Effects of Myocardial Bridges on Coronary Blood Flow: an Insight Provided by iFR
- 1. Department of Cardiology, ARNAS Civico Hospital, Italy
Citation
Caruso M (2023) Effects of Myocardial Bridges on Coronary Blood Flow: an Insight Provided by iFR. Ann Vasc Med Res 10(2): 1163.
INTRODUCTION
Intramyocardial segments of epicardial coronary arteries are common findings among patients undergoing coronary angiography, and their role as a potential cause of anginal symptoms has been broadly described [1]. Extravascular compression, mediated by myocardial systolic contraction, squeezes the coronary lumen and overshoots intraluminal pressure. The effect of squeezing on intracoronary pressure is significantly higher distally, so that during systole there is a negative gradient through the intramyocardial tract, which is inverted during diastole (Figure 1).
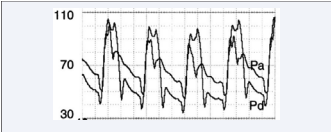
Figure 1: Pressure curves proximal (Pa) and distal (Pd) to the intramyocardial bridge during dobutamine infusion, enhancing myocardial inotropism. During systole, distal pressure overcomes the proximal one. The gradient is inverted during diastole, when the squeezing ends.
Such hemodynamic implications of muscular bridges are the pathophysiological cause underlying the onset of the anginal sympthoms described by some of these patients, but the quantitative assessment of inducible ischemia, in this context, is still debated [2].
Figure 1: Pressure curves proximal (Pa) and distal (Pd) to the intramyocardial bridge during dobutamine infusion, enhancing myocardial inotropism. During systole, distal pressure overcomes the proximal one. The gradient is inverted during diastole, when the squeezing ends.
Although pressure wires have provided a consistent proof of inducible ischemia for the most significant phasic stenoses, FFR might be useless in these cases since it’s calculated on the whole cardiac cycle, and the alternance of positive and negative gradients can thus result in a non-significant average value underestimating the ischemic potential of the dynamic squeezing. technique for the functional assessment of coronary stenoses, with the advantages of being calculated exclusively during the diastolic “wave-free period” and without the need of a pharmacologically-induced vasodilation. Such features make the iFR technology potentially helpful when the myocardial-bridgeinduced ischemia has to be demonstrated to drive therapeutic choices (Figure 2).
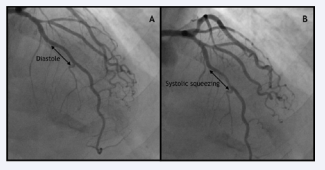
Figure 2: Angiograms of the Left Coronary Artery during diastole (A) and systole (B) showing the phasic stenosis determined by the myocardial bridge on the middle tract of the LAD (Left Anterior Descending).
On this topic, we report the case of a 74-year-old man who underwent a coronary angiography in our Cath Lab for an exertional angina, re-evoked during stress testing with concomitant ST-segment depression in precordial leads.
Angiograms showed no significant coronary atherosclerosis, except for a proximal intermediate lesion of the main Diagonal branch and a mild focal narrowing of the proximal LAD (Left Anterior Descending), with an intramiocardial tract of its intermediate segment accounting for a phasic stenosis of about 60% of coronary lumen (Figure 2).
In order to assess the functional significance of the same lesions, we used a pressure wire (iFR - Volcano Corporation, San Diego, CA, USA) and calculated iFR through the stenoses on the proximal LAD (0,95), the diagonal branch (0,92) and the distal LAD beyond the intramyocardial tract (positive: 0,87), where FFR had failed to demonstrate the hemodynamic significance of the phasic squeezing (FFR on distal LAD after intravenous infusion of adenosine: 0,88) (Figure 3).
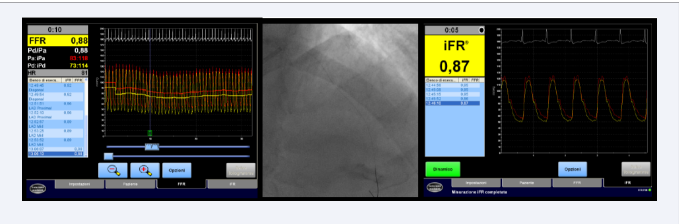
Figure 3: Records of FFR (left) and iFR (right) on LAD coronary artery (angiogram in the middle).
iFR demonstration of the ischemic significance of the myocardial bridge drove subsequent optimization of medical therapy with calcium channel blockers and low-dose beta blockers, allowing the achievement of a good control of anginal symptoms and an increase in functional capacity of the patient.
In the previous years, anatomical and functional features of myocardial bridges have been step by step clarified in their key points, providing a likely explanation for a wide span of ischemic patients even in absence of a significant coronary artery disease. Initial angiographic observations of systolic squeezing, determinant of the peculiar “milking effect” [3,4], have been better analyzed with current technologies, and quantitative coronary angiography has shown how extramural compression persists even during diastole. In this phase, microvascular vasodilation creates a gradient through the MB resulting in an abrupt acceleration of blood flood in the intramiocardial tract, clearly visible when a doppler wave is recorded here and previously described as the “fingertip phenomenon”, followed by a rapid deceleration and a plateau phase occurring when the cross-sectional area of the lumen increases. The final result of extravascular squeezing has been deemed to be significant when it provokes a 70% decrease of luminal diameter during systole persisting with a 35% decrease during diastole [5]. Such delay in diastolic relaxation and its hemodynamic implications on blood flow are the most important determinants of the inducible ischemia, which is often clearly related to physical efforts during which cardiac inotropism, and consequently extramural compression, increases and tachycardia shortens diastolic perfusion, significantly impairing myocardial blood supply.
However, not every myocardial bridge is a potential source of ischemia, since the anatomical features of the intramiocardial tract, as its length, thickness and myocardial fibers’ orientation markedly influence its functional effects, and the most appropriate tool to assess them is still a matter of debate and a true gold standard has never been validated. Fractional flow reserve across the bridge can be measured and provide proof of significant ischemia when <0,75 [6], but in many cases, like ours, FFR fails, since the detection of a diastolic gradient is mitigated by its systolic invertion, resulting in a negative whole-cycle average ratio between distal and proximal pressures. Conversely, iFR focuses on pressure measurements during the diastolic wave-free period, with the advantage of neglecting systolic inversion and assessing the isolated ischemic potential of the diastolic relaxation delay. “Diastolic FFR” has been previously proposed with the same purpose [2] but is not commonly used nor validated in larger case series.
By contrast, recent studies have significantly widened the indications for iFR, shown to be non-inferior to FFR as a guidance for percutaneous coronary interventions.
Our case shows one of the scenarios in which iFR is probably superior in comparison to its precursor, since the pathophysiological mechanisms underlying inducible ischemia for myocardial bridges are significantly different from those implicated by a fixed coronary stenoses. The exclusive evaluation of diastolic gradients provides an advantage which could be able, as in our case, to show an otherwise masked intraluminal gradient, conferring iFR the potential to become a true gold standard, if confirmed by wider validation studies, for the functional assessment of intramyocardial tracts of epicardial coronary arteries.
REFERENCES
3. Bourassa MG, Bernard P, Brevers G, Petitclerc R, Dyrda I. Systolic and early diastolic inflow obstruction in patients with muscular bridging of the left anterior descending artery. In: Bruschke AVG, van Herpen G, Vermeulen FEE, editors. Coronary Artery Disease Today. Princeton, NJ: Excerpta Medica, 1981: 380–94.







































































































































{kind=link}