GoBack
- 1. UOS Radiologia Interventistica, Valduce Hospital, Italy
- 2. UO Chirurgia Vascolare, Institute of Care of the City of Pavia, Italy
Abstract
Background: Treatment of graft limb occlusion can be challenging but the multifunctionality of the GoBack crossing e reentry device helps to overcome difficult situations and prevents alternative approaches to the endovascular one.
This novel device allows direction-change inside hard plaque and crossing of tough lesions ensures an excellent pushability.
Case Presentation: A 74-year-old male with a long occlusion of the right common iliac artery, due to a graft folding. After several failed crossing attempts, recanalization and flow restoration in the common femoral artery on both sides were performed with the GoBack crossing catheter.
Conclusions: The GoBack crossing catheter should be consider the preferred catheter to deal with tough occlusions being a well-grounded complementary interventional instrumentation tool.
Citation
Azzaretti A, Bonalumi G, Mazzotta G, Beneggi IM, Stabile A, et al. (2022) GoBack™ Catheter: A Trans-Replacement Recanalization of the Right Leg in Chronic Occlusion of an Aortic Graft. Ann Vasc Med Res 9(1): 1138.
BACKGROUND
Although graft limb occlusion recanalization can be challenging, it is a well-established procedure, generally performed using endovascular techniques. Nevertheless, the high failure rates render the surgical approach the only viable option. Within this framework, improvement of wire technologies and crossing devices could significantly improve procedural success rates [1,2].
The GoBack™ Crossing Catheter (Upstream Peripheral Technologies, Caesaria - Israel) is a single-lumen crossing catheter that features a curved nitinol needle at its distal tip, with an adjustable protrusion length from a straight (2-3 mm) to a fully curved (11 mm) position. These features mark it as the only available medical device suitable for intraluminal crossing or subintimal re-entry. Indeed, the novel-designed GoBack™ Crossing Catheter has been thought to enable directional change inside hard plaques and crossing of firm lesions, thereby enhancing procedure effectiveness.
CASE PRESENTATION
A 74-year-old male was admitted with right limb intermittent claudication (Rutherford category 3), which was managed using a clinical procedure as previously described [3]. Aneurysmectomy of the abdominal aorta had been performed 2 years earlier, using an open surgical approach and placement of aorto-bi-iliac Dacron graft (14X7 mm). One year after the surgical procedure, the patient reported on sural claudication at 150 m. An angio-CT scan of the abdomen and lower limbs showed an aortic diameter of 17 mm at the lower level, with a normal lumen, normal patency of the left iliac branch and 13 mm long occlusion of the right common iliac artery, due to a graft folding. The right iliac bifurcation was revascularized by collateral circulation and the ipsilateral hypogastric artery was patent with significant calcifications. Both femoral arteries were patent with diffuse calcification (Figure 1).

Figure 1 CT-scan and angiography image performed before the procedure.
After local anesthesia, a standard bilateral femoral arterial transcutaneous approach was performed, by inserting a 6 Fr introducer sheath on the left side and 8 Fr introducer sheath on the right side, and administration of 5000UI heparin. The right iliac branch occlusion was confirmed by a preliminary angiography performed through a 4FR pig tail catheter, positioned in abdominal aorta via the left iliac branch. Attempts to cross the right common iliac artery occlusion were consistently unsuccessful. A GoBack™ catheter 4 Fr with 0.018’’ guidewire ASAHI Gladius MG 18 PV ES (Asahi Intecc, Nagoya - Japan) was inserted from the right common femoral artery and advanced to the desired location. The needle was then extended to 5-7 mm. Using the needle’s distal radio-opaque marker served as a guide as to the axial and radial position of the tip, the GoBack™ needle was oriented to cross the occlusion (Figure 2).
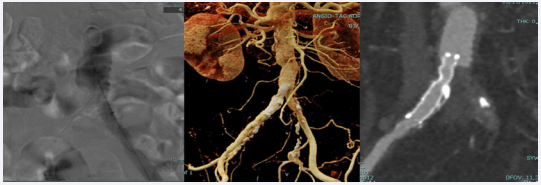
Figure 2: Catheter-based angiography showing the GoBack, CT-scan and angiography follow up at 3 month.
Then, pre-dilation to 4 mm was performed using a lowprofile Sterling balloon catheter (Boston Scientific Corporation, Natik - USA). On the right side, a Viabahn (BD, Franklin Lakes – USA) stent-graft (8x50 mm) was arranged with distal landing in the common ipsilateral iliac artery and with proximal landing in an aortic prosthesis. Then, a post-dilation was performed at 8 mm proximally and at 7 mm distally. The final angiographic assessment clearly demonstrated occlusion resolution and restored direct flow in the common femoral artery on both sides. No periprocedural complications emerged. Access hemostasis was performed with 6/7 F Femoseal. At first clinical control after one month sural claudication was resolved and CT-scan follow up at 3 months confirmed patency of right iliac axis with triphasic flow at DUS examination (Figure 2).
CONCLUSION
Conventional clinical endovascular methods are mostly unsuccessful in cross occlusions, as in the reported case in which the occlusion could not be resolved with a standard approach. The GoBack™ catheter allowed for stenting of the right iliac axis with a covered stent, with subsequent restoration of the physiological flow and symptom relief. For this reason, the GoBack™ catheter should be considered a viable and effective re-entry technique, suitable even for strong occlusions resulting from a folded vascular graft.
In conclusion it should be consider the preferred catheter to deal with tough occlusions being a well-grounded complementary interventional instrumentation tool [4].









































































































































{kind=link}