Tramadol Toxicology and Road Traffic Crashes: A Case Report
- 1. Department of Pharmaceutical Chemistry, University of California, USA
Abstract
This Report describes a road traffic crash fatality involving the opiate Tramadol, discusses the differences between US DUI classifications for Tramadol and those of EU nations, and recommends that US DUI classifications for prescription medicines incorporate appropriate EU standards as an important goal in patient safety, medicinal chemistry, and drug design. The identities of individuals, vehicles, and locations have been disguised for reasons of patient privacy.
Citation
Wolf ME (2014) Tramadol Toxicology and Road Traffic Crashes: A Case Report. Ann Med Chem Res 1(1): 1002.
CASE PRESENTATION
In July of 2012 at 11 PM in the Western US, an accident occurred at the intersection of Road 1 and Road 2. At the intersection, eastbound Road 1 and westbound Road 1 each consist of two travel lanes with right turn only lanes and center left turn lanes. Southbound Road 2 intersects with the north side of westbound Road 1; a stop sign and a lighted “Cross Traffic Does Not Stop” sign are posted at the intersection. Car_1 driven by Driver1 was stopped southbound on Road 2 at this intersection; Driver1 then attempted to turn left into eastbound Road 1. Car2 driven by Driver2, and a Car3 were westbound on Road 1 at 60- 70 mph east of the Road 2 intersection. Driver1 pulled out into this traffic in Car_1 and was hit on the left (driver’s) side by Car2, fatally injuring Driver1 and severely injuring Driver2.
(1) Car3 Westbound on Road 1
(2)Car2 Westbound on Road 1 (East)
(West) Road 1
Road 2 (North) Driver1 in Car_1
According to a witness in Car3, no cars other than Car_1, Car2, and Car3 were in the immediate area, and Driver1 should have waited: “no person in their right mind” would have driven into the oncoming traffic.
In a report dated shortly after the night of the accident, the Medical Examiner wrote that the Manner of Death of Driver1
was “Accident” and the Immediate Cause of Death was “Blunt force injuries of the torso and extremities” due to “Motor vehicle accident”. Toxicology examinations of the blood of Driver1 were completed by the toxicologist with the following results: Volatiles Screen including ethanol, negative; Cocaine Screen, negative, Methamphetamine Screen, negative, Morphine Screen, negative, THC Screen (for marijuana) negative. A test for carbon monoxide was reported as 2.6% carboxyhemoglobin (COHb) without comment. This is a standard test for carbon monoxide in blood. R.C. Baselt’s standard reference (Disposition of Toxic Drugs and Chemicals in Man, 6th Edition (2002)) states “COHb averages1-2% in urban non-smokers and 5-6% in smokers”. The single prescription drug found in Driver1’s blood by the toxicologist’s Gas Chromatography/ Mass Spectrometry Rx Drug Panel screen was Tramadol, at a concentration of 0.21 micrograms per milliliter (equivalent to 0.21 milligrams per liter or 210 micrograms per liter)
DISCUSSION
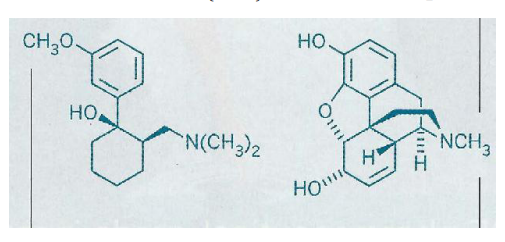
As shown above, Tramadol (left) has the essential medicinal chemical features of morphine (right) and consequently has pharmacological effects that result in its action as a potent
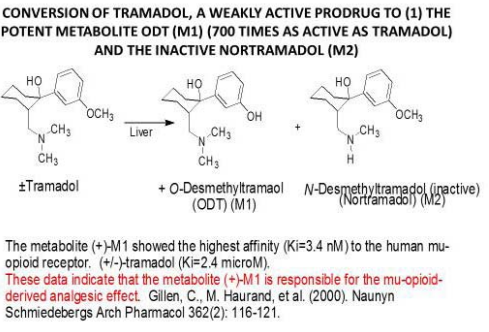
analgesic. Because of two asymmetric centers in the molecule, this drug substance is used as the racemic (±) 2-[(dimethylamino) methyl]-1-(3-methoxyphenyl) cyclohexanol. As with codeine, the methyl ether function in Tramadol is subject to metabolic attack by the liver enzymes CYP2D6 and CYP3A4, in this case to produce the potent metabolite O-desmethyl Tramadol (ODT) and the inactive metabolite N- desmethyltramadol (nortramadol) as shown; levels of these metabolites were not measured in the toxicology examination of Driver1’s blood. Although only the levels of Tramadol itself (which may be considered a prodrug) are available for this case, the same is true in most road crash studies [1]. Thus, as in the literature studies, it is assumed that the Tramadol level is an index of the ODT level in reaching the conclusions in the present case.
It is well known that psychoactive medications including alcohol and others have the power to affect driving in a dose dependent manner as shown (Figure 1).
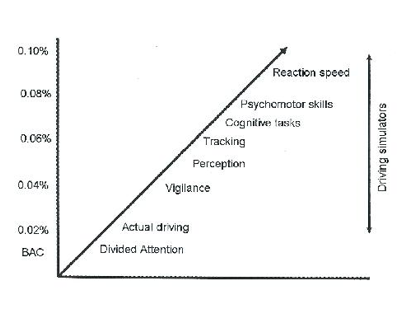
Figure1. Effect of Blood Alcohol Levels (BAC) on Driving Simulations
The mental abilities that are affected include, vigilance, perception, tracking, cognitive tasks, psychomotor skills and reaction skills. Laws exist to regulate these negative effects on driving performance. For example, most US states impose a limit of 0.08% BAC (blood alcohol concentration) on drivers of passenger autos. However, in the US such legal limits do not exist for prescription drugs.
By contrast, in the EU there are many such limits for prescription drugs [2].In Europe, drugs are allocated to one of the following International Council on Alcohol, Drugs, and Traffic Safety (ICADTS) categories:
I. Presumed to be safe or unlikely to produce an effect. These drugs are Equivalent to a BAC of less than 0.05%. II. Likely to produce minor or moderate adverse effects. Approximately equivalent to a BAC of 0.05%-0.08%.
III. Likely to produce severe effects or presumed to be dangerous. Approximately equivalent to a BAC greater than 0.08%. Morphine and Tramadol are Group III drugs in many EU nations
According to the FDA “Label” (i.e. the required package insert) single doses of Tramadol (50 mg.) given orally to geriatric adults produce peak blood concentrations of 208 ng/ml (0.208 micrograms/ml), in reasonable agreement with the level of 0.21 micrograms per ml found in Driver1’s blood. A recent investigation that included the blood concentration of Tramadol in drivers involved in road traffic crashes [1] included 9 cases in which Tramadol was the only drug present and shown to be present at a median concentration of 0.20 milligrams per liter. The median concentration is defined as the middle concentration in a series of concentrations. As there were 9 cases in this group, the middle of the series is the fifth individual and there were 5 of the 9 cases having a concentration of 0.20 milligrams per liter or lower. Tramadol, at a concentration of 0.21 micrograms per milliliter (equivalent to 0.21 milligrams per liter) was the sole drug found in Driver 1’s blood in the Rx Drug Panel on August 22, 2012. Driver1’s Tramadol blood concentration is virtually identical with the median concentration in the 9 crash cases in the Ahlner road traffic crash study, clearly showing that Driver1 was driving with a blood level consistent with an ICADTS Class III drug “likely to produce severe effects”, and a blood level found to be commensurate with responsibility for road traffic crashes.
The use of Tramadol as an analgesic has increased in both the EU and the US as a result of the withdrawal of propoxyphene because of adverse cardiac effects. This increased use of Tramadol has made it even more desirable to identify and codify drugs that diminish the ability of automotive drivers to properly operate their vehicles. The Driving under the Influence of Drugs, Alcohol and Medicines (DRUID) project in the EU [2] has placed a total of 40 CNS drugs be in the ICADTS Class III defined above. These CNS drugs included 3 opioids and other analgesics, 4 antiepileptic, 8 antipsychotics, 7 anxiolytics, 11 sedatives, and 7 antidepressants. The adoption in the US of a similar warning system for prescribers and patients would be an important step forward, and the reduction of these effects on driving performance would, likewise, be an important drug design goal for medicinal chemists.
REFERENCES









































































































































{kind=link}