Report of a Rare Case of Congenital Laryngocele associated with Thyroglossal Cyst as a Differential Diagnosis of Congenital Stridor
- 1. Associate professor of Goiás Federal University (UFG), Brazil
- 2. Postgraduate of Goiás Federal University (UFG), Brazil
- 3. Medical student of Goiás Federal University (UFG), Brazil
Abstract
A congenital laryngocele is an abnormal dilation of the saccule of the ventricle of Morgagni, located between the false vocal fold and the inner surface of the thyroid cartilage. We present a rare case of congenital stridor in a full-term newborn, diagnosed as a congenital laryngocele associated with a thyroglossal cyst. While the most common diagnosis for congenital stridor is laryngomalacia, detailed physical examination is essential for the correct diagnosis. To our knowledge, the association of congenital laryngocele with a thyroglossal cyst has not been previously reported in the literature.
Keywords
• Congenital laryngocele
• Cervical swelling
• Upper airway obstruction
• Thyroglossal cyst
• Congenital stridor
Citation
Ferri L, de Deus MM, de Paula Reis R, Duarte TAL, Avelino MAG (2025) Report of a Rare Case of Congenital Laryngocele associated with Thyroglossal Cyst as a Differential Diagnosis of Congenital Stridor. Pediatr Child Health 13(1): 1346.
INTRODUCTION
Congenital laryngoceles are abnormal dilations of the saccule of the ventricle of Morgagni, situated between the false vocal fold and the proximal edge of the thyroid cartilage. These lesions contain air that communicates with the laryngeal lumen and may become distended by mucus. Congenital laryngoceles are extremely rare, with an estimated incidence of 1 in 2.5 million people per year [1]. Although benign, they can present congenitally or be acquired later in life. In newborns, they may cause symptoms such as stridor, respiratory difficulty, and severe airway obstruction, requiring urgent intervention [2].
When diagnosing congenital stridor in newborns, it is essential to consider differential diagnoses, particularly laryngomalacia, congenital subglottic stenosis, vocal cord paralysis, vallecular cyst, tracheal duplication, ductus arteriosus aneurysm, subglottic cyst or hemangioma, as well as tracheal and laryngeal agenesis [3-6].
Stridor is a primary symptom of laryngeal and/ or tracheal obstruction, and flexible endoscopy (nasofibroscopy) is essential for confirming this diagnosis and ruling out other potential causes. In cases of congenital stridor, even when symptoms strongly suggest laryngomalacia, which is the most common cause, flexible endoscopy should be conducted to verify the presence of laryngeal abnormalities [7,8].
This article aims to present a rare case of congenital stridor, where the diagnosis revealed a congenital laryngocele associated with a thyroglossal cyst.
CASE REPORT
A full-term newborn presenting with inspiratory stridor at birth, respiratory distress following retraction of the furcula, and a requirement for supplemental oxygen was referred to the Neonatal Intensive Care Unit (Neo-ICU) after initial care in the delivery room. Due to the presence of stridor, the referring hospital suspected laryngomalacia, documented the findings, and requested a transfer to the Neo-ICU at Goiânia Children’s Hospital. On the fifth day of life, the child arrived in our Hospital and in addition to the stridor, the newborn had a palpable cervical bulge in area IV on the right side, measuring approximately 2 x 2 cm. The bulge was mobile, with no signs of inflammation or skin fluctuation (Figure A).
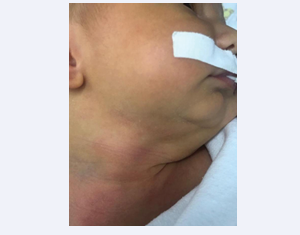
Figure A : The bulge in the right laryngeal region
He underwent endoscopy and suspension laryngoscopy under spontaneous ventilation and during the procedure, submucosal supraglottic bulging was observed in the right false vocal fold, while the subglottic region and trachea were within normal limits. This bulge compromised the lumen, making it difficult to assess the mobility of the right vocal fold (Figure B).

Figure B: Endoscopic image showing supraglottic bulging in the right false vocal fold.
In light of this endoscopic finding, along with the presence of the cervical bulge, we proceeded with an imaging examination to further assist in the diagnosis.
Computed tomography of the neck revealed two cervical lesions: a larger lateral lesion with a cystic component filled with air, suggestive of a congenital laryngocele, and a smaller lesion located on the midline, indicative of a separate cyst (Figure C).
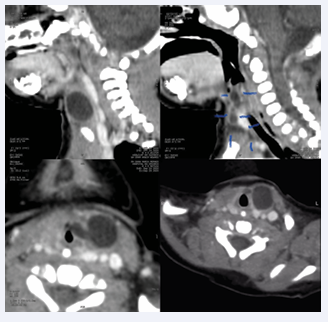
Figure C.1–C.4: Tomographic images displaying the Congenital Laryngocele and Thyroglossal Cyst in lower density images (in dark gray, according to the Hounsfield scale).
To address the issue, external cervical access (Figure D),
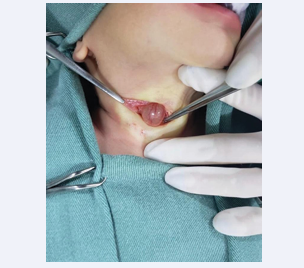
Figure D: Depiction of the open access in the anterior cervical region showing the excision of the lateral cystic lesion confirmed histopathologically as a laryngocele.
was chosen for the surgical resection of the cervical cystic lesions.
Intraoperatively, another cystic lesion was identified, which was continuous with the hyoid bone, raising the possibility of a thyroglossal duct cyst that had not been detected during the physical examination, only on CT scan. The histopathological results confirmed the presence of a congenital laryngocele and the additional smaller cystic lesion confirmed the diagnosis of a thyroglossal duct cyst. A follow-up endoscopy was performed after 48 hours to confirm the restoration of the laryngeal lumen. The child had an uneventful postoperative course, with complete resolution of symptoms and discharge from the ICU within 48 hours of the operation.
DISCUSSION
The correct diagnosis of a congenital stridor may be a challenge. Most reports of congenital stridor in the literature are related to the presence of laryngomalacia, as it is the most common congenital laryngeal condition [8]. Our case is a rare case of congenital laryngocele associated with a thyroglossal cyst. The cervical bulging observed during this patient’s physical examination was crucial in raising suspicion to other congenital abnormalities that would support a different diagnosis from laryngomalacia. The presence of stridor requires diagnosis with a flexible endoscopy; however, an accurate diagnosis may require a rigid laryngotracheobronchoscopy and suspension laryngoscopy [2]. To confirm the diagnosis of laryngocele, suspension laryngoscopy and imaging tests are performed. The hypothesis of a thyroglossal duct cyst was considered only intraoperatively, due to the cystic lesion’s midline location and its contact with the hyoid bone, but the diagnosis was confirmed with histopathological results.
Congenital laryngocele is rarely reported in the literature, with the majority of cases being acquired rather than congenital. Acquired laryngoceles are associated with factors and conditions such as chronic cough, laryngeal carcinoma, and the use of wind instruments. They are more prevalent in men, with a ratio of 5:1 [5]. Their occurrence is due to the weakening of the aryepiglottic and thyroepiglottic muscles and the periventricular connective tissues.
Since congenital laryngoceles are formed during the embryonic period, they result from the saccule developing beyond normal limits in utero [2]. A total of twenty cases of congenital laryngocele have been found in the literature, none of which discussed the presence of an associated thyroglossal duct cyst.
In addition to clinical history and physical examination, direct laryngoscopy is required to confirm the diagnostic hypothesis of a laryngocele [2]. The use of computed tomography or magnetic resonance imaging is important to determine the exact delineation of the structures involved in the pathology, and thus it is an important tool in selecting an intervention plan [4].
It is important to emphasize that what distinguishes this case from others presented in the literature is the manifestation of congenital laryngocele associated with the presence of a thyroglossal duct cyst, which was only confirmed intraoperatively, as the child did not present any abnormal findings in the cervical midline during the physical examination. The thyroglossal duct cyst is generally diagnosed in school-aged children after the onset of upper respiratory infections, presenting as a cervical midline bulge associated with inflammatory signs and sometimes with cervical infection. The occurrence of this association between congenital laryngocele and thyroglossal duct cyst has not yet been reported in the available literature.
Although the presence of a thyroglossal duct cyst is relatively common compared to the appearance of a congenital laryngocele, the fact that this presentation was found concomitantly raises the question of a possible embryological association between these two malformations. The existence of this unique case in the literature opens doors to better understanding the unknown mechanisms related to the formation and appearance of these malformations during the embryonic period. Nevertheless, there is the possibility that this correlation is mere coincidence.
It is noteworthy that the presence of respiratory symptoms, such as stridor, is an important marker of severity since airway obstruction in neonates poses a risk to the patient’s life [3].
Therefore, in clinical practice, it is important to consider the differential diagnosis of congenital stridor, in addition to laryngomalacia, to ensure that medical interventions achieve the desired results with the least possible harm to the patient.
CONCLUSION
This is a rare case of congenital laryngocele with an associated thyroglossal cyst, where the initial diagnosis was laryngomalacia despite the presence of cervical bulging. Thus, we emphasize the importance of thorough clinical examination, including endoscopy and suspension laryngoscopy, for accurate diagnostic confirmation.
REFERENCES
- Y?lmaz S, Y?ld?zba? ?, Yaman H, Güçlü E, Öztürk Ö. Stridor in a newborn caused by a congenital laryngocele and bifid epiglottis: a case report and review of literature international. J Pediatric Otorhinolaryngol Extra. 2010; 5: 28-31
- Tasinklar H, Vayisoglu Y, Avlan D, Polat A, Nayci A. Congenital Laryngomucocele: a rare cause of airway obstruction in a newborn. J Craniofac Surg. 2015; 26: e238-e240.
- Ahmed H, Ndiaye C, Barry MW, Thiongane A, Mbaye A, Zemene Y, et al. A Rare Cause of Upper Airway Obstruction in a Child. Case Rep Otolaryngol. 2017; 1-3.
- Andrea A, Balázs S, Miklós S, Béla V, István S, László R. An unusual cause of infant’s stridor – congenital laryngocele. J Otolaryngol Head Neck Surg. 2020; 49.
- Felix JA, Felix F, Mello LFP. Laringocele: uma causa de obstrução de vias aéreas superiores. Revista Brasileira de Otorrinolaringologia. 2008; 74:143-146.
- Rangel AC, Pegorer LF, Vilela R. Stridor in the delivery room. Revista Paulista de Pediatria. 2010; 28: 409-412.
- Cassol VE. Endoscopic diagnosis of stridor in childhood. J de Pneumologia. 2001; 27.
- Bedwell J, Zalzal G. Laryngomalacia. Sem Pediatric Surg. 2016; 25: 119-122.









































































































































{kind=link}