)
• Masseter muscle rigidity (MMR)
• Succinylcholine
• Volatile anesthesia
Citation
Zeng X, Zhang Y, Li S, Chen G, Chi D, et al. (2016) Highly Suspicious Malignant Hyperthermia: A Case Report. Ann Clin Exp Hypertension 4(2): 1038.
ABBREVIATIONS
MH: Malignant Hyperthermia; MMR: Masseter Muscle Rigidity; CKP: Creatine Phosphokinase; EtCO2 : End-tidal Carbon dioxide Pressure; SR: Sarcoplasmic Reticulum; AST: Aspartate Aminotrans Ferase; OSAHS: Obstructive Sleep Apnea-hypopnea Syndrome; T: Temperature; HR: Heart Rate; RYR1: Ryanodine Receptor
INTRODUCTION
Malignant hyperthermia (MH) is a hyper metabolic, lethal syndrome triggered by anesthetic drugs in those genetically susceptible individuals [1]. The Pathophysiology of MH is related to altered sarcoplasmic reticulum (SR) calcium release channel. Two genes’ mutation has been reported associated with MH: ryanodine receptor subtype 1(RyR1) and CACNA1S [2]. During MH episode the SR calcium channels open persistently and responding calcium influx causes sustained muscle contraction and increased metabolism of oxygen and glucose resulting in acidosis, rigidity and hyperkalemia. Sustained muscle contraction expands large number of adenosine triphosphate. Consumption of cellular adenosine triphosphate stores finally leads to rhabdomyolysis and release of the contents of cells (e.g., potassium, creatine phosphokinase, and myoglobin) [3,4]. Increased metabolism accounts for hyperthermia and a high level of end tidal CO2 (EtCO2 ) out of proportion to clinical setting indicates MH during anesthesia because persistent metabolism lead to increased oxygen consumption, hypoxia, progressive lactate acidosis, excessive production of CO2 , and increased body temperature [5].
We here present a case showing all the clinical signs and symptoms of malignant hyperthermia after administration of succinylcholine and sevo sevoflurane in a patient who was scheduled to undergo tonsillectomy.
CASE PRESENTATION
A 34-year old and 85 kilograms male who was scheduled to receive bilateral tonsillectomy under general anesthesia was diagnosed with left tonsil mass, chronic tonsillitis and obstructive sleep apnea-hypopnea syndrome (OSAHS). This patient has suffered sleep apnea-hypopnea at night for half a year, 1 to 2 times/month, no dizzy or sick at the next morning.
According to pre-anesthetic physical examination, there was no significant finding except for bilateral tonsil enlargement (II°). The mouth opening of this patient was 4.5cm with a 5.5cm thyromental distance and no abnormality was found in the extension of the atlanto-occipital joint. The Mallampati grade was II°.
Routine adjunctive investigations such as complete blood count, coagulation parameters, liver and kidney function and ECG were all negative and no allergic history was found. The result of polysomnogram indicated apnea recurrent 5 times during sleep and apnea hyponea index was about 6 times/h. In 2009, the patient received cholecystectomy under general anesthesia and no significant complication was found.
On the day of surgery, the patient was taken to operation room with flat wagon at 10:45 am. The pulse oximeter and cardiac monitor were attached immediately. His heart rate was 98 beats per minutes and blood pressure was 142/90 mmHg. Saturation of Pulse Oximetry (SpO2 ) on air was 100%. The patient fall asleep after inhaled 100% oxygen at flow of 5L/min and 3% sevoflurane for 5 minutes, mask ventilation with bag was well for his pre-oxygenation procedure. Introduction was intravenously midazolam 2mg, sufentanil 25ug, propofol 200mg and scoline 100mg. On attempting laryngoscopy, the patient was found to have systemic muscle tremors and 30 seconds later, little difficulty in opening mouth and masseter muscle rigidity were developed. Laryngoscopy was still available and a 7.5 reinforced endotracheal tube was placed successfully. Then cis-atracurium 10mg was given intravenously and 1-1.5% sevoflurane were used to maintain anesthesia. HR, SPO2 , NIBP and EtCO2 were regularly recorded during operation. However, 10 minutes after intubation, the EtCO2 maintained at or over 55mmHg all the time. Suspecting problems associate with high-level EtCO2 was examined at this moment: (1) the location of endotracheal tube was normal without bending and auscultated lung indicated breath sounded symmetrically without wheezes or moist crackles. (2) A new soda lime tank was used, but EtCO2 did not improve. (3) Anesthesia machine respiration valve ran normally. Slight hyperventilation was administrated at this time. Tidal volume was increased to 600-700ml and respiratory rate was accelerated to 25 bpm. The airway pressure was 20cmH2 O, but there is no decline of EtCO2 5 minutes later. At 11:15 am, axillary temperature of the patient was 37.7 and EtCO2 was 57 mmHg. Cis-atracurium 10mg and sufentanil 20ug were boosted intravenously again at 11:25am. 10 minutes later, surgeons feed it back that muscle tension was still very high. At this time, axillary temperature was 37.6 and EtCO2 was 56mmHg. MH was highly suspicious. The sevoflurane was removed immediately and 100% oxygen at flow of 8L/ min was used. Another anesthesia machine was changed for ventilation. Propofol 6mg/Kg/h and remifentanil 0.15ug/Kg/min were applied to maintain anesthesia. Vital signs were monitored carefully: BP 90-100/50-60mmHg, HR 100-105bpm, EtCO2 54- 57mmHg, T 37.5-37.6, SPO2 100%.
At 11:40 am, an ABG done showed: pH 7.199, PaCO2 61.3 mmHg, PaO2 113.5 mmHg, HCO3 - 23.4 mEq/L, BE -5.69 mmol/L, SO2 98%, K+ 4.45 mmol/L, Ca2+ 1.073 mmHg. Surgery ended at 12:00 with temperature 37 and EtCO2 56mmHg. The patient recovered at 01:05 pm with temperature 37.7 and EtCO2 45mmHg (Spontaneous breath on air). Extubation was successfully.
The patient was back to the ward after careful observation in PACU. First day after surgery the patient’s highest temperature was 37.1. He complained about pharyngeal pain and discomfort especially when he swallowed, the whole body muscle soreness. His urine was tawny without urgent urination, frequent micturition or urodynia and osphyalgia. Nephrologists suggested alkalize urine; fluid infusion and diuretic to ensure urine volume reach 300ml/h. On the third day after surgery, the whole body muscle soreness remitted partly, urine was faint yellow, and temperature was 37.0. On the fifth day after surgery, the whole body muscle soreness remitted completely, urine also was faint yellow, temperature was 37.2. Serum myoglobulin and creatine phosphokinase rose severely in 24 hours post operation then gradually reduced to normal Table (1). Renal function, coagulation function and electrolyte were normal during the postoperative period.11 days after surgery the patient discharged without any complication or discomfort.
In this case, we found multiple heterozygous mutations by DNA analysis in the patient’s RYR1 Figure (1a-1d). The consequence of his younger sister was negative, but his parents’ gene mutation was found in RYR1 which also related to MH (Table 2).
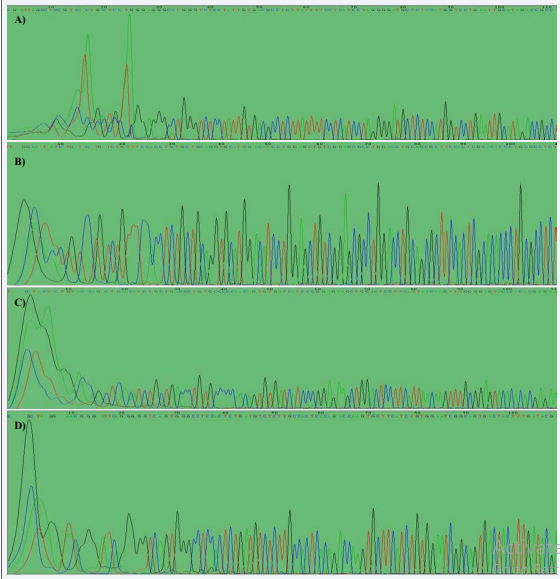
Figure 1 The mutation in exon of the patient. A: The mutation in exon 14-16. B: The mutation in exon 34. C: The mutation in exon 52-53. D: The mutation in exon 103-104.
DISCUSSION
Clinical presentations of MH are various from slight or moderate symptoms to fatal MH crises cause by severe skeletal muscle hyper metabolism and rhabdomyolysis [6]. However, it was an atypical MH in this case. The clinical manifestations were characterized by masseter muscle rigidity (MMR) following intravenous succinylcholine, moderate rise of EtCO2 and slightly increase of temperature. It is very interesting that the patient did not suffered from severe hyperpyrexia at all. Some other cases also reported no significant changes in body temperature, particularly when appropriate treatment was started early [7,8]. The moderate clinical presentation due to the early suspicion of MH and rapidly appropriate treatment. The severity of MH also depended on the dose of triggering agents, such as volatile anesthetics or succinylcholine, which was given to the patient [9]. A small amount of sevoflurane was inhaled during the beginning of the surgery in this case.
A clinical grading scale considered a useful tool for detection of MH [10]. Among seven criteria of this score there are four criteria. i.e. masseter spasm following succinylcholine (15 points), ETCO2 >55mmHg with appropriately controlled ventilation (15 points), Arterial pH <7.25(10 points) and inappropriate sinus tachycardia(3 point) were present in this case, leading to a total score of 43 corresponding to MH rank 5, classified as ‘MH Very likely’[11].
Compared with the invasive contracture test, DNA analysis is becoming more and more important over the last decades [12,13].As we known, there are three mammalian isoforms of the ryanodine receptor: RYR1, expressed in skeletal muscle; RYR2 , predominant in heart muscle; RYR3, found in skeletal and smooth muscle [14,15]. Many mutations in the RYR1 gene have been connected with a susceptible to MH [16]. Multiple mutations in RYR1 which are associated with MH, were found in the patient’s and his parents’ DNA [17]. So it’s very essential to ask the patient questions about individual or family history of MH in every preanesthetic interview.
The early suspicion of MH and rapidly appropriate treatment lead to favorable prognosis of a MH crisis [6]. In this case, MH was suspected by masseter muscle rigidity (MMR), high level of EtCO2 and slightly increase in temperature then immediate treatment (including stopping the trigger agents, removing the volatile anesthesia from the anesthesia machine hyperventilating with 100% oxygen at maximum fresh gas flow, turning to total intravenous anesthesia) was initiated [18]. Dantrolene as a specific medicine for crisis of MH can decrease the mortality rate prominently [19,20]. In this case, the favorable prognosis without administration of dantrolene was due to early diagnosis and treatment.
Without severe Hemodynamic changes and pulmonary complications, after operation, the patient was recovery and extubated successfully in the operation room. Patient was carefully monitored and investigated in postoperative period and a severe rise in creatine phosphokinase and myoglobin level was recorded at 24 hours. Most patients were killed by acute renal failure cause by high level of myoglobin during the post-operation. Thus, fluid infusion and diuretic were employed to prevent acute renal failure in our case [8].
In conclusion, the prognosis of a MH crisis depends on close observation and early diagnosis of MH. Rapidly appropriate treatment including initial and symptomatic treatment is crucially important as well. Masseter muscle rigidity (MMR) following trigger agents (succinylcholine and volatile anesthetic), increase in temperature and EtCO2 should be suspicious MH. Repeated arterial blood gas analysis and monitoring of serum electrolyte, creatine phosphokinase and myoglobin are also important leading to the success of therapy.
Table 1: change of creatine phosphate kinase and myoglobin. The surgery day is On October 30, 2014
| Date | creatine phosphate kinase (IU/L) | myoglobin (ng/ml) |
| 2014-10-28 | 762 | Without test |
| 2014-10-31 | 196748 | >3000.00 |
| 2014-11-01 | 121252 | 2546.00 |
| 2014-11-02 | 80783 | 1059.00 |
| 2014-11-03 | 42831 | 676.30 |
| 2014-11-04 | 10972 | 406.60 |
| 2014-11-06 | 2530 | 188.40 |
| 2014-11-08 | 1161 | 127.80 |
| 2014-11-10 | 851 | 95.06 |
Table 2: the mutation in RYR1 of patient and his family.
| 14-16 | 34 | 52-53 | 103-104 | |
| Patient’s father | normal | normal | normal | 100th of Exon 103: A>C |
| Patient’s mother | normal | normal | 28th of intron 53:G\A SNP rs2915953; 98th of intron 52:C\G rs3829976 |
normal |
| Patient | 92th of exon 15: G\A SNP rs2288888; 22th of intron 15:G\C SNP rs2288889 |
At the point of 127bp: C\T SNV COSM249669 | 98th of intron 52: C\G rs3829976; 27th of exon 53: G\A SNP rs2915952; 28th of intron 53: G\A SNP rs2915953 |
From 89th of intron 103: deletion of GGGGTG SNP rs369582296 |
| Patient’s younger sister | The same to the patient | normal | normal | normal |
ACKNOWLEDGEMENTS
All the co-authors are positive about what I sent. Dongmei Chi helps me collecting material and translating the report. Shuting Li supervise the procedure of the work. The DNA was analyzed by You Zhang.
REFERENCES
1. Bandschapp O, Girard T. Malignant hyperthermia. Swiss Med Wkly. 2012; 142: 13652.
9. Hopkins PM. Malignant hyperthermia: pharmacology of triggering. Br J Anaesth. 2011; 107: 48-56.
14. Fill M, Copello JA. Ryanodine receptor calcium release channels. Physiol Rev. 2002; 82: 893-922.
15. Hamilton SL. Ryanodine receptors. Cell Calcium. 2005; 38: 253-260.







































































































































{kind=link}