Double Vision after Blunt Trauma: A Case of Acquired Brown Syndrome
- 1. Department of Ophthalmology and Visual Sciences, Case Western Reserve University and University Hospitals Rainbow Babies and Children’s Hospital, USA
ABSTRACT
Brown syndrome is a special form of strabismus characterized by limited elevation of the eye in adduction resulting from an abnormality of the superonasal aspect of the orbit. The etiology may be congenital, inflammatory, or traumatic, and treatment approaches can vary. We report a case of Brown syndrome causing diplopia in a child after trauma to the lateral side of the face but with an unclear mechanism of injury to the superonasal orbit.
CITATION
Boente CS, Orge FH (2014) Double Vision after Blunt Trauma: A Case of Acquired Brown Syndrome. Ann Pediatr Child Health 2(4): 1028.
KEYWORDS
Diplopia, Orbital trauma, Brown syndrome, Superior blique muscle, Trochlea
INTRODUCTION
Trauma to the eye and surrounding structures can present in a variety of ways, requiring careful assessment to rule out trauma-related injuries such as traumatic iritis, orbital bone fractures, or ruptured globe. Orbital bone fractures are not uncommon in children sustaining severe blunt trauma injuries around the eye and can be confirmed with a CT scan of the orbits. Because of the possibility of extraocular muscle entrapment and incarceration within clefts of orbital bone fractures, a careful ocular motility exam is required to determine if surgical intervention is needed to release incarcerated tissue and/or to repair the fracture. In our case, we describe a child presenting with a special form of strabismus, called Brown syndrome, after blunt trauma.
Brown syndrome is defined as limited elevation of the eye in adduction, originally described intra operatively by Harold Whaley Brown in 1950 as a “short tendon sheath of the superior oblique tendon that restricts passive movements of elevation in the nasal field”. Other features of Brown syndrome include normal or near normal elevation in abduction and positive forced duction testing revealing mechanical restriction when attempting to elevate the eye in adduction [1]. Since Brown’s original observations, others have attributed the motility limitations to include a variety of abnormalities not only to the tendon sheath, but also to other sensitive structures in the superonasal aspect of the orbit, such as the superior oblique muscle, tendon, and/or trochlea complex. These abnormalities have included a congenital tight tendon, impaired slippage of tendon through the trochlea due to a mass or trauma, or other inflammatory conditions (e.g. rheumatoid arthritis, sinusitis) causing thickening of the retrotrochlear tendon, trochlea, or superior oblique muscle itself [2]. Our patient exhibited the typical features of Brown syndrome, but with an unclear mechanism, as no direct trauma to the superonasal aspect of the orbit was confirmed on physical exam, radiology, or surgical exploration.
CASE PRESENTATION
A 7 year old boy with no known past ocular history initially presented to an orbital specialist at the University Hospitals Eye Institute after sustaining trauma to the right face during a sledding accident resulting in contusion with 12mm x 2mm ecchymosis to the lateral side of the right face. On exam, visual acuity without correction was 20/15 in the right eye, 20/15 in the left eye, and he exhibited moderate right eye ocular motility restriction in upgaze with adduction and associated double vision. CT scan of the orbits was obtained and reviewed with the radiologist revealed mild, chronic inflammatory changes to bilateral maxillary sinuses, questionable entrapment of tissue in a small cleft of the right orbital floor, as well as possible thickening of the right trochlea (Figure 1).

Figure 1: CT scan of the orbits with showing (a) possible soft tissue entrapment in cleft of orbital floor and (b) enlargement of right trochlea.
There was no evidence of direct trauma to the right trochlea, nor was there obvious evidence of significant muscle entrapment explaining the degree of restriction. The patient was initially observed for two weeks on oral prednisone 20 mg (1mg/kg), but since his symptoms of diplopia persisted, it was agreed that surgical orbital exploration was indicated.
Intraoperatively, forced movements of the eye by the surgeon revealed tightness and restriction when moving the right eye upward in adduction. With further exploration and periosteal dissection, no entrapment was evident at the cleft initially identified as suspicious on the CT scan, but did reveal a thin 0.5mm wide fracture running anterior-posterior reaching almost to the pterygopalatine fossa just at the junction of the medial orbital wall and floor. With minimal traction, a small amount of soft tissue was noted to free up from the fracture site. Notably, further exploration revealed no abnormalities to the superonasal aspect of the globe and orbit. The patient was continued on oral prednisone 20 mg (1mg/kg) daily for an additional 10 day course as well as oral cefelaxin for a 7 day total course.
At both his one and two week post-op visits, the patient continued to exhibit restriction in up gaze with adduction of the right eye (Figure 2), and associated diplopia.
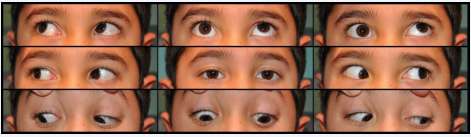
Figure 2: One month after blunt trauma to lateral side of right face, and two weeks after right orbitotomy and exploration.
The patient was managed conservatively with observation, although further exploration with MRI to identify possible injury to fourth cranial nerve and/or additional surgery was discussed. At our patient’s three month post-op visit, he showed significant improvement in his ocular motility (Figure 3) and at six months post-op, he showed complete resolution (Figure 4) without any additional intervention.
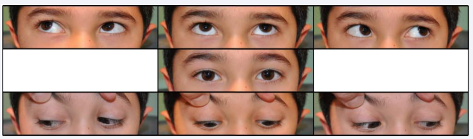
Figure 3: Three months after injury.
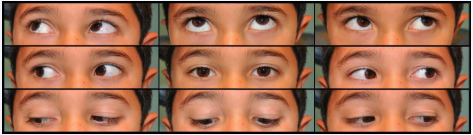
Figure 4: Six months after surgery.
DISCUSSION
The presentation of Brown syndrome has been well characterized, but the cause and disease course may vary. Our patient demonstrated many of the constant and variable features of Brown syndrome, including deficient elevation in adduction, normal elevation in abduction, restriction of elevation in adduction on forced ductions, limitation of elevation from primary position, downshoot on adduction, and widening of lid fissure on adduction [2] (Figure 2). The atypical feature of our case is the absence of obvious or direct superior oblique tendon or trochlea abnormalities, by history, exam, radiology, and surgical exploration. Even after the release of soft tissue incarceration at the junction of the medial wall and orbital floor, the patient continued to exhibit the classic features of Brown syndrome. Furthermore, with tissue incarceration inferonasally, one would expect to see abduction restriction patterns, in addition to the adduction motility limitations seen in our patient. Therefore, although the mechanism of injury was not obvious to the cause of his diplopia, the strabismus pattern on ocular motility exam localized the issue to the superonasal aspect of the orbit.
CT has been shown superior in evaluating the superior oblique muscle and trochlea complex particularly in acquired Brown syndrome, which can show thickening of the tendon in known inflammatory conditions or direct trauma to the trochlear region [4]. In our patient, there was only questionable thickening of tissue around the right trochlea without any signs of external trauma directly extending to the site. The mechanism of injury opposite to the side of impact is unclear, but there is reason to believe that inflammation, edema, and swelling of the connective tissue surrounding the superior oblique tendon within the trochlea resulted in this child’s presentation of Brown syndrome. As described by Helveston, the intra-trochlear portion of the superior oblique tendon is highly vascularized, supporting the possibility of vascular dilation and local edema from blunt trauma injuries causing restriction of the tendon through the trochlear tunnel, resulting in a Brown syndrome [3]. Wright suggests the use of the term acquiredpseudo-Brown syndrome for cases without any superior oblique pathology, such as in our patient [1].
Although a variety of surgical techniques to the superior oblique muscle have been used to manage congenital and acquired Brown syndrome, many would favor observation in the absence of primary position ocular misalignment or abnormal head positioning [5]. In one study, Dawson found spontaneous resolution of constant Brown syndrome in 75% of patients aged 1-14, with follow up ranging from 6 months to 9.5 years after the initial visit, suggesting a preferred observational approach [6]. In our patient, improvement began to occur about 3 months after onset, with complete resolution noted 6 months after onset. Identifying the strabismus pattern as Brown syndrome was imperative to avoid potentially unnecessary surgical intervention of extraocular muscles to correct this child’s diplopia. In cases of acquired Brown syndrome after known trauma without direct injury to the trochlear region, an inflammatory process to the region should be highly considered and managed by observation alone with or without systemic steroids.









































































































































{kind=link}