Type B Aortic Dissection in the Last 15 Years in Brazil: A Statistical Analysis
- 1. PhD in Medicine and Health, Federal University of Bahia, Brazil
- 2. 3rd year Medical Student, Bahiana School of Medicine and Public Health, Brazil
- 3. 4rd year Medical Student, Bahiana School of Medicine and Public Health, Brazil
- 4. General and Thoracic Surgeon, Member of Brazilian Society of Thoracic Surgery, Brazil
ABSTRACT
Introduction: Acute aortic dissection is a complex pathology with high morbidity and mortality that requires an effective health system with a skilled and available team. Brazil’s vast territory and its socio-economic differences may have an impact on the diagnosis, treatment and prognosis of this disease.
Objective: To describe the statistical behavior of AD available in the Brazilian public health system database (DataSUS).
Materials and Methods: An observational, retrospective, aggregate, descriptive and documentary study of secondary data extracted from the SUS Hospital Information System (SIH/SUS), available in the DataSUS database from 2008 to 2023, of patients with type B aortic dissection. Type A dissections were excluded.
Results: 4325 authorizations for hospital admissions and 1342 deaths for dissection repair were recorded. The Southeast had the highest total number of hospitalizations due to the procedure (49%), while the South had the highest prevalence (0.235 per 100,000 inhabitants). The average number of days spent in hospital was 12.6 days. In terms of total expenditure, 36.38% of these were elective admissions, while 63.60% were emergency admissions. In both cases, the Southeast was the region that paid the most, accounting for 56.83% of the national amount in elective cases and 44.38% in emergency cases. The average dollar amount spent on this procedure during this time series was $2,596.94, of which $2,529.66 on an elective basis and $2,637.87 on an emergency basis, showing no significant discrepancies. The number of hospitalizations on an emergency basis was significantly higher than on an elective basis (62.64% and 37.36%, respectively).
Conclusion: There was a concentration of figures in the Southeast region of the country, which led the way in terms of the total number of hospitalizations and deaths and accounted for almost half of the expenditure on the correction procedure. Equal public policies are needed throughout Brazil for early diagnosis and more elective treatment of AD.
KEYWORDS
- Dissection
- Aorta
- Pain
CITATION
Borges WR, Menezes RDS, de Farias IP, Lima GN, Arpini PAA, et al. (2024) Type B Aortic Dissection in the Last 15 Years in Brazil: A Statisti- cal Analysis. Ann Vasc Med Res 11(2): 1183.
INTRODUCTION
Acute aortic dissection (AD), first described by the English physician Frank Nicholls in 1761, is a serious and potentially fatal condition in which rupture of the intimal layer of the aorta, with separation of the intima from the media, causes the formation of a false lumen. This pathology manifests itself abruptly and its pathophysiology involves numerous hemodynamic and structural interactions between the vessels, which intensify as the dissection progresses. According to the Stanford classification, aortic dissections can be divided into two types: A necessarily involves the ascending aorta, while B involves the descending aorta [1,2]. AD, whose global incidence is estimated at between 2.6 and 3.5 cases per 100,000 people per year, is considered an extremely serious emergency, with a mortality rate of 90% when not identified and treated early [3-5].
It has been reported that the overall percentage of in- hospital mortality after surgical treatment of patients with aortic dissection is 15 to 25% [6]. The major causes of perioperative mortality and morbidity are acute myocardial infarction (AMI), paraplegia, renal failure, tamponade, hemorrhage and sepsis [6]. However, the long-term prognosis for patients with treated aortic dissections is generally good when there is careful follow- up. In these cases, the 10-year survival rate is around 60%.
Furthermore, in a study published in 2023 by the Brazilian Journal of Development, AD was described as being responsible for 7% of sudden out-of-hospital deaths and had a 40% mortality rate if identified early, with an increase of 1% every hour that passes when there is no proper management of the disease [7].
Systemic arterial hypertension is the main risk factor for AD, present in over 70% of cases. Other factors include previous heart surgery, chest trauma, bicuspid aortic valve, smoking, trauma, intense physical exertion, family history of aortic disease and syndromes such as Turner’s, Ehlers-Danlos and Marfan’s syndrome, in which 44% of individuals may present. Older age and drug use have also been characterized as risk factors for developing AD [3].
Type B AD is a disease that, when symptomatic, presents with sudden and intense pain, typically in the chest, accompanied by hypertension and possibly neurological deficits [8]. However, studies show that in practice this condition can present with very varied symptoms, as well as mimicking other diseases, making its diagnosis a challenge for medical practice and making epidemiological analyses of the disease difficult [9]. Complicated type B AD is treated surgically by thoracic aortic endovascular repair (TEVAR) or, in cases of anatomical difficulties, by open surgery [10-12].
As this is a disease with a high morbidity and mortality rate, it is imperative to evaluate epidemiological variants that may have an impact on the diagnostic and therapeutic management of these cases. As Brazil is a country of vast continental extension and strong socio-economic inequalities, we decided to evaluate the variables available in the Brazilian government’s health data system in order to provide a statistical description of type B aortic dissection in Brazil.
MATERIALS AND METHODS
This is an observational, retrospective, aggregated and descriptive study of secondary data extracted from the SUS Hospital Information System (SIH/SUS), available in the DataSUS database, referring to patients admitted to hospital and who died in Brazil between 2008 and 2023, by place of residence. Data recorded as “thoracoabdominal aortic aneurysm/dissection repair” was taken into account. The data obtained was then processed in Microsoft Excel software, where the tables and graphs relating to the data collected were constructed. These data can be checked on the TabNet portal, at the following link: https://datasus.saude.gov.br/
Although the data referring to thoracic-abdominal aneurysm repair is not distinguished from that of thoracic-abdominal aortic dissection repair, for the purposes of analysis, all the data collected will be discussed in the results and discussion as referring to the latter type of procedure, exclusively because we observed that the treatment of thoracic-abdominal or thoracic or abdominal aneurysms (not related to dissection) is partly distinct from that of AD.
To describe the profile of hospitalizations due to ED, the variables used were: number of hospitalizations; hospitalization coefficient; average length of stay; total length of stay; total amount spent; cost of professional services; cost of hospital services; average cost per hospitalization; deaths and mortality rate. These variables were also analyzed according to their distribution in Brazil’s demographic regions (North, Northeast, Midwest, Southeast, South) and according to the nature of the procedure (emergency, elective and other external causes). Given the statistical insignificance of the data recorded as “other external causes”, they were not analyzed in this study. To calculate the hospitalization coefficient, the number of hospitalizations was divided by the resident population in the respective year and region and multiplied by 100,000. The data on the resident population was taken from the demographic and socio-economic indicators in the “Study of Population Estimates by Municipality, Sex and Age - 2000-2021”, available on the DataSUS database. As it is a public health database, analysis by the Ethics Committee was not required.
RESULTS
In the period between 2008 and 2023, 4,325 authorizations for hospital admissions (AIH) for AD correction were recorded in Brazil, with no great variation over the years in the number of admissions - there were no sharp rises or falls in hospitalizations during this period - the average was approximately 270 admissions per year in Brazil.
The Southeast was the region with the highest total number of hospitalizations, with 2,100 AIH (49%), with more than 100 hospitalizations in all the years of the study, followed by the South and Northeast, with 1,109 (26%) and 688 (16%), respectively. In addition, the regions with the lowest absolute records were the North, with 153 (4%) hospitalizations, and the Midwest, with 275 (6%). However, when analyzing each region’s hospitalization prevalence rate per 100,000 inhabitants, it can be seen that the South with 0.235 has the highest prevalence, followed by the Southeast with 0.151, the Midwest with 0.105, the Northeast with 0.077 and the North with 0.047 [Table 1].
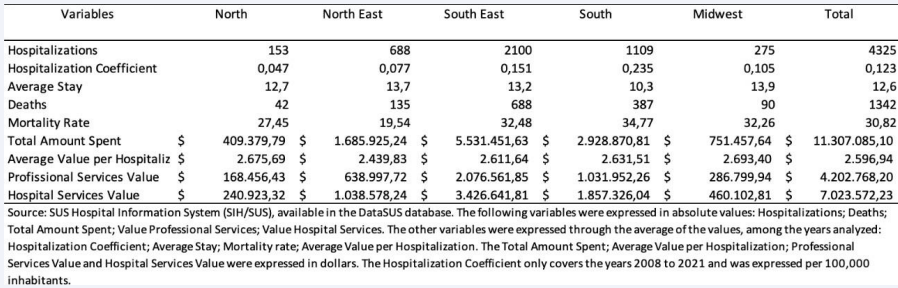
Table 1 Regional distribution of the statistical behavior of hospitalizations for correction of thoraco-abdominal aortic dissection between 2008 and 2023, in Brazil.
When we take into account the differences between the types of care, we see a significant difference in the distribution between urgent and elective care, which accounted for 62.64% and 37.36%, respectively. It was noticeable that in most regions, urgent care outweighed elective care, with the sole exception of the northeast, where the distribution between urgent and elective care was 43.13% and 56.87%, respectively. The Midwest was the region with the most significant relative difference between the types of care: 12.54% (elective care) and 87.46% (emergency care) [Graph 1].
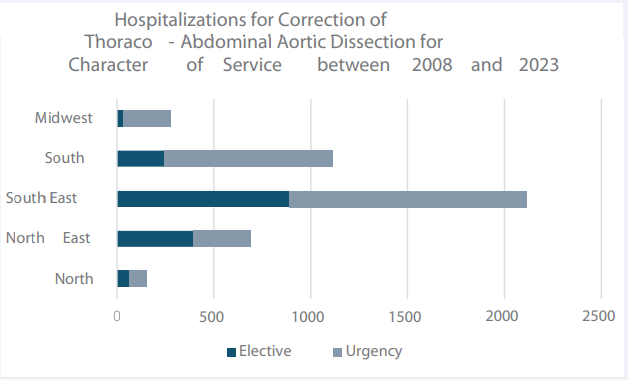
Graph 1: Hospitalizations for Correction of Thoraco-Abdominal Aortic Dissection for Character of Service between 2008 and 2023.
The average number of days spent in hospital for correction of AD during this period was 12.6 days. The average number of days spent in elective cases (14.8 days) was higher than in emergency cases (11.2 days). Almost all the regions showed the same pattern, with the exception of the North, where the average number of days spent as an emergency (13.1 days) exceeded the number spent as an elective (12 days). The region with the lowest average length of stay was the South, with 10.3 days, and the region with the highest average number of days was the Midwest, with 13.9 days [Graph 2].
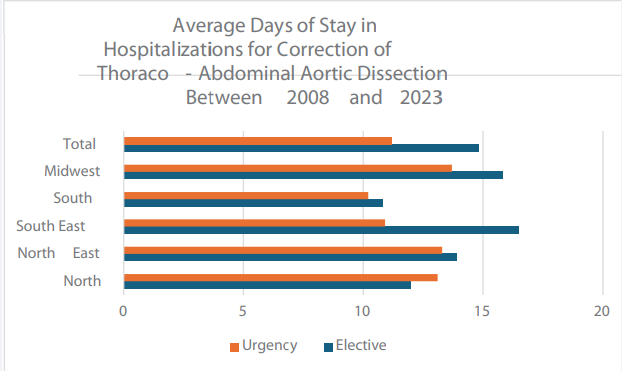
Graph 2: Average Days of Stay in Hospitalizations for Correction of Thoraco- Abdominal Aortic Dissection Between 2008 and 2023.
In total, between 2008 and 2023, there were 1,342 deaths due to AD registered in the public health system. During the period, there was a slightly increasing linear trend, in which the years with the lowest and highest number of deaths were 2014, with 67 deaths, and 2022, with 104 deaths, respectively. A significant increase in the number of deaths of 43.47% was evident between 2018 and 2019 [Graph 3].
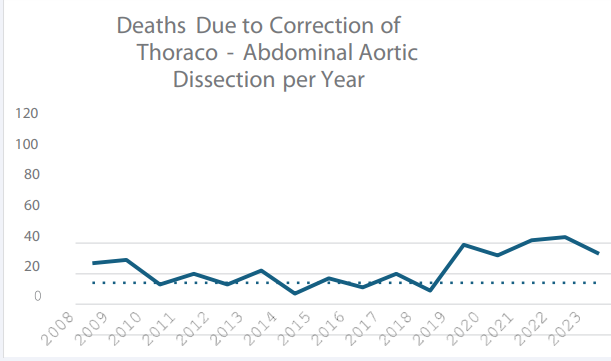
Graph 3: Deaths Due to Correction of Thoraco-Abdominal Aortic Dissection per Year.
The region with the highest total number of deaths was the Southeast with approximately 51% of deaths, followed by the South with 28% and the Northeast with 10%, while the Midwest and North had the lowest total number of deaths with 6% and 3%, respectively. Furthermore, when we take the mortality rate into account, the South region leads the way with a rate of 34.77, followed by the Southeast (32.45), Midwest (32.26), North (27.45) and Northeast (19.54) [Table 1]. When comparing the mortality rate in relation to the type of care, it is notable that during this period emergency care had a higher mortality rate in all regions when compared to elective care, a total average of 35.33 versus 23.25. The Midwest region showed the greatest discrepancy between the mortality rate and character: emergency mortality rate of 35.25 and elective mortality rate of 11.43. During this time series, the period with the highest emergency mortality rate was 2015 with 41.22, coincidentally the year in which the elective mortality rate was the lowest (14.04). The year with the highest elective mortality rate was 2020 (36.67), but this was still lower than the emergency rate (38.46) in the same year [Graphs 4 and 5].
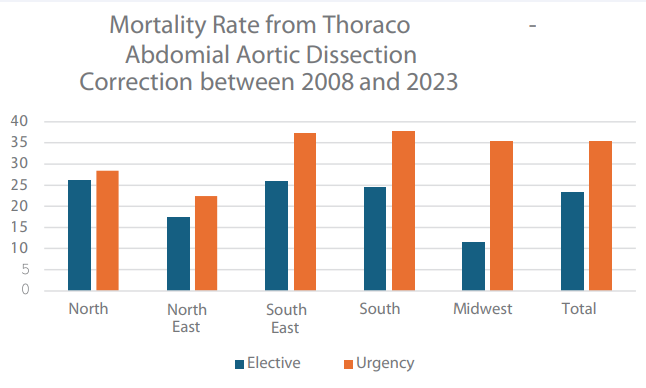
Graph 4: Mortality Rate from Thoraco- Abdomial Aortic Dissection Correction between 2008 and 2023.
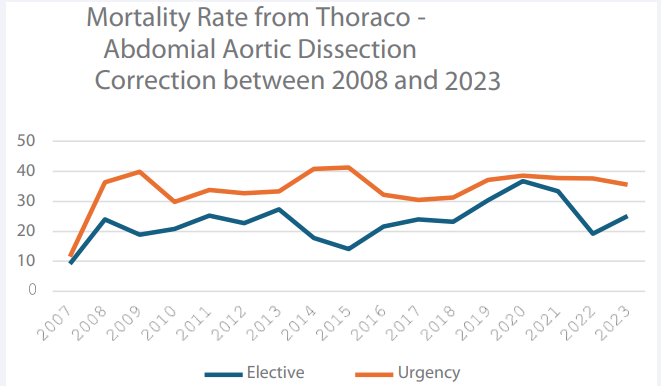
Graph 5: Mortality Rate from Thoraco- Abdomial Aortic Dissection Correction between 2008 and 2023.
The total amount spent - in dollars - by Brazil over the 16- year period (2008 to 2023) to correct AD was $11,307,085.10. There has been a noticeable increase in total spending in recent years. By way of comparison, in 2008 Brazil spent $ 516,567.71; in 2021, 13 years later, it was $ 705,986.74; and more recently, in 2023, total national spending was $ 1,435,785.61; the figure has doubled in just 2 years, a drastic change when compared to the increase between 2008 and 2021 [Graph 6].
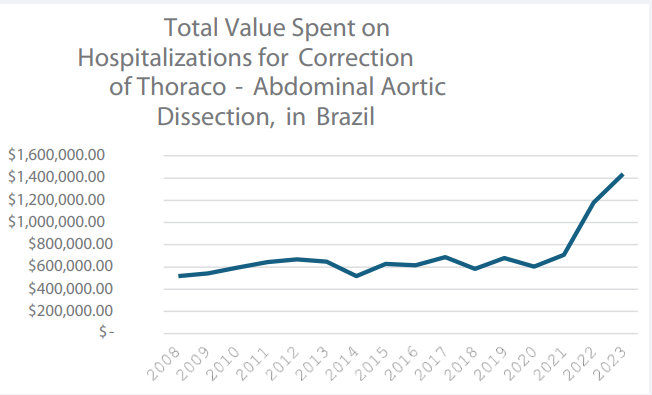
Graph 6: Total Value Spent on Hospitalizations for Correction of Thoraco- Abdominal Aortic Dissection, in Brazil.
As for the total amount spent by region, in descending order, we have: the Southeast with approximately half of the total amount spent (48.92%); the South with 25.9%; the Northeast with 14.91%; the Midwest with 6.65%; and the North with 3.62%. Looking at the graph, the highlight is the exponential increase in spending in the Southeast over the last 5 years, followed by a less significant increase in the South and Northeast. The Southeast region spent $242,391.60 in 2020 and more than tripled this amount in 2023, with a total expenditure of $750,822.66 [Graph 7].
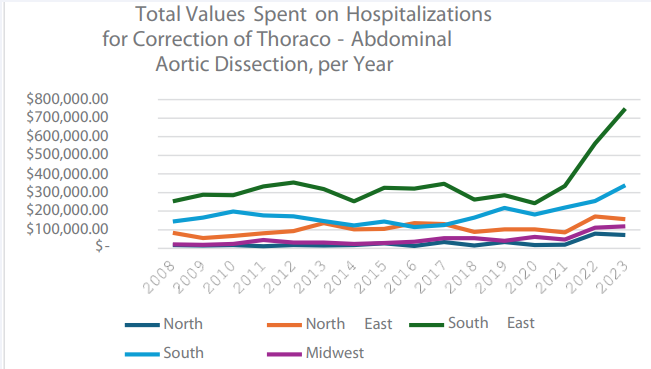
Graph 7: Total Values Spent on Hospitalizations for Correction of Thoraco- Abdominal Aortic Dissection, per Year.
Another important point is the difference in spending on professional services and hospital services for hospitalizations for corrective AD. Taking into account the total spent between 2008 and 2023 ($ 11,307,085.10), 37.17% went on professional services, while 62.12% went on hospital services. In general, all Brazilian regions spent more on hospital services than on professional services. Following the distribution pattern, the region with the highest spending on both professional services ($2,076,561.85) and hospital services ($3,426,641.81) was the Southeast. The North of the country again had the lowest amounts, $ 168,456.43 and $ 240,923.32, for professional and hospital services, respectively [Table 1].
We can also compare spending according to whether the hospitalization was elective or emergency. In relation to total spending on AD corrections, 36.38% of this was on elective admissions, while 63.60% was on emergency admissions. For both types of hospitalization, the Southeast was the region with the highest expenditure, accounting for 56.83% of the national amount for elective hospitalizations and 44.38% for emergency hospitalizations.
The average dollar amount spent on this procedure during this time series was $2,596.94, of which $2,529.66 on an elective basis and $2,637.87 on an emergency basis, showing no significant discrepancies. In general, the average amounts spent were very similar between the regions and between the different types of care. The region with the greatest discrepancy was the Midwest, where the average amount spent was $2,806.38 for urgent care and $1,905.72 for elective care.
DISCUSSION
The distribution of the total number of hospitalizations for AD by Brazilian region shows the disparities in infrastructure and sociodemographic factors that exist in Brazil. The differences in the number of inhabitants in each region was an important variable in the analysis of the data obtained for the study, as well as access to existing health services. The Southeast region stands out in terms of the absolute number of hospitalizations when compared to the other regions, followed by the South. However, based on the prevalence figures for this procedure by region, the South outperformed the Southeast, so the smaller population of the former compared to the latter is one of the factors responsible for this. Considering that these are more industrialized regions with better socio-economic indicators, the health system is more efficient.
One of the factors that explains the predominance of the Southeast and South in the number of hospitalizations and deaths is the higher quality of infrastructure and data recording in these regions, given the high investment and spending on health. Another reason for this phenomenon is the higher prevalence of cases of systemic arterial hypertension (SAH) in these regions, a reflection of longer life expectancy and an age structure with more elderly people, as shown in the 2022 Census, which recorded approximately 12.2% of the population in these regions aged 65 or over [14-16]. In addition, the population is more susceptible to developing AD, due to greater stiffening of the vessels, a higher rate of comorbidity and an increase in peripheral vascular resistance, as well as a higher concentration of elderly people in the age structure compared to the others [17].
The distribution of the total number of deaths by Brazilian region shows a great disparity in the numbers, although there was a certain proportionality in the mortality rate. There was a disproportionate number of deaths in the Southeast and South regions compared to the other regions in the same period analyzed, so that 80% of deaths were concentrated in these two regions alone. It’s worth noting that this significant difference may be influenced by underreporting, which is more likely to affect the North and Northeast regions, given their large territorial extension, together with the low level of access to tests to confirm the real cause of death, thus sometimes not recognizing the influence of dissection as the cause of death [18,19].
The distribution of the number of hospitalizations for AD by type of care shows a prevalence of urgency. This was in line with the literature, given that the clinical condition is sudden, with a prevalence of symptoms that alert the patient themselves, most of the time the pain leads them to seek out the hospital emergency department as soon as possible, resulting in hospitalizations for evaluation and follow-up care. However, it should be borne in mind that it may not be diagnosed in the non-emergency phase, which suggests that there is a need for more diagnosis of AD on an elective basis through screening policies [20]. On the other hand, elective consultations for this pathology account for approximately 1/3 of the total, but it should be noted that the only region that goes against this trend is the northeast, with a similar frequency, but with a predominance of elective hospitalizations. This scenario can be explained by the fact that the procedures are carried out at a later date by the SUS after the patients have stabilized. This electivity is due to high demand, which is often not met in the ideal time. According to a survey by the Ministry of Health, the region that stands out in terms of doctor/patient ratio with the most surgeries and elective care to be carried out is the northeast, corroborating the data from this study [21].
It can be seen that in all regions, the highest mortality rates are due to emergency care, with a clear predominance, especially in the Central-West region. It’s not so clear what the reasons are for the behavior of mortality due to the urgent procedure of AD correction in central Brazil, but it’s completely understandable that the majority of deaths are due to more serious pathologies that take the patient to the emergency room (urgent) when compared to less serious cases (elective).
There has been a significant increase in spending on correcting AD over the period analyzed (2008-2023). In 2008, Brazil spent $ 516,567.71, while in 2021 this figure rose to $ 705,986.74, and in 2023 it reached $ 1,435,785.61. This drastic increase may be related to better life expectancy, which can lead to chronic diseases in the Brazilian population, such as systemic arterial hypertension, the main risk factor for AD [20].
Comparing this expenditure by demographic region, it can be seen that the Southeast allocated almost half of the expenditure on the procedure (48.92%), being the most economically developed region in the country, followed by the South with 25.9% of the expenditure. This raises the question of whether the high amount of spending is due to the greater allocation of government resources for health in the more developed regions or the greater frequency of diagnosis in the south and southeast. Furthermore, the population differences between the regions and the demographic concentration in the Southeast over the others may also have an influence on the amounts spent.
When analyzing spending on professional and hospital services, there is a significant discrepancy between them. Of the total spending in the time series analyzed, 62.12% went to hospital services, while only 37.17% went to professional services. This pattern is consistent in all regions of the country. These figures are a reflection of the high cost of surgical materials in the procedure, such as endoprostheses. A study published in the Brazilian Vascular Journal revealed that vascular surgery with an endoprosthesis can cost health insurance plans around $60000 [22]. However, this data may also be due to the undervaluation of health professionals in Brazilian society.
CONCLUSION
The study of the Brazilian reality in terms of hospitalizations and deaths from AD shows a concentration of figures in the Southeast region of the country. This region led the way in the total number of hospitalizations and deaths and accounted for almost half of the expenditure on the correction procedure. The difference in infrastructure, quality of notification, population size and access to healthcare between the South and Southeast regions and the other Brazilian regions are possible factors that led to the discrepancies shown in the results. The Northeast, which was the only region to show a predominance of elective procedures compared to emergency procedures, had the lowest mortality rate, but comparatively did not have more early diagnoses. That said, there is a need for equal public policies throughout Brazil for early diagnosis and more elective treatment of AD. Limitations may have compromised the analysis of the data collected: failure to distinguish between aneurysms caused by AD and classic AD with its variants (ulcer, intramural hematoma or dissection), since they are clinical entities with different behaviors, which is a flaw in the DataSUS data registry. The data is not recorded by health professionals, but by administrative technicians who have no expertise in the pathology.
The values recorded in the system are not corrected for inflation and the underreporting of data, especially diagnoses that are not carried out properly, cannot be disregarded.
REFERENCES
- Gardner ED, Gray DJ, O’rahilly R. Anatomy: regional study of the human body. Rio de Janeiro: Guanabara Koogan, 1988.
- Dinato FJ, Ribeiro Dias R, Abrahão Hajjar L. Aortic Dissection: Clinical and Surgical Management. Revista da SOCESP. 2018; 28: 260-266.
- Velasco TI, Souza RA, Marino HP, Marchini LO, Alencar JCG de, Brandao RAN,et al. Medicina de emergência: abordagem prática, 16th edition. Barueri, Manole. 2022.
- De Souza FM, Araujo JVG, Costa ACB, Camargos BP, Carvalho MKS, Calzavara GP, De Oliveira LGM, De Andrade Júnior J, Portella VN. Acute aortic dissection - epidemiological and pathophysiological aspects and therapeutic management. Brazilian Journal of Development. 2023; 9: 12379-12391.
- de Souza FM, Araujo JVG, Costa ACB, Camargos BP, Carvalho MKS, Calzavara GP, et al. Acute aortic dissection - epidemiologic and pathophysiologic aspects and therapeutic management. Brazilian Journal of Development. 2023; 9: 12379-12391.]
- Loscalzo J, Fauci AS, Kasper DL, et al. Harrison’s Internal Medicine. [Porto Alegre]: Grupo A, 2024. E-book. ISBN 9786558040231.
- Côrtes JVR, Martins AP, Santos JVB, Azevedo AAT, Hernandes NNF, Hernandes Júnior PR. Xx Simpósio Internacional De Ciências Integradas Da Unaerp -Campus Guarujá Avaliação Do Procedimento De Dissecção Da Aorta Toraco-Abdominal No Município Do Rio De Janeiro.
- Cooper M, Hicks C, Ratchford EV, Salameh MJ, Malas M. Diagnosis and treatment of uncomplicated type B aortic dissection. Vasc Med. 2016; 21: 547-552.
- Sullivan PR, Wolfson AB, Leckey RD, Burke JL. Diagnosis of Acute Thoracic Aortic Dissection in the Emergency Department. 2000; 18: 46-50.
- Huu A Le, Preventza O. Endovascular Repair of Acute Type B Thoracic Aortic Dissection. Ann Cardiothorac Surg. 2021; 10: 793-800.
- Augoustides JG. Commentary: Acute type B aortic dissection: Navigating new horizons. J Thorac Cardiovasc Surg. 2022; 164: 1066- 1067.
- Ana Nery is the national leader in endovascular abdominal aortic aneurysm/dissection repair procedures - Hospital Ana Nery. 2024.
- Novero ER, Metzger PB, Obregon J, Marco VLA, de Rossi FH, Moreira SM, et al. Endovascular treatment of thoracic aortic diseases: analysis of the results of one center. Radiologia Brasileira. 2012; 45: 251-258.
- IBGE - Brazilian Institute of Geography and Statistics. Demographic Census 2022: population and households: first results. Rio de Janeiro: IBGE, 2023.
- Report shows that the number of adults with hypertension has increased by 3.7% in 15years in Brazil.
- IBGE. Census 2022: number of people aged 65 or over grew by 57.4% in 12 years.
- Malta DC, Goncalves RPF, Machado IE, Freitas MIF, Azeredo C, Szwarcwald CL. Prevalence of arterial hypertension according to different diagnostic criteria, National Health Survey. Rev Bras Epidemiol. 2018; 21: e180021.
- In SUS and the private network, inequality in access to diagnostic equipment.
- Velasco IT, Neto RAB, Souza HP, Marino LO, Marchini JFM, Alencar JCG . Medicina de emergência: abordagem prática, 16th edition. Barueri. Manole. 2019.
- Northeast is first in the queue of elective surgeries paralyzed in SUS.
- Mendonça CT, Oliveira LG, José FF, da Silva ES, Santos JG, Junior SF, et al. Endovascular treatment of abdominal aortic aneurysms: initial experience. J Vasc Bras. 2009; 8: 7-11.
- Cebes. The devaluation of public health professionals. 2024.









































































































































{kind=link}