Cerebral Micro Arteriovenous Malformations (mAVMs) - Endovascular Treatment in 3 Cases and Review
- 1. Department of Neurointervention, CINN-Centro Integrado de Neurologia e Neurocirurgia, Brazil
- 2. Parana Hospital, Maringá, Brazil
Abstract
Object: Microarteriovenous malformations (micro-AVMs) defined by Yasargil, represent a subgroup of cerebral AVMs with a nidus diameter <1cm and corresponding to 7% of all cerebral AVMs and 21% of AVMs after hemorrhage. Hemodynamic and structural factors can predispose bleeding, the small size and flow characteristics prevent presentation with usual symptoms as seizures. The authors’ present 3 cases with endovascular treatment and a literature review.
Methods: In a review since 2011, we found three patients (two males and one female) with micro AVMS. Two had intraparenchymal hematoma and initial DSA was negative. A third patient had epilepsy and daily seizures with unruptured left temporal micro AVM. In the literature review the key words used were: “micro arteriovenous malformation”, “arterio venous malformation”, “occult arteriovenous malformation” and “embolization”.
Results: In all cases micro AVM was confirmed diagnosis with a DSA, 3D reconstruction DSA and superlective DSA. All underwent embolization with embolic liquid EVOH (SQUID 18®) and total occlusion and no procedures complications. All had good clinical mRS 0 in long term follow up and no recanalization in angiography FU.
Conclusion: Patients with micro-AVMs generally present with large intracranial hemorrhages and neurological deficits. An initial angiography may be negative in suggestive cases, then delayed or superselective angiography and 3D DSA is recommended. Surgery is the treatment of choice for large volume hematomas. Embolization may be a safe alternative and should be considered as an alternative to surgical resection.
Keywords
Micro arteriovenous malformation; Arterio venous malformation; Occult arteriovenous malformation; Embolization
Citation
De Andrade GC, Leszczynski A, Pereira ER (2020) Cerebral Micro Arteriovenous Malformations (mAVMs) - Endovascular Treatment in 3 Cases and Review. Ann Vasc Med Res 7(2): 1107.
ABBREVIATION
AVM: Arteriovenous Malformation; DSA: Digital Subtraction Angiography; AS: Superselective Angiography; MRI: Magnetic Resonance Imaging; CT: Computed Tomography; ICH: Intracerebral Hematoma; NBCA: N-butyl-cyanoacrylate; EVOH: Ethylene Vinyl Alcohol; PVA: Polyvinyl Alcohol; mRS: modified Rankin Scale
INTRODUCTION
Micro-AVMs are a rare entity, accounting for about 7-8% of all cerebral AVMs in surgical series, but they are usually a source of clinically relevant cerebral hemorrhage in young adults [1,2]. This kind of micro AVM had small nidus or fistula and a single normalized feeding artery and draining vein. The literature and pathological classifications are confusing with regard to the so-called occult (unrevealed) and cryptic (hidden) vascular malformations, but were originally defined with a nidus less than a centimeter in size by Ya?argil [1]. They are rare lesions comprising 7% of all cerebral AVMs and 21% of AVMs diagnosed following hemorrhagic presentation and their predominant presenting sign of micro-AVMs is intracranial hemorrhage [3]. By definition micro-AVMs are visible at angiography, sometimes just as an abnormal arteriole without draining veins or as an abnormal draining vein with the feeding vessels remaining undetectable in other times a tiny lesion with the classic appearance of pathological arterioles and pathological draining veins is visible on angiography. Micro AVM can be treated with surgery, radiosurgery or embolization. Embolization has been proposed as a minimally invasive and effective alternative.
MATERIAL AND METHODS
We identified 3 patients (2 females and 1 male) with average age of 40.6yrs that had a micro-AVM and constitute the present series. Two patients had intraparenchymal hematoma and initial DSA was negative. A second DSA study was scheduled after hematoma resorption. In one of them a second DSA found a left frontal micro AVM. In the other one, follow up was made with MRI and Angio MRI for three years always negative. In this case, a second opinion with us, performed an angiography with 3D reconstruction DSA and a right temporal micro AVM was found. A third case with diagnosis of epilepsy and daily seizures refractory to multiple drug treatment, had a left micro AVM diagnosed by MRI and angiography, had follow up by neurology and neurosurgery for 10 years and no indication for surgical, endovascular or radiosurgical treatment. In a second opnion with us, there was endovascular treatment with total occlusion and better seizures control. All cases were supratentorial. The identification of a small feeding vessel with a poorly defined, tiny nidus and an early draining vein was the finding on angiography. In one patient, a focal neurological deficit was present at the initial diagnosis (Figure 1). None of the patients had a family history or findings indicative of Osler-Rendu-Weber disease. Definitive treatment for the AVM was endovascular embolization in all cases (Figure 1-3). None of the patients demonstrated new neurological deficits after treatment. Embolization with EVOH (SQUID 18®) (Balt Extrusion, Montmorency, France) cured all patients. The treatment did not add morbidity in any of our patients. The mRS was excelent in all cases. The long term angiography follow up (12 months) was performed in all cases.
RESULTS
In all cases micro AVM was confirmed diagnosis with a DSA, 3D reconstruction DSA and superlective DSA. All underwent endovascular treatment with superlective microcatheterization technique of the feeder of the nidus and total occlusion with embolic liquid EVOH (SQUID 18®) and no procedures complications. The long term angiography follow up (12 months) was negative to recanalization of micro AVMs. All cases had clinical mRS 0 in follow up. In the first case there was neurological deficit recovery after left parietal hematoma resorption. In the case with epilepsy and daily seizures, there was better seizures control after micro AVM occlusion.
Endovascular Treatment
The same neuroradiologist (GCA) performed the embolization and informed consent was obtained from each patient before the procedure. In all patients the embolization was performed under general anesthesia and a transarterial transfemoral route was performed using a long sheath 6-Fr access with loading bolus of 5000 IU heparin followed by an infusion of 1000 IU/h was administered. A triaxial system as a 6F guiding catheter Fargo Max (Balt Extrusion, Montmorency, France) was placed into the distal internal carotid artery and a microcatheter SONIC 1.2F (Balt Extrusion, Montmorency, France) primed with a 0.08-inch guidewire Hybrid (Balt Extrusion, Montmorency, France) was subsequently advanced proximal to the nidus. A superselective angiography was performed before embolization. A single shot embolization with embolic liquid (SQUID 18® - Balt Extrusion, Montmorency, France) was delivered via a microcatheter that was wedged in the nidus or placed in the terminal arterial feeder just proximal to the nidus (Figure 1B,2C,3E). All patients underwent immediate angiographic post treatment studies and also performed after 12 months follow up. A total occlusion was achieved in all cases.
Procedural Complications
We didn´t have any kind of complications in this series.
Immediate Postembolization Angiography Results
Complete nidus obliteration was achieved at the end of the embolization in all cases (100%), with complete penetration of the EVOH (SQUID 18®).
Angiographic Follow-Up
All patients had a follow-up angiogram 12 months post embolization and DSA with total occlusion of the all micro AVMs.
Clinical Outcome
The clinical follow-up period ranged from 6 to 36 months. All patients experienced improvements after the endovascular treatment and total occlusion of their AVMs. No permanent neurological deficits related to the procedure were evident. All patients had 0 mRS (modified Rankin Scale). In the first patient that had intraparenchymal hematoma on the left frontal cortex with sudden right hemiparesis, there was an improvement in his deficit maintaining only deficit in the dorsiflexion of the right foot and no seizures in his evolution. In the second case there was history of right temporal intraparenchymal hematoma and seizures every 6 months and after embolization there was not recurrent seizures. In the last case that had the diagnosis of the left posterior temporal micro AVM and seizures daily refractory to multidrug treatment, after endovascular occlusion there was 50% reduction in seizure frequency.
Literature Review
Eight publications of micro AVMs were found in the literature between 1988 and 2016 [4-11] (Table 1).
|
Table 1: Literature review with all publications about micro AVM, with case reports and series, including number of patients and mean age, number of micro AVMS, site, clinical presentation, treatment technique, occlusion rate, complication rate and clinical follow up. |
||||||||||||
|
Author/year |
Nº patients |
Mean age |
NºMicro AVM |
AVM site |
Ruptured (%) |
Unruptured (%) |
surgery |
radiosurgery |
Embolization/ liquid embolic/ Nº patients |
Occlusion Rate(%) |
Complication (%) |
mRS 0–2 (%) |
|
1)Willinsky R 1988 |
13 |
31 |
13 |
Supratentoral-11 Infratentorial-2 |
100 |
- |
13 |
- |
- |
100 |
- |
- |
|
2)Tanaka M 2001 |
3 |
36 |
3 |
Supratentoral-2 Infratentorial-1 |
100 |
- |
- |
- |
3 -PVA
|
100 |
- |
100 |
|
3)Cellerini M 2002 |
10 |
48.8 |
10 |
Supratentoral-8 Infratentorial-2 |
100 |
- |
5 |
- |
5 -Histoacryl |
80 |
10 |
- |
|
4)Perrini P 2004 |
14 |
44.6 |
14 |
Supratentoral-11 Infratentorial-3 |
100 |
- |
7 |
- |
7-Histoacry |
- |
11 (vasospasm) |
93 |
|
5)Andreou A 2008 |
25 |
29.7 |
26 |
Supratentoral-18 Infratentorial-8 |
100 |
- |
- |
- |
5 -Histoacryl 20 - Glubran 1 -Ônix 18 |
84.6 |
12 |
60 |
|
6)Alén JF 2013 |
28 |
35.5 |
28 |
Supratentoral-22 Infratentorial-6 |
93 |
7 |
16 |
6 |
2 -Histoacryl |
91 |
- |
64 |
|
7)Hong JF 2015 |
13 |
32.6 |
13 |
Supratentoral-13 Infratentorial-0 |
100 |
- |
10 |
2 |
1 –Ônix 18 |
100 |
- |
77 |
|
8)Cai J 2016 |
1 |
21 |
2 |
Supra tentorial-2 Infratentorial-0 |
100 |
- |
- |
- |
2 -Ônix 18 |
100 |
- |
100 |
In one paper with just one case report [11], another with a series of 3 cases [6]. However, most of publications had more than 10 cases, and the biggest with 28 cases (ALEN). All were retrospective study. They include 107 patients with 109 micro AVMs (Table 1). The mean age of all studies was 35 years. In almost all cases the initial diagnosis was performed after a hemorrhage (intraparenchymal, lobar, subcortical or intraventricular) and just in 7 cases was unruptured (6.5%). In the most of cases micro AVMs were supratentorial in 87 cases (80%) and infra tentorial were 22 cases (20%). The main treatment was through microsurgery in 46.7% of the cases and this had relationship with the surgical treatment of hematoma. Endovascular treatment has been used more recently and comprising 42.2% of all cases and about 7.3% performed radiosurgery treatment. Endovascular treatment was performed with many different materials as polyvinyl alcohol (PVA) particles, NBCA (N-Butyl Cyano Acrylate) and EVOH (Ônix 18®). In cases of embolization in most of them N-Butyl Cyano Acrylate was used in 84.7% of the cases, followed by EVOH in 8.6% and PVA particles in 6.5% of the cases. Treatment success was achieved in almost all cases regardless of the technique microsurgery, embolization or radiosurgery.
DISCUSSION
Micro-AVMs are composed of a small nidus or a fistula by digital subtraction angiography (DSA) and they are low-volume slow-flow lesions, as demonstrated by filling in the late arterial phase and by definition the feeding artery is not usually dilated, and there is no transdural supply. Venous drainage is usually to a single draining vein of normal or slightly enlarged caliber [3]. These micro AVMs of the brain have been defined as those AVMs with a nidus less than 1 centimeter in size of the nidus [1]. Some authors have subsequently reported the presence of small vascular malformations in the margins of intracranial hematoma [2]. Early angiography may not show the AVM, because usually present with an intracerebral hematoma (ICH) [1,4]. Often the nidus itself is not perceptible, but an early draining vein is evident at the site of the hematoma. Theorectally in this kind of malformations it is speculated that have large bridging arteries that anchor the draining veins to the brain parenchyma producing outflow obstruction and increased venous pressure and are generally considered to have a high risk of bleeding [4]. However, their propensity to bleed may also reflect the fact that their small size and flow characteristics preclude presentation with other symptoms and incidental detection on CT or MRI. Neither CT nor MRI findings are usually diagnostic; DSA is the most accurate diagnostic examination, although findings are often subtle or nonspecific.
The diagnosis of micro AVM may be difficult and challenging. Diagnosis requires a high index of suspicion. In young patients (< 40 years of age) with large superficial hematomas should suggest the possibility of an underlying micro AVM. Vascular lesions can be found in patients with spontaneous subcortical hemorrhage up to 30% [12]. This finding has also been describing in patients with subcortical hematoma undergoing surgical treatment and histophatological analysis of the material showing critical AVMs in 43% of the cases [13].
Early angiography in the setting of a large hemorrhage may obscure identification of the micro AVM and something’s as low blood flow through the lesion, intralesional thrombosis, post hemorrhagic vascular spasm, or compression of the vessels by the hematoma may account for the lack of visualization of the micro AVM in the acute or sub-acute phase [12,14].
Cerebral angiography (DSA) has been considered to be the method of choice “gold standard” for the detection of vascular malformations. The lack of visualization on the initial angiogram obtained during the acute phase may be explained by compression of the vessel lumens and/or destruction of the abnormal vessels by the hematoma, vascular thrombosis due to gross hemorrhage, and/or post hemorrhagic vascular spasm. In a series with micro AVM in 15 patients, super selective angiography (SA) it was perform in four of these 15 patients with ICH, were sedated using neuroleptic anesthesia, for the purpose of either confirming the diagnosis [15]. In cases with ICH and negatives first and also repeated selective cerebral angiography (four-vessel study), super selective angiography can be perform to search this unusual kind of AVM [6]. The term dormant has been used in cases with haemorrhage and when the first DSA is negative and the patient can have another stroke some month’s later [11]. This dominant presentation with hemorrhage contrasts with that for larger AVMs, in which 65%-70% of cases present with hemorrhage and in that it causes substantial neurological impairment [4,5,8,16]. The effects seem to be related to dimensions of the parenchymal hematoma and its cortical location, which frequently involves eloquent area, in a literature series the mean volume of the parenchymal hematoma was between 25 and 33ml and most of patients had a focal neurological deficit at the initial diagnosis and needed urgent surgery [9,10]. Neurologic morbidity rates after AVM hemorrhage average 20-30% [17]. For this reason, negative or questionable conventional DSA findings in young adults with atypical hemorrhaging should prompt a repetition of the examination after complete resorption of the cerebral hematoma, and superselective angiographic exploration should eventually follow [5]. Careful examination uncovers a “hidden vessel” in the arterial phase, revealing its identity as an early draining vein as in our first case (Figure 1).
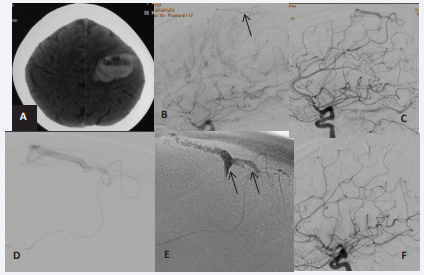
Figure 1: A) CT scan in axial section showing a left frontal intracerebral hematoma(ICH); B) DSA in acute phase was apparently normal, however a small feeding frontal venous was doubt( black arrow); C) DSA control confirming a micro AVM, 3 months later; D) SA shwoing venous drainage; E) Superselective embolization with EVHO( SQUID 18®) (black arrows); F) DSA follow up 12 months later showing a total occlusion of the micro AVM.
The angiographic aspects of the micro AVMs may give the appearance of a fistula (Figure 3). In general, the feeding artery of a micro AVM is a single vessel, a small branch of a normal-sized artery and unlike larger AVMs, there is usually no significant dilation of the feeding vessel and do not recruit extradural supply [4]. In fact, the draining vein of the micro AVM is enlarged, as it corresponds to a small cortical vein usually not seen on angiography. But since it appears within the range of normal veins on angiography, it is described as a “normal-sized vein”. They can also present with seizures, neurological deficit or headaches.
New Technologies in diagnosis as rotational angiography with 3D reconstruction has been shown as a supplementary technique to DSA and the additional information obtained through the acquisition of 3D has some advantages as review of the multiple angles AVM nidus, anatomy of the arterial pedicle and his diameter to program the optimal embolization [18].
In our series we had two cases that bled with intraparenchimal hematoma and one case, third case (Figure 3),
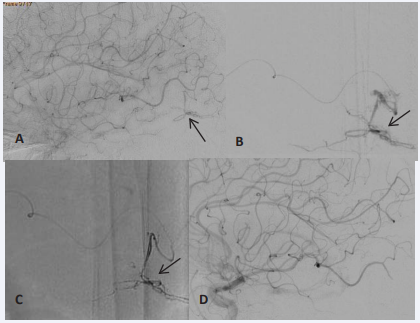
Figure 3: A) DSA showing a left temporal micro AVM (black arrow); B) SA showing a micro AMV (black arrow); C) Superselective embolization with EVHO (SQUID 18®) (black arrow); D) DSA follow up 12 months later showing a total occlusion of the micro AVM
with temporal unruptured micro AVM diagnosed during research for epilepsy. In the ruptured cases, at first case (Figure 1) we did not see the micro AVM at the first angiogram, with questionable conventional DSA findings, just a low flow cortical vein, at the 3 month follow up, after hematoma resorption, in a second angiography and SA exploration of the arterial pedicle enabled precise anatomic location of the lesion and characterization of the angioarchitecture of the nidus and we saw the micro AVM and his cortical drein vein. Superlective distal angiography show a micro nidus and on the control angiography a total occlusion after embolization. At 2nd case, the diagnosis of the micro AVM was not performed after hemorrhage and also during the follow up that was done by annual Angio MRI (Figure 2)
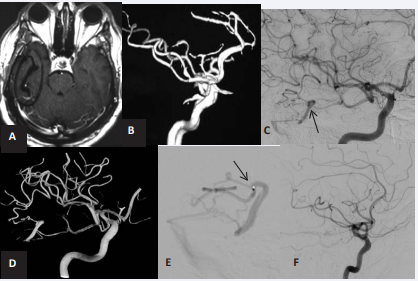
Figure 2: A) MRI in axial section showing a right temporal cavit after absortion of the ICH; B) Angio MRI follow up negative for AVM; C) DSA 3 years later showing a right temporal micro AVM (black arrow); D) 3D DSAconfirming the micro AVM and his details; E) SA showing a micro AMV and it drainage vein and the tip of microcatheter(black arrow); F) DSA follow up 12 months later showing a total occlusion of the micro AVM.
and after 3 years in a second opinion with us, an angiography and 3D DSA showed the right temporal nidus of micro AVM, and an embolization was performed with his total occlusion.
Treatment options for intracranial AVMs should be based on the patient’s clinical picture, the size of the parenchymal hematoma, the location and characteristics of the micro AVM and these include radiosurgery, conventional microsurgery, and endovascular embolization. In generally surgical removal is the main method of treatment for the superficial lesion, under the condition that the volume of hematoma is more than 40 mL and the patients began to complain of consciousness disturbance [10]. Micro AVMs are tiny lesions, their accurate localization represents one of the major problems encountered during surgical resection in cases of unruptured micro AVMs. Small AVMs that fulfill the selection criteria for curative embolization are likely to be suitable for surgical removal or radiosurgery as well. Endovascular embolization is suitable for the lesion site located in the deeper brain and is not suitable for surgery removal. The typical findings of micro AVMs as distal and deep location and tortuous and small feeding arterial supply are the majors limiting factors for successful embolization and we can see some reported unsuccessful embolization of micro AVMs [4]. Most recently, major technical progresses in the field of endovascular therapy have expanded the armamentarium of treatment strategies for cerebral AVMs with the good evolution of the material for embolization as new distal access catheters, new detachable micro catheters and also new embolic liquids, an endovascular approach could be considered as an alternative treatment for micro AVMs. Although embolization of micro AVMs can be complicated by hemorrhage or dissection due to perforation of the small-sized as well as vasospasm due to tortuous feeding arteries during navigation of the micro catheter, we can see in the literature that it is a relatively safe therapeutic approach [8]. The rate of complication due the vessel perforation can reach 22.2% [7] but sometimes this kind of minor perforation may be a silent microperforation. The goal of embolization in micro AVMs is the complete and permanent obliteration of the AVM nidus. However, given the homogeneous features found in all series with high risk of sudden haemorrage that high volume intraparenchymal hematoma and neurological deficit, the good therapeutic results with total occlusion when performed endovascular approach or total exclusion in surgery approach (Table 1) suggest that any micro AVM diagnosed should be treated. Our series was too small to allow us to draw any statistical conclusions about the relationships between micro AVM localization, embolization treatment and outcomes. However, the findings are in agreement with reported data in that and the literature results (Table 1). In our series, one patient had a suggestive history of a previous hemorrhagic episode and limited negative Angio MRI follow up, but some years later a correct angiography and 3D DSA showed a micro AVM and also another case with a suggestive hemorrhagic episode and angiography diagnosis, has gotten a correct angiography follow up and confirmed a micro AVM. In the unruptured case with previous diagnosis of left temporal micro AVM by MRI and angiography, the patient had epilepsy and daily seizures and refractory to multiple drugs treatment and a contra indication to the surgical treatment and also endovascular or radiosurgery treatment by the responsible medical team for tem years. In a second opinion with our team, we decided to the embolization and at the long term follow up the patient had a better seizures control.
CONCLUSION
Micro-AVMs typically occur with relatively large intracranial hemorrhages along with associated significant neurological deficits in young adults. These lesions may go undetected on routine diagnostic workups. When the initial angiography is negative or dubious, delayed angiography or super selective angiography is recommended. In deep and subcortical lesions endovascular catheterization and embolization were possible in the majority of patients despite the small size of the feeding arteries, the distal location of these lesions, and the initial under diagnosis associated with micro-AVMs in the brain. 3D angiography reconstruction images is modern tool for the analyzing the best treatment for these lesions. Single-shot embolization and a high immediate and permanent obliteration rate were achieved in this series. Embolization may be a safe alternative to the established surgical therapy in select cases and depend mostly on the clinical conditions at admission, but for the incidental deep lesions endovascular embolization with embolic liquids can be a good and safe alternative.
REFERENCES
- Ya?argil MG. Microneurosurgery: AVM of the Brain, History, Embryology, Pathological Considerations, Hemodynamics, Diagnostic Studies, Microsurgical Anatomy. Stuttgart: Georg Thieme.1987; Vol IIIA: 85.
- Stiver IS, Ogilvy CS. Micro-arteriovenous malformations: significant hemorrhage from small arteriovenous shunts. Neurosurgery. 2000; 46: 811-819.
- Berenstein A, Lasjaunias P, terBrugge KG: Surgical Neuroangiography. New York: Springer-Verlag. 2004; 3: 655-656.
- Willinsky R, Lasjaunias P, Comoy J, Pruvost P. Cerebral microarteriovenous malformations (mAVMs). Review of 13 cases. Acta Neurochir (Wien). 1988; 91: 37-41.
- Cellerini M, Mangiafico S, Villa G, Nistri M, Pandolfo C, Noubari H, et al. Cerebral microarteriovenous malformations: diagnostic and therapeutic features in a series of patients. AJNR Am J Neuroradiol. 2002; 23: 945-952.
- Tanaka M, Valavanis A. Role of superselective angiography in the detection and endovascular treatment of ruptured occult arteriovenous malformations. Interv Neuroradiol. 2001; 7: 303-311.
- Perrini P, Scollato A, Cellerini M, Mangiafico S, Ammannati F, Mennonna P, et al. Results of surgical and endovascular treatment of intracranial micro-arteriovenous malformations with emphasis on superselective angiography. Acta Neurochir (Wien). 2004; 146: 755-766.
- Andreou A, Ioannidis I, Lalloo S, Nickolaos N, Byrne JV. Endovascular treatment of intracranial microarteriovenous malformations. J Neurosurg. 2008; 109: 1091-1097.
- Alén JF, Lagares A, Paredes I, Campollo J, Navia P, Ramos A, et al. Cerebral microarteriovenous malformations: a series of 28 cases. J Neurosurg. 2013; 119: 594-602.
- Hong JF, Song YF, Liu HB, Liu Z, Wang SS. The Clinical Characteristics and Treatment of Cerebral Microarteriovenous Malformation Presenting with Intracerebral Hemorrhage: A Series of 13 Cases. Biomed Res Int. 2015; 2015: 257153.
- Cai J, Lin H, Li S, Zou Z, Zhang Y, Liu S, et al. Dormant micro arteriovenous malformations lead to recurrent cerebral haemorrhage. Springerplus. 2016; 5: 1054.
- Hino A, Fujimoto M, Yamaki T, Iwamoto Y, Katsumori T. Value of repeat angiography in patients with spontaneous subcortical hemorrhage. Stroke. 1998; 29: 2517-2521.
- Elhammady MS, Baskaya MK, Heros RC. Early elective surgical exploration of spontaneous intracerebral hematomas of unknown origin. J Neurosurg. 2008; 109: 1005-1011.
- Ogilvy CS, Heros RC, Ojemann RG, New PF. Angiographically occult arteriovenous malformations. J Neurosurg. 1988; 69: 350-355.
- Willinsky R, TerBruge K, Montanera W, Wallace C, Aggarwal S. Micro-arteriovenous malformations of the brain: superselective angiography in diagnosis and treatment. AJNR Am J Neuroradiol. 1992; 13: 325-330.
- Crawford PM, West CR, Chadwick DW, Shaw MD. Arteriovenous malformations of the brain: natural history in unoperated patients. J Neurol Neurosurg Psychiatry.1986; 49: 1-10.
- Graf CJ, Perret GE, Torner JC. Bleeding from cerebral arteriovenous malformations as part of their natural history. J Neurosurg. 1983; 58: 331-337.
- Kakizawa Y, Nagashima H, Oya F, Ito K, Tanaka Y, Hongo K, et al. Compartments in arteriovenous malformation nidi demonstrated with rotational three-dimensional digital subtraction angiography by using selective microcatheterization. Report of three cases. J Neurosurg. 2002; 96: 770-774.







































































































































{kind=link}