Development and Validation of the Chinese Rapid Health Literacy Questionnaire for Primary and Secondary students
- 1. Chinese Academy of Medical Sciences and Peking Union Medical College, School of Health Policy and Management, China
Abstract
Health literacy is critical for shaping health behaviours in children and adolescents, yet there is a lack of an appropriate tool for measuring comprehensive health literacy employing grounded theory approaches. This study aimed to develop and validate a rapid health literacy questionnaire for primary and secondary students to address gaps in exiting tools. Firstly, a health literacy indicator system was constructed through literature analysis, Delphi method, and expert interviews. Secondly, for each domain indicator, items were generated. Finally, a stratified sampling survey with 3,325 primary students and 2,788 secondary students was conducted, Rasch analysis was applied to evaluate reliability and validity. Reliability analysis confirmed consistent results, demonstrating favourable overall fit between observed data and the model. Validity results showed internal consistency. We developed a robust assessment tool tailored to Chinese primary and secondary students, which is expected to comprehensively measure the health literacy of students aged 6 to 15 years. Future cross-cultural validation is recommended to enhance its global applicability
Keywords
• Health literacy
• Children
• China
• Test
• Tool
Citation
Guo J, Zan Z, Liu L, Wang Y, You L (2025) Development and Validation of the Chinese Rapid Health Literacy Questionnaire for Primary and Secondary students. Pediatr Child Health 13(3): 1356.
ABBREVIATIONS
CTT: Classical Test Theory; EFA: Exploratory Factor Analysis; GAMA: Global Action for Measurement of Adolescent health(WHO); HL: Health Literacy; HLS-EUQ47:European Health Literacy Survey Questionnaire; IRT: Item Response Theory; KMO: Kaiser-Meyer-Olkin; MOE: Ministry of Education of the People’s Republic of China; NHC: National Health Commission of the People’s Republic of China; NVS: Newest Vital Sign; PCA: Principal Component Analysis; REALM-Teen: Rapid Estimate of Adolescent Literacy in Medicine; SC: State Council of the People’s Republic of China; SCT: Social Cognitive Theory; s-TOFHLA: Short Test of Functional Health Literacy in Adults
INTRODUCTION
Health literacy (HL) has been defined as ‘the integration of skills, knowledge, and motivational drivers to access, understand, appraise, and apply health information for decision-making in healthcare, disease prevention, and health promotion contexts [1,2]. The WHO Integrated Model [3], synthesizes individual and population perspectives, highlighting HL as a dynamic process that requires alignment with societal systems to achieve health equity. Childhood and adolescence are formative years for learning and developing health behaviors and HL promotion during this period can significantly impact the quality of life in adulthood [4]. Children’s and adolescents’ HL are multidimensional, going beyond numeracy and literacy skills and developmental characteristics is related to use of HL skills [5,6].
The WHO has been engaged in a range of actions to promote HL as an enabling factor in promoting health in a whole-of-society approach [7]. Current studies have established some domain-specific assessment tools for children’s and adolescents’ HL, including nutritional/food literacy [8,9], physical health literacy [10], mental health literacy [11,12], however, there is a lack of an appropriate tool for measuring comprehensive children’ and adolescents’ HL-one that employs grounded theory approaches both to determine HL’s key attributes and to acknowledge it as a latent construct. By incorporating various topics, the tool can encompass the common daily activities where they engage in health-promoting actions and ensure that children’s and adolescents’ HL development includes all relevant dimensions [13]. Existing measurements have some main deficiencies: (1) insufficient cultural sensitivity, failed to fully capture the cultural factors [14]; (2) insufficient psychometric properties and quality lacking [15], which represents a severe weakness in a measure termed construct underrepresentation [16]. (3) insufficient age adaptability, which adapted from adult-centric instruments such as NVS [17], and s-TOFHLA [18], or lacking age-span perspective [19], resulting in being less precise when evaluating the different capabilities of specific age groups.
(4) insufficient content coverage, which place too much emphasis on functional health literacy and neglect the assessment of interactive and critical health literacy. (5) absence of digital health literacy. With the popularity of digital media, digital health literacy has become increasingly important [20,21], but some tools fail to fully assess the capabilities in this regard [19]. Studies on how frameworks that may be used to guide the development of HL measure for children and adolescents find that there exists theoretical insufficient and fragmentation, with HL conceptualization has been largely limited to concepts of adult HL in healthcare and disease prevention settings [22-25], and few tools involved children and adolescents in the development and conceptualization of HL [26]. Different studies use different definitions and tools, making it difficult to compare and integrate results [27]. The challenge is to develop more comprehensive, highly adaptable, and fully validated HL questionnaire which is context and content specific to better support health education and intervention efforts for children and adolescents. Specifically, in order to develop a tool that is sensitive to the wide range of potential HL needs of children and adolescents, including potential key mechanisms to support intervention development, as well as measuring potential intervention effects, a welltargeted, from a health promotion perspective, stagedevelopmental HL modelling is vital.
Therefore, we take increased independence around food choice, physical activity participation, sleep patterns and sexual expression into fully consideration throughout the transitional years. Previous researches have often utilized classical test theory (CTT) and item response theory (IRT) to validate scale reliability [28]. CTT faces limitations with measurement and sample dependency, whereas IRT correlates examinee ability with the likelihood of correct responses. Rasch analysis offers a probabilistic model for scale scoring, quantifying both respondent ability and item difficulty on a unified scale [29,30].
Therefore, we use Rasch analysis to evaluate the questionnaire’s difficulty, accuracy, and psychometric properties.In response to the findings of previous research, this study aims to define children’s and adolescent’s HL and develop a Chinese Rapid Health Literacy Questionnaire for primary and secondary students (CRHLQ-PS). Specific research questions include: (1) how can existing HL models be adapted to reflect children’s and adolescents’ cognitive, social, and emotional developmental needs? (2) what domains and competencies should be prioritized in a context-specific HL assessment tool? (3) does the proposed questionnaire demonstrate reliability and validity across age groups?
MATERIALS AND METHODS
Stage I: Development of the CRHLQ-PS
Step 1: Concept modelling: To identify candidate theories for HL modeling, we systematically searched PubMed, Web of Science, and CNKI (2000–2024). “health literacy” “eHealth literacy” “health competence” “health capability” “health empowerment” and “child/adolescent/ school-age/youth” were used as search terms.
Based on nutbeam’s hierarchical model and Bandura’s Social Cognitive Theory (SCT), we derived four core dimensions: (1) Knowledge: understanding foundational health concepts; (2) Skills: Ability to access, appraise, and apply health information; (3) Motivation: intrinsic drivers to engage in health-promoting behaviors; (4) Participation: active involvement in individual and collective health decision-making.
To address the limitations of prior adult-centric HL models, we introduced two distinctive features:(1) Developmental adaption: acknowledging cognitivebehavioral progression, the model integrates a developmental perspective: early primary (grades 1–2, ages 6–8), middle primary (grades 3–4, ages 9–10), upper primary (grades 5–6, ages 11-12), and junior high (ages 13–15). (2) Domain-specific articulation: while maintaining HL as a cross-cutting capacity, we embedded context-bound literacies validated in prior studies: eHealth literacy, nutrition literacy, physical literacy and mental health literacy.
The child- and adolescent- centric HL model synthesizes four core competencies—knowledge, skill, motivation, and participation. Distinct from adult-centric frameworks, the model advances HL measurement and intervention through developmental adaptation and domain-specific articulation, ensuring precision across evolving capacities and real-world health ecosystems.
Step 2: Indicator construction: Phase 1:
Policy Review: Firstly, we collected and analyzed the policy files
and data relevant to HL from government departments’ websites, including the State Council of the People’s Republic of China (SC), the National Health Commission of the People’s Republic of China (NHC), and the Ministry of Education of the People’s Republic of China (MOE) (Figure 1).
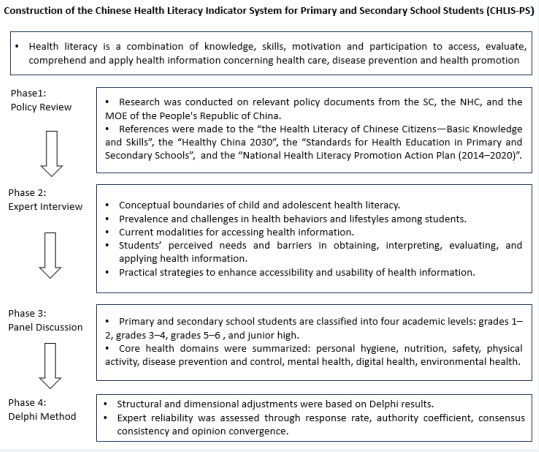
Figure 1 Procedures diagram of the health literacy indicator system construction Captions: figure showing the construction process of the Chinese health literacy indicator system for primary and secondary school students, which includes four phases: policy review, expert interview, panel discussion, and Delphi method, with details on key focuses at each phase and the definition of health literacy
Key documents, such as the Health Literacy of Chinese Citizens—Basic Knowledge and Skills [31], and Healthy China 2030 [32], emphasized knowledge, skill, motivation, and participation. Developmental benchmarks from the Standards for Health Education guided age-specific item design, while the Ecological Environment and Health Literacy (2018) informed contextually grounded domain like environment.
Phase 2: Expert Interview: Secondly, in semi- structured interviews and panel discussions with 13 multidisciplinary experts, key themes were discussed
including: (1) conceptual boundaries of child’s and adolescents’ HL; (2) Prevalence and challenges in health behaviors and lifestyles among students; (3) Current modalities for accessing health information (e.g., digital platforms, school-based resources); (4) Students’ perceived needs and barriers in obtaining, interpreting, evaluating, and applying health information; (5) Practical strategies to enhance accessibility and usability of health information.
Phase 3: Panel Discussion: Thirdly, eight health domain indicators were identified through many brainstorming sessions and discussions within the group. The domain delves into multiple key aspect indicators: eye, oral, and hand hygiene; food sanitation and nutrition; exercise, sedentary behavior and sleep; accidental injury prevention and natural disaster evacuation; nutrition- related, infectious, chronic and endemic diseases;
sociocultural adaptation, behavior regulation and psychological assistance; digital health access, evaluation and application; pollution exposure prevention and sustainable resource utilization.
Phase 4: Delphi Method: Finally, following established procedures of previous studies [33], the Delphi method was used to make structural adjustments of the initial version of the Chinese Health Literacy Indicator System for primary and secondary students (CHLIS-PS). Thirteen experts (all expertise in health promotion, behavioral science and child development) with at least 10 years of working experience in their field contributed to an online consultation of a structured questionnaire and proposed any additional amendments to the system. Then, experts were provided with relevant background information and asked to rate each indicator for their importance and appropriateness [34]. Expert reliability was assessed through: (1) Response rate; (2) Authority coefficient (Cr=[Ca+Cs]/2), where Ca (0.3-0.1) reflected judgment basis and Cs (0.2-1.0) indicated familiarity; (3) Consensus consistency (Kendall’s W, 0-1); (4) Opinion convergence. Open-ended feedback informed iterative revision.
After repeated deliberation and consideration, “environmental health” and “endemic disease” were deleted, “sexual and reproductive health” was added. Compared with grades 5-6 and junior high school students, grades 1-2 and 3-4 does not include the domain indicator “digital health literacy”, and does not include the aspect indicators “chronic disease” and “sexual and reproductive hygiene” (Figure 2).
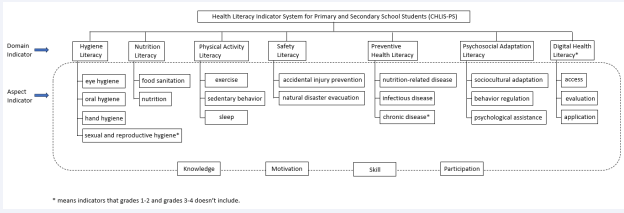
Figure 2 The Chinese health literacy indicator system for primary and secondary students. Captions: figure showing modifications to the health literacy indicator system, including deletion of “environmental health” and “endemic disease,” addition of “sexual and reproductive health,” and age-group adjustments: grades 1-2/3-4 exclude “digital health literacy,” “chronic disease,” and “sexual and reproductive hygiene” domains/aspects. Final questionnaire structure: 6 domain/16 aspect indicators for lower grades (1-4) vs. 7 domain/20 aspect indicators for upper grades (5-6) and junior high, tailored to different age groups.
Results achieved Cr=0.88, exceeding the 0.70 reliability benchmark, with Kendall’s W=0.36 (p<0.01), demonstrating moderate consensus. The mean value of the importance score of all aspect indicators ranged from
3.9 to 5.0 and the appropriateness score from 4.1 to 5.0
(Table 1).
Table 1: Importance and appropriateness score of the indicators.
|
Domain indicator |
Aspect indicator |
Importance |
Appropriateness |
||
|
X±s, score |
Cv |
X±s, score |
Cv |
||
|
?Hygiene literacy |
|
4.5±0.8 |
0.17 |
4.6±0.7 |
0.16 |
|
Eye health |
4.8±0.6 |
0.13 |
4.9±0.3 |
0.05 |
|
|
Oral health |
4.8±0.6 |
0.13 |
4.8±0.6 |
0.12 |
|
|
Hand health |
4.1±1.4 |
0.34 |
4.3±1.2 |
0.27 |
|
|
Sexual and reproductive hygiene |
4.9±0.3 |
0.06 |
5.0±0.0 |
0.00 |
|
|
Nutrition literacy |
|
4.8±0.8 |
0.17 |
4.6±0.8 |
0.18 |
|
Nutrition |
4.9±0.3 |
0.06 |
4.8±0.5 |
0.11 |
|
|
Food sanitation |
4.9±0.3 |
0.06 |
4.8±0.5 |
0.11 |
|
|
Physical activity literacy |
|
5.0±0.0 |
0.00 |
4.9±0.3 |
0.05 |
|
Exercise |
4.7±1.1 |
0.24 |
5.0±0.0 |
0.00 |
|
|
Sedentary behavior |
4.8±0.4 |
0.08 |
4.8±0.5 |
0.11 |
|
|
Sleep |
5.0±0.0 |
0.00 |
4.9±0.3 |
0.05 |
|
|
Preventive health literacy |
|
4.9±0.3 |
0.06 |
4.9±0.3 |
0.05 |
|
Nutrition-related disease |
4.5±0.8 |
0.17 |
4.5±0.8 |
0.17 |
|
|
Infectious disease |
4.9±0.3 |
0.06 |
4.9±0.3 |
0.06 |
|
|
Chronic disease |
3.9±1.5 |
0.38 |
4.1±1.3 |
0.32 |
|
|
Safety literacy |
|
4.8±0.4 |
0.08 |
5.0±0.0 |
0.00 |
|
Accidental injury prevention |
5.0±0.0 |
0.00 |
5.0±0.0 |
0.00 |
|
|
Natural disaster evacuation |
4.9±0.3 |
0.06 |
4.9±0.3 |
0.06 |
|
|
Psychosocial adaptation literacy |
|
5.0±0.0 |
0.00 |
4.9±0.3 |
0.05 |
|
Sociocultural adaptation |
5.0±0.0 |
0.00 |
5.0±0.0 |
0.00 |
|
|
Behavior regulation |
5.0±0.0 |
0.00 |
4.8±0.4 |
0·08 |
|
|
Psychological assistance |
4.8±0.6 |
0.13 |
4.5±0.8 |
0.17 |
|
|
Digital health literacy |
|
4.8±0.4 |
0.08 |
4.7±0.6 |
0.13 |
|
Access |
4.7±0.6 |
0.13 |
4.8±0.6 |
0.13 |
|
|
Evaluation |
4.5±1.2 |
0.27 |
4.6±0.8 |
0.17 |
|
|
Application |
4.5±1.2 |
0.27 |
4.5±0.8 |
0.17 |
|
Step 3: Item generation: We generated an item list via three brainstorming sessions which were merged with items brainstormed independently by an expert; sessions lasted from 2-4 hours each and were facilitated by the author Lili Y. All researchers and experts were either health education workers, and/or health promotion specialists. For each domain indicator, we aimed to generate a minimum of four items. This methodology is consistent with findings that at least three to four items per scale resulted in adequate internal consistency reliabilities [35].
Priorities in item generation included, (1) balanced representation across each subdomain of HL, (2) developmental appropriateness of items for children and adolescents, and (3) brevity to secure the feasibility to complete the scale responses; consensus was built via discussion.
Step 4: Questionnaire measurement: The constructed CRHLQ-PS consists of four sub-questionnaires, respectively tailored to grades1-2, grades3-4, grades 5-6 and junior high, named CRHLQ-12, CRHLQ-34, CRHLQ-56, and CRHLQ-junior. CRHLQ-12 contains 39 items, CRHLQ-34 contains 40 items, CRHLQ-56 contains 52 items and CRHLQ-junior contains 58 items. Question type differs among different grades (Table 2).
Table 2: Questionnaire measurement framework.
|
Sub-questionnaire |
Dimension |
Item number |
Item count |
Question type |
|
?Crhlq-12 |
Basic information |
A1-a11 |
11 |
Fill-in-the-blank; single-choice |
|
Knowledge |
B1-b11, c1, c3-c5, c10 |
16 |
Single-choice; judgement |
|
|
Skill |
B12, c2, c6-c8 |
5 |
Single-choice; judgement |
|
|
Motivation |
D1-d6 |
6 |
?3-point likert-type |
|
|
Participation |
C9, e1-e11 |
12 |
3-point likert-type |
|
|
Crhlq-34 |
Basic information |
A1-a11 |
11 |
Fill-in-the-blank; single-choice |
|
Knowledge |
B1-b10 |
10 |
Judgement |
|
|
Skill |
B11, c1-c7 |
8 |
Single-choice; judgement |
|
|
Motivation |
D1-d12 |
12 |
3-point likert-type |
|
|
Participation |
E1-e10 |
10 |
3-point likert-type |
|
|
Crhlq-56 |
Basic information |
A1-a11 |
11 |
Fill-in-the-blank; single-choice |
|
Knowledge |
B1-b14, c1, c2, c5 |
17 |
Judgement |
|
|
Skill |
C3, c4, c6-c16 |
13 |
Single-choice; judgement |
|
|
Motivation |
D1-d12 |
12 |
?5-point likert-type |
|
|
Participation |
E1-e10 |
10 |
5-point likert-type |
|
|
Crhlq-junior |
Basic information |
A1-a10 |
10 |
Fill-in-the-blank; single-choice |
|
Knowledge |
B1-b15, c1-c5 |
20 |
Judgement |
|
|
Skill |
C6-c15 |
10 |
Single-choice; judgement |
|
|
Motivation |
D1-d18 |
18 |
5-point likert-type |
|
|
Participation |
E1-e10 |
10 |
5-point likert-type |
Stage II: Validation of the CRHLQ-PS
In this phase, the developed questionnaire was administered to primary and secondary school students to test its validity and reliability.
Data collection
A multi-site validation study employing stratified sampling was conducted with 3,325 primary students and 2,788 secondary students across geographically distinct Chinese regions on the digital platform “Yiqixiu”. Standardized administration was supervised by trained teachers, with parental assistance protocols for lower grades students.
We obtained ethical approval from the Institutional Review Board of the Chinese Academy of Medical Sciences & Peking Union Medical College, which oversees research involving human participants. For participants, informed consent including a thorough explanation of the survey’s content and objectives was obtained from their parents to their involvement
Statistical analysis
For CRHLQ-junior, knowledge and skill dimensions composed of judgmental or multiple-choice questions underwent Rasch model analysis, while motivation and participation dimensions featuring scale-type questions were analyzed underwent CTT analysis. The CRHLQ-12, CRHLQ-34 and CRHLQ-56 were entirely validated through the Rasch model.
We Employed the Rasch model (Winsteps 3.72.3), to evaluate reliability and validity: reliability (>0.7) and separation indices (>2.0) confirmed measurement precision, unidimensionality was verified via principal component analysis of residuals (first contrast eigenvalue < 2.1), item fit was assessed through mean - square residuals (Infit/Outfit MNSQ: 0.5–1.5) and |ZSTD| < 2.0, the Wright map calibrated the alignment between item difficulty and person ability, model - data fit was evaluated via Infit/Outfit MNSQ (acceptable range [0.5, 1.5]), and point - measure correlations (range [0, 1], with larger values indicating better discriminative power) reflected the item - total score correlation, adhering to Rasch standards (Linacre, 2020). Meanwhile, within the CTT framework, construc validity was evaluated via exploratory factor analysis (EFA) with promax rotation (factor loadings > 0.4; cumulative variance ≥ 40%), concurrent validity was assessed using spearman’s correlation analysis, and internal consistency reliability was measured by cronbach’s α (> 0.55).
RESULTS
Sample characteristic
The survey included 1070 students in grades 1-2, with 792 in Luzhou, 116 in Taiyuan, 142 in Beijing, and 20 in
Zhengzhou; 1190 students in grades 3-4, with 962 in Luzhou, 78 in Taiyuan, 115 in Beijing, and 35 in Zhengzhou; 1065 students in grades 5-6, with 646 in Luzhou, 162 in Taiyuan, 218 in Beijing, and 39 in Zhengzhou; 2788 in junior high, with 1875 in Luzhou, 650 in Taiyuan, 263 in Beijing.
Reliability analysis
For CHLQ1-12, CHLQ1-34, CHLQ1-56, and judgmental/ multiple-choice questions of CRHLQ-junior, person ability values (2.84, 1.82, 1.99, 1.93) all exceeded the item difficulty value of 0. Reliability metrics-person reliability(0.59, 0.59, 0.73, 0.61) and item reliability (0.98, 1.00, 0.99, 1.00)-confirmed consistent and stable results. Separation indices revealed person separation values (1.19, 1.19, 1.63, 1.24; below the standard 2), indicating concentrated person ability levels, while item separation indices (6.39, 15.26, 10.86, 20.37; exceeding the ideal 2) underscored the questionnaire’s strong discriminative power and high item difficulty differentiation. Moreover, both INFIT MNSQ and OUTFIT MNSQ for items and persons approached the optimal value of 1, with INFIT ZSTD and OUTFIT ZSTD within [-2, 2], demonstrating favorable overall fit between observed data and the model (Table 3).
Table 3: Rasch model analysis results.
|
Sub-questionnaire |
Number |
Measure |
Infit |
Outfit |
Separation |
Reliability |
||
|
Mnsq |
Zstd |
Mnsq |
Zstd |
|||||
|
Crhlq-12 |
Person(n=1070) |
2.84 |
1.01 |
0.00 |
0.92 |
0.10 |
1.19 |
0.59 |
|
Item(n=39) |
0.00 |
1.00 |
0.20 |
0.95 |
-0.10 |
6.39 |
0.98 |
|
|
Crhlq-34 |
Person(n=1190) |
1.82 |
1.00 |
0.00 |
1.01 |
0.00 |
1.19 |
0.59 |
|
Item(n=40) |
0.00 |
1.01 |
0.40 |
1.02 |
0.20 |
15.26 |
1.00 |
|
|
Crhlq-56 |
Person(n=1065) |
1.99 |
1.00 |
0.00 |
0.95 |
0.00 |
1.63 |
0.73 |
|
Item(n=52) |
0.00 |
1.01 |
0.20 |
0.96 |
0.00 |
10.86 |
0.99 |
|
|
Crhlq-junior |
Person(n=2788) |
1.93 |
1.00 |
0.00 |
0.92 |
0.10 |
1.24 |
0.61 |
|
Item(n=30) |
0.00 |
0.98 |
0.10 |
0.92 |
-0.20 |
20.37 |
1.00 |
|
For scale-type question of CRHLQ-junior, the Cronbach’s α coefficients for the overall, motivation and participation dimensions were 0.818, 0.769, and 0.676, respectively.
Validity analysis
Unidimensionality: The Rasch model measurement explained 32.1% of the variance. The first residual factor, with a value of 2.4, accounted for 5.7% of the residual variance. These outcomes essentially satisfied the unidimensionality requirement, demonstrating that the
items measured the same domain.
Difficulty Analysis: For CRHLQ-12, item difficulty approximated a normal distribution (mean = 0 logit), and person ability estimates approximated a normal distribution spanning 6 logits (mean = 2.84 logit), higher than item difficulty. For CRHLQ-34, item difficulty was mostly distributed below 0 logit, person ability approximated a normal distribution (mean = 2.12 logit), higher than item difficulty. For CRHLQ-56, item difficulty approximated a normal distribution, (mean = 1.99 logit). The mean person ability exceeded the mean item difficulty by nearly 2.00 logit and no items corresponded to high- ability students (≥2.50 logit). For CRHLQ-junior, person ability demonstrated a normal distribution (mean = 2.12 logit) and items below -1 logit had no corresponding test- takers. All results showed that the overall difficulty of the questionnaire was set relatively low.
Spearman’s correlation analysis
The results showed that there were high correlations between the scores of the two dimensions of motivation and participation and the total score, with correlation factors of 0.771 and 0.835, respectively, and p-values of <0.001. The KMO values were 0.924 and 0.787, respectively, and the values of the Bartlett’s ball test were 22586.647 and 6668.652, respectively, with p-values of
<0.001. Motivation and participation applied principal component analysis to obtain the eigenvalue>1 of the common factor is 2, the cumulative variance contribution rate is 55.211%, 51.630%, respectively, the cumulative variance contribution rate of the common factor ≥40%; entries on the factor loadings are>0.4, the common factor variance is>0.3, and there is no multivariate loading, the structural validity is good.
DISCUSSION
Main finding of this study
HL Improvement can provide a competence base for health empowerment, and be good for individual health. In this study, we develop and validate a rapid comprehensive HL questionnaire, including four sub-questionnaires tailored to different academic levels.
This study offers new insights into the concept of children’s and adolescents’ HL from a developmental perspective.
In the process of questionnaire development, firstly, the numbers and contents of Items were strictly adherent to the indicators, with flexible adjustments. Secondly, different question expressions were used in each sub- questionnaire. Questionnaire targeting the relatively weak comprehension skills of students in the lower grades adopted a simplified format and dimension measures. In contrast, 5-point Likert-type scales was used for students in higher grades to gain a comprehensive understanding of their motivations for health behaviors. This differentiated approach effectively increased the sensitivity and accuracy of the questionnaires. Thirdly, pictorial displays were used to assist lower grade children in answering question.
We used the Rasch model for quality analysis, which unifying participant ability and questionnaire difficulty on a single measurement scale [29]. The results showed the questionnaire had a good internal consistency and can effectively differentiate between students of different levels. However, the average item difficulty was lower than the average ability, implying an overall simplicity. This simplicity may stem from the prevalence of easy-
to-answer judgement questions. Future studies should consider introducing more challenging types of questions, such as open-ended questions, or computational questions to increase difficulty.
What is already known on this topic
Previous research varies considerably on the definition and what constitutes HL has been consistently contested within the literature [36]. Recently, karolina developed the first child and adolescent-centered health literacy model [37]. As such, HL model in children and adolescents is deserving of direct attention. Conceptualizing HL can serve as a solution to recognize empowerment that extends beyond the acquisition of basic health knowledge.
This study constructs a robust HL indicator system for primary and secondary school students containing seven domain indicators. To our knowledge, this is the first study to build a dynamically evolving assessment framework for primary and secondary school students. European and American systems have adapted assessment tools like s-TOFHLA [18], REALM-teen [38], and HLS-EU-Q47 [39], to achieve adaptation for children and adolescents. s-TOFHLA REALM-teen focus on text comprehension and health decision-making skills in medical scenarios, while HLS- EU-Q47 cover three major domains of health promotion, disease prevention, and healthcare, and emphasizing cross-cultural adaptation and the effectiveness of policy interventions. Besides, the WHO GAMA framework’s 47 adolescent health indicators [40], cover health behaviors, social determinants, and system performance. However, the focus of GAMA is more on policy and system-level assessments rather than on specific measurement tools.
What this study adds Limitations of this study
In the survey, we relied on voluntary responses from students. Considering the age and level of cognitive development of the students, the results may contain biases inherent in the students. In condition, our participants were selected through cluster sampling, which may result in an underrepresented population. However, it is worth noting that this limitation is less important due to the fact that Rasch analysis is less dependent on sample characteristics than classical measurement theory.
In conclusion, The CHLIS-PS we constructed, validated through literature based, policy alignment and expert consensus, demonstrates robust and comprehensiveness. The CRHLQ-PS is expected to comprehensively measure the HL of students aged 6 to 15 years, filling the gap in related research areas. In the future, we hope to have some cross-country comparative studies to further validate the applicability of the CRHLQ-PS, and it may become a key tool to promote global adolescent health literacy.
FUNDING
This work was supported by the Science and Technology Innovation Project in Medicine and Health, Chinese Academy of Medical Sciences under Grant [number 2021- I2M-1-046]; the National Natural Science Foundation of China under Grant [number 71904205].
ACKNOWLEDGEMENT
We acknowledge participating primary and secondary schools in Luzhou, Taiyuan, Beijing, and Zhengzhou for facilitating student recruitment and data collection. Special thanks are due to the multidisciplinary experts who contributed their insights through Delphi consultations and interviews. This study was approved by the Institutional Review Board of the Chinese Academy of Medical Sciences & Peking Union Medical College, and we thank the committee for their ethical oversight. Finally, we recognize the funding support from the Science and Technology Innovation Project in Medicine and Health, Chinese Academy of Medical Sciences (2021-I2M-1-046) and the National Natural Science Foundation of China (71904205). The authors alone are responsible for the content and writing of this paper.
REFERENCES
- Liu C, Wang D, Liu C, Jiang J, Wang X, Chen H, et al. What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam Med Com Health. 2020; 8: e000351.
- Sørensen K, Van Den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health. 2012; 12: 80.
- Santana S, Brach C, Harris L, Ochiai E, Blakey C, Bevington F, et al. Updating Health Literacy for Healthy People 2030: Defining Its Importance for a New Decade in Public Health. J Public Health Management and Practice. 2021; 27(Supplement 6): S258-S264.
- Fleary SA, Joseph P, Pappagianopoulos JE. Adolescent health literacy and health behaviors: A systematic review. J Adolesc. 2018; 62: 116- 127.
- Joseph P, Fleary SA. “The Way you Interpret Health”: Adolescent Definitions and Perceptions of Health Literacy. J Sch Health. 2021; 91: 599-607.
- Massey PM, Prelip M, Calimlim BM, Quiter ES, Glik DC. Contextualizing an expanded definition of health literacy among adolescents in the health care setting. Health Educ Res. 2012; 27: 961-974.
- World Health Organization. Shanghai declaration on promoting health in the 2030 Agenda for Sustainable Development. Health Promot Int. 2017; 32: 7-8.
- Kelly RK, Nash R. Food Literacy Interventions in Elementary Schools: A Systematic Scoping Review. J Sch Health. 2021; 91: 660-669.
- Truman E, Lane D, Elliott C. Defining food literacy: A scoping review.Appetite. 2017; 116: 365-371.
- Edwards LC, Bryant AS, Keegan RJ, Morgan K, Jones AM. Definitions, Foundations and Associations of Physical Literacy: A Systematic Review. Sports Med. 2017; 47: 113-126.
- Clark LH, Hudson JL, Rapee RM, Grasby KL. Investigating the impact of masculinity on the relationship between anxiety specific mental health literacy and mental health help-seeking in adolescent males. J Anxiety Disord. 2020; 76: 102292.
- Bhagat K, Howard DE, Aldoory L. The Relationship Between Health Literacy and Health Conceptualizations:An Exploratory Study of Elementary School-Aged Children. Health Commun. 2018; 33: 131-138.
- Van Boxtel W, Jerkovi?-?osi? K, Schoonmade LJ, Chinapaw MJM. Health literacy in the context of child health promotion: a scoping review of conceptualizations and descriptions. BMC Public Health. 2024; 24: 808.
- Spillane A, Belton S, McDermott C, Issartel J, Osborne RH, Elmer S, et al. Development and validity testing of the Adolescent Health Literacy Questionnaire (AHLQ): Protocol for a mixed methods study within the Irish school setting. BMJ Open. 2020; 10: e039920.
- Haun JN, Valerio MA, McCormack LA, Sørensen K, Paasche-Orlow MK. Health literacy measurement: an inventory and descriptive summary of 51 instruments. J Health Commun. 2014; 19: 302-333.
- Hawkins M, Elsworth GR, Osborne RH. Application of validity theory and methodology to patient-reported outcome measures (PROMs): building an argument for validity. Qual Life Res. 2018; 27: 1695-1710.
- Caldwell EP, Killingsworth EE. The Online Use of the Newest Vital Sign in Adolescents. Clin Nurs Res. 2022; 31: 55-59.
- Chang LC, Hsieh PL, Liu CH. Psychometric evaluation of the Chinese version of short-form Test of Functional Health Literacy in Adolescents. J Clin Nurs. 2012; 21: 2429-2437.
- Chou AK, Liao CH, Chen DR. Measuring adolescent health literacy in Taiwan: validation of the health literacy assessment scale for adolescents. BMC Public Health. 2023; 23: 2409.
- Arias López MDP, Ong BA, Borrat Frigola X, Fernandez AL, Hicklent RS, Obeles AJT, et al. Digital literacy as a new determinant of health: A scoping review. PLOS Digit Health. 2023; 2: e0000279.
- Ban S, Kim Y, Seomun G. Digital health literacy: A concept analysis. Digit Health. 2024; 10: 20552076241287894.
- Bröder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM, et al. Health literacy in childhood and youth: a systematic review of definitions and models. BMC Public Health. 2017; 17: 361.
- Guo S, Armstrong R, Waters E, Sathish T, Alif SM, Browne GR, et al. Quality of health literacy instruments used in children and adolescents: a systematic review. BMJ Open. 2018; 8: e020080.
- Okan O, Pinheiro P, Zamora P, Bauer U. [Health literacy in childhood and adolescence: An overview and current state of research]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2015; 58: 930-941.
- Ormshaw MJ, Paakkari LT, Kannas LK. Measuring child and adolescent health literacy: a systematic review of literature. Health Education. 2013; 113: 433-455.
- Fretian A, Bollweg TM, Okan O, Pinheiro P, Bauer U. ExploringAssociated Factors of Subjective Health Literacy in School-Aged Children. Int J Environ Res Public Health. 2020; 17: 1720.
- Urstad KH, Andersen MH, Larsen MH, Borge CR, Helseth S, Wahl AK. Definitions and measurement of health literacy in health and medicine research: a systematic review. BMJ Open. 2022; 12: e056294.
- Mansfield R, Patalay P, Humphrey N. A systematic literature review of existing conceptualisation and measurement of mental health literacy in adolescent research: current challenges and inconsistencies. BMC Public Health. 2020; 20: 607.
- Jabrayilov R, Emons WHM, Sijtsma K. Comparison of Classical Test Theory and Item Response Theory in Individual Change Assessment. Appl Psychol Meas. 2016; 40: 559-572.
- Woudstra AJ, Meppelink CS, Pander Maat H, Oosterhaven J, Fransen MP, Dima AL. Validation of the short assessment of health literacy (SAHL-D) and short-form development: Rasch analysis. BMC Med Res Methodol. 2019; 19: 122.
- National Health Commission (2008). National Health Commission of the People’s Republic of China. Chinese Resident Health Literacy- Basic Knowledge and Skills (Trial). Beijing. 2025.
- The State Council of the People’s Republic of China (2016). The State Council of the People’s Republic of China. Health China 2030. Beijing. 2025. Accessed March 20, 2025.
- Bale J, Grové C, Costello S. A narrative literature review of child- focused mental health literacy attributes and scales. Mental Health & Prevention. 2018; 12: 26-35.
- Holey EA, Feeley JL, Dixon J, Whittaker VJ. An exploration of the use of simple statistics to measure consensus and stability in Delphi studies. BMC Med Res Methodol. 2007; 7: 52.
- Harvey RJ, Billings RS, Nilan KJ. Confirmatory Factor Analysis of the Job Diagnostic Survey. Good News and Bad News. J Appl Psychol. 1985; 70: 461-468.
- Bröder J, Okan O, Bollweg TM, Bruland D, Pinheiro P, Bauer U. Child and Youth Health Literacy: A Conceptual Analysis and Proposed Target-Group-Centred Definition. Int J Environ Res Public Health. 2019; 16: 3417.
- Seidl K, Stauch L, Affengruber L, Sommer I, Wahl A, Rojatz D, et al. Conceptualization of health literacy from the perspective of children and adolescents - a meta-ethnography. Sci Rep. 2025; 15: 5697.
- Davis TC, Wolf MS, Arnold CL. Development and validation of the Rapid Estimate of Adolescent Literacy in Medicine (REALM-Teen): a tool to screen adolescents for below-grade reading in health care settings. Pediatrics. 2006; 118: e1707-1714.
- Domanska OM, Firnges C, Bollweg TM, Sørensen K, Holmberg C, Jordan S. Do adolescents understand the items of the European Health Literacy Survey Questionnaire (HLS-EU-Q47) : German version? Findings from cognitive interviews of the project “Measurement of Health Literacy Among Adolescents” (MOHLAA) in Germany. Arch Public Health. 2018; 76: 46.
- World Health Organization. The adolescent health indicators recommended by the Global Action for Measurement of Adolescent health. 2024.1904205). The authors alone are responsible for the content and writing of this paper.









































































































































{kind=link}