Gamma Variant of SARS Cov2: Increase in the Number of Contaminants and Lethality and the Start of Vaccination
- 1. Medical School of the University of Ribeirão Preto, Brazil
- 2. UNAERP, Avenue Costábile Romano, Ribeirão Preto, Brazil
Abstract
Introduction: In January/2020 China notified the appearance of a new coronavirus- SARS- CoV-2- that causes the coronavirus disease (COVID-19) that can evolve with the Severe Acute Respiratory Syndrome. Due to its rapid spread throughout the world, the World Health Organization decreed in March 2020 that it is a pandemic. Variants are classified into Variant of Concern (VOC), Variants of Interest, and Variant of High Consequence. This classification aims at a better study, evaluation and monitoring of these variants. The Brazilian Gamma variant (identified by 20J501Y.V3 or B.1.1.28 or 20 J/501Y.v1 and VOC-202101/02) was detected by RT-PCR examination in four travelers who returned to Japan after a trip to Manaus (state capital of Amazonas- Brazil) on January 2, 2021. This variant is related to the second wave of COVID-19 contagion in Manaus that created chaos in the city’s fragile health system. Objective: Evaluate the increase in the number of cases and deaths resulting from the Gamma Variant in the city of Ribeirão Preto Material and Method: Ribeirão Preto has an estimated population of 720,116 people. Data provided by the Health Department of Ribeirão Preto in the New Coronavirus Bulletin (COVID-19) were analyzed. Period A- First wave of contamination: June-August 2020- SARS- CoV-2- first strain/ rudimentary virus/ wild form. Period B- Second wave of contamination: March-May 2021- Gamma (P.1) variant. Results: Increased number of positive cases in period B. Lethality- increased lethality in period B (2021), predominance in men. As for age, in period B there was a predominance of deaths in younger people. Conclusion: Without a rapid plan for mass vaccination in the world, universal mask wearing, and social distancing to contain the spread of COVID-19 cases, we will be subject to the emergence of new variants.
Keywords
• Gamma Variant
• SARS CoV2
• COVID- 19
• Lethality
• Deaths
Citation
Daniel RF, Farias M, Almeida ALN, Geleilete TJM, Roncato P, et al. (2024) Gamma Variant of SARS Cov2: Increase in the Number of Con- taminants and Lethality and the Start of Vaccination. Clin Res Infect Dis 8(2): 1067.
INTRODUCTION
In January/2020 China notified the appearance of a new coronavirus- SARS- CoV-2- that causes the coronavirus disease (COVID-19) that can evolve with the Severe Acute Respiratory Syndrome. Due to its rapid spread throughout the world, the World Health Organization decreed in March 2020 that it is a pandemic. SARS-CoV-2 (genome: Wuhan-Hu-1/ MN908947.3)
[1] is a positive-stranded envelope mRNA virus and uses the protein spike to enter the target cell. It can mutate, a fact inherent to viruses, and can generate new variants, recombinants, insertion, and deletion within the genome [2-8]. In a world plagued by a new disease, the possibility of the emergence of new variants is a major cause for concern. These variants can have a direct impact on the transmissibility and virulence of COVID-19, directly impacting the health system and devastating the economy of countries. These variants can cause reinfection and escape the immunization generated by the vaccines used at the time. Regarding reinfections, a survey carried out with blood donors in the city of Manaus showed that 1 in 6 people infected with the coronavirus in the first wave of contagion (rudimentary virus) was reinfected with the Gamma (P.1) variant [3-8].
According to the worldometers website, there are 270,238,909 cases and 5,320,878 deaths in the world caused by SARS-Cov-2; in Brazil, there are 22,188,179 cases and 616,859 deaths (12/12/2021) [9]. Variants are classified into Variant of Concern (VOC), Variants of Interest, and Variant of High Consequence. This classification aims at a better study, evaluation and monitoring of these variants. The Variants of Concern (VOC) tracked are B.1.1.7 or Alpha (United Kingdom), B.1.351 or Beta (South Africa), B.1.1.28 or Gamma (Japan/Brazil), and B.1.617.2 or Delta (India) [3,5,10].
The Brazilian Gamma variant (identified by 20J501Y.V3 or B.1.1.28 or 20 J/501Y.v1 and VOC-202101/02) was detected by RT-PCR examination in four travelers who returned to Japan after a trip to Manaus (state capital of Amazonas- Brazil) on January 2, 2021. This variant was recognized as an emerging lineage from Manaus that has 21 lineage-defining mutations and 10 synapomorphic mutations in the Spike protein (L18F, T20N, P26S, D138Y, R190S, K417T, E484K, N501Y, T1027I) [5,11]. This variant is related to the second wave of COVID-19 contagion in Manaus that led to chaos in the city’s fragile healthcare system. [4,12] According to Sharun et al, the Gamma (P.1) variant is related to the rapid increase in cases of COVID-19 and a greater number of hospitalizations, and the consequent number of deaths [3].
In Ribeirão Preto, a city placed in São Paulo state, Brazil, from March 2021, there was a significant increase in cases of COVID-19, taking the health system to its maximum capacity for occupation. According to an experiment carried out at Instituto Adolfo Lutz, 83.33% positivity was identified for the Gamma variant in samples carried out between March and April 2021, thus placing Ribeirão Preto in first place in the state regarding the presence of the Gamma (P.1) variant. [13,14] In parallel with the increase in the number of infected individuals, immunization of the population was started at the end of January 2021, with the vaccine Coronavac (Butantan/ Sinovac) and Vaxzevria (AstraZeneca/ Fiocruz) [15].
MATERIAL AND METHOD
Ribeirão Preto has an estimated population of 720,116 people [16]. Data provided by the Health Department of Ribeirão Preto in the New Coronavirus Bulletin (COVID-19) were analyzed [17]. A descriptive and cross-sectional study was carried out in 2 distinct periods of the pandemic. These periods were defined as they are considered the beginning of the first and second wave of contamination of COVID-19 in Ribeirão Preto. So far, these were the worst moments of the Covid-19 pandemic, with a large number of infected people and deaths.
- Period A- First wave of contamination: June – August 2020- SARS- CoV-2- first strain/ rudimentary virus/ wild form.
- Period B- Second wave of contamination: March-May 2021- Gamma (P.1) variant.
For data analysis, Software R version 3.0.2 RStudio (version 1.1.463-2019-2018) was used. The statistical method used was the 2-Sample Test for equality of proportions with continuity correction. The variables analyzed in the determined periods were: number of positive cases and deaths by COVID- 19, lethality, incidence by sex, deaths by age group, mortality by age group after the start of the vaccine in 2021, mortality in the general population, and mortality.
RESULTS
The periods with the highest number of cases and deaths were compared, namely period A (2020) and period B (2021). From March 2020 to September 2021, 2,933 deaths were reported in Ribeirão Preto; 1,044 were notified in 2020. During 2020 there were 41,980 positive cases and in the period January September/2021 68,316 positive cases [17] (Figure 1).
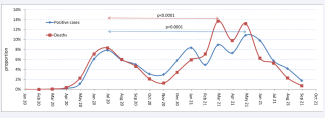
Figure 1: Evolution of the COVID pandemic- 19 positive cases and the number of deaths in the period from April/20 to September/21. The evaluated periods were highlighted in the graph (ellipse), being considered the peaks of the 2 waves. Period A (2020) rudimentary virus and Period B (2021) Gamma variant. The number of confirmed cases and deaths in Period B was higher than in Period A.
The start of vaccination for people over the age of 90 was on 02/08/2021 and for the population over the age of 85 on 02/25/2021 [18]. In March, the Gamma variant was identified in positive cases of COVID-19 [19]. In the period from 03/17/2021 to 03/21/2021, a new lockdown was decreed in Ribeirão Preto, due to the situation classified as pre-collapse of the health system due to the severity of COVID-19 cases [20].
Lethality (the measure of disease severity, calculated by dividing the number of deaths from COVID-19 by the number of cases of the same disease)- Comparison between periods A (2020) and B (2021) showed a greater lethality of COVID-19 in the period with the predominance of the Gamma variant (2021) (Figure 2).
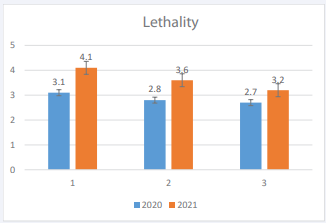
Figure 2: COVID- 19 lethality in 2020 and 2021: 1 June, 2020 and March, 2021, 2 July, 2020 and April 2021, 3-August, 2020 and May, 2021.
The first wave of contamination began in June 2020 and the second wave, with the Gamma variant, in March 2021. Comparisons in the two periods (2020- 2021) were made based on the beginning of the wave of contamination. The comparison between both groups according to sex showed that male sex was predominant in both periods, as illustrated in (Figure 3).
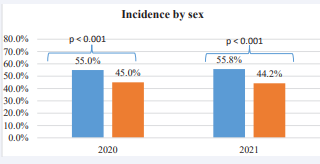
Figure 3: Incidence of covid 19 in men and women. The predominance of male patients.
In Period A, there was a predominance of percentual deaths in patients over 70 years of age (657). In Period B, however, there was an inversion of the age group, with a predominance of percentual deaths in patients under 70 years of age. In absolute numbers in 2020, there were 1,044 deaths; nonetheless, with the predominance of Gamma variant in 9 months, there were 1,877 deaths (Figure 4).
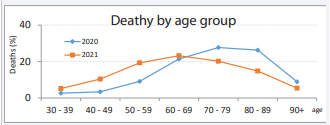
Figure 4: In 2020, there was a predominance of death in the elderly (over 70 years), but with the start of vaccination in 2021 there was a marked decrease in deaths in this age group, with an increase in the younger age groups (50-70 years) not covered by vaccination in the period evaluated.
The start of vaccination took place in February/ 2021 with older patients and health professionals. With the advance of vaccination, the elderly are no longer the age group most affected by COVID-19. The incidence of deaths in the elderly population decreased with the start of vaccination (Figure 5) illustrate these data.
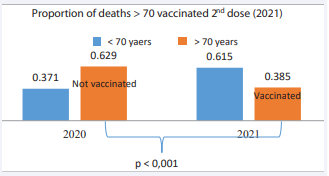
Figure 5: Proportion of deaths after the second dose of vaccine.
Despite the start of vaccination in January 2021 and in the population aged over 90 years on 02/08/2021, there was an increase in mortality from COVID-19 in 2021 at ages not covered in the vaccination schedule. In May 2021, vaccination was made available to people aged 50-59 with comorbidities. The Gamma Variant is characterized by greater transmissibility and severity of cases, as depicted in (Figure 6).
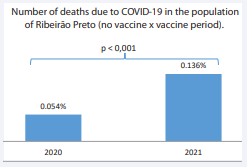
Figure 6: Mortality in the no vaccine versus vaccine period. In 2020, with the circulation of the rudimentary virus, mortality was lower when compared to 2021 with the Gamma variant. Result based on the total number of deaths in the period without vaccination and in the period with vaccination (vaccination by age and morbidity) - periods evaluated: 2020- A- First wave of contamination: June – August 2020- SARS- CoV-2- first strain/ rudimentary virus/ wild form./ 2021- BSecond wave of contamination: March-May 2021- Gamma (P.1) variant.
DISCUSSION
At the beginning of the pandemic, before the confirmation of the first case, Ribeirão Preto decreed a lockdown in March 2020 so that the city’s health service could prepare itself for cases of COVID-19. With the reduction in the number of people circulating in the city, hospitals were able to prepare for the admissions of patients with COVID-19 (reduction in admissions of multiple trauma patients, cancellation of elective surgeries, etc.). Even with the increase in the number of beds in the Intensive Care Unit in July/2020, the hospitalization capacity reached its limit. The peak of transmissibility, mortality and lethality in 2020 was in the period evaluated (June-August/20). In the following months, there was a gradual decrease in new confirmed cases (Figure 1), hospitalizations, and deaths from COVID-19. The percentage of deaths in the population of Ribeirão Preto during 2020 was 0.054% (Figure 6), a period in which there was no availability of vaccines.
In January 2021 Manaus had an explosion of COVID-19 cases; hospitals and Intensive Care Units collapsed with overcrowding. Due to the chaos in the healthcare system, several patients were transferred to other states. These patient transfers were performed without special security precautions. The Gamma variant quickly reached other states in the country and became the predominant variant throughout the national territory, starting the new wave of COVID-19 contagion. This variant has mutations in the spike protein (K417Y. E484K and N501Y) associated with the increased binding to the human ACE2 (Angiotensin-Converting Enzyme 2) receptor [21].
It is a variant at least twice more transmissible than the parental line. With effective reproduction (Re) of 2.2 and transmission rate in the order of 1.4 to 2.2 times higher than the parental line, evasion of immunity of 25-61%. with the probability of reinfection (28%) and transmissibility 2.6 times higher than the original strain (rudimentary virus or wild form) [5,21]. Furthermore, it may show reduced neutralization by monoclonal antibody therapies, convalescent serum and post-vaccination sera [22,23]. In addition, Naveca et al., in a study performed with upper respiratory tract secretion in patients contaminated with Gamma variant, identified a viral load ten times higher than those contaminated with non-Gamma in adult patients (18-59 years) [24].
In Ribeirão Preto, the Gamma variant (P.1) quickly became predominant during the second wave of contagion [13-25] that started at the end of February. The significant increase in cases in the period evaluated when compared to the first wave is compatible with the higher transmissibility rate of this variant (2.6x), when compared to the wild form. In South America, this variant was responsible for about 40% of cases in February 2021 [21-26].
At the beginning of 2021, the city was practical with its normal activities, as there had been a significant decrease in the number of hospitalizations and deaths. With the explosion of cases (Gamma Variant) rapidly in late February and early March, the municipal health system did not have time to make the necessary adjustments beforehand. Concomitantly with this explosion of cases, the elderly and health professionals began to be vaccinated. The vaccines available at that time were: Coronavac- (Butantan/ Sinovac) and Vaxzevria (AstraZeneca-Fiocruz). The interval between doses for full immunization ranged from 21 to 28 days (Coronavac) to 12 weeks (Vaxzevria) [27]. There was a “rejuvenation” of the population affected by COVID-19, since this variant is more virulent in young patients [11,12], as shown in this investigation.
According to the Fiocruz Bulletin, deaths in the population between 18 and 45 years old grew 193%, rising from 13.1% to 35.5% in Intensive Care Units between February and March 2021 [12-17]. Ribeirão Preto Period B (when the variant Gamma was predominant) was responsible for 42% (1.061 deaths) of the total number of deaths from the entire pandemic period to date (March 2020-May 2021) when compared to period A (25%-629 Deaths). There was a 3.4-fold increase in the number of deaths in the 17-50 age group in period B (117 deaths) when compared to period A (34 deaths). These data demonstrate the transmissibility of the Gamma variant and the change in the age group of infected patients and the number of deaths (Figure 1) [11].
This reversal of deaths in the age group can be explained by vaccination. The two vaccines used in this period (Coronavac and Vaxzevria) are considered effective against SARS-CoV2 infection, effectively reducing the rate of hospitalization, admission to Intensive Care Units, and death in elderly patients. The lethality among hospitalized patients between 20-39 years was 2.7 times compared to the first wave [5]. In Ribeirão Preto, case lethality reached 4.1 in March 2021 (period B) and in June 2020 (period A) the lethality was 3.1%, thus demonstrating the higher lethality of the Gamma variant.
According to updated data (06/14/2024) from the Brazilian Ministry of Health, accumulated data regarding COVID-19: 38,823,186 confirmed cases, 712,349 deaths and a mortality of 339.0 / 100 thousand inhabitants. Regarding vaccination: 82.2% of the population received the full vaccination schedule and 58.1% received the booster dose [28,29].
CONCLUSION
Without a rapid plan for mass vaccination in the world, universal mask wearing, and social distancing to contain the spread of COVID-19 cases, we will be subject to the emergence of new variants. We have seen that despite vaccination in a large part of the population in several countries, the increase in the number of cases followed by new admissions has increased significantly again. Our study shows that the Gamma variant resulted in a high number of positive cases and deaths in comparison to those found with the wild variant; this took the health system to its maximum capacity and beyond its capacity at times.
REFERENCES
- Cella E, Benedetti F, Fabris S, Borsetti A, Pezzuto A, Ciotti M, et al . SARS- CoV-2 Lineages and Sub-Lineages Circulating Worldwide: A Dynamic Overview. Chemotherapy. 2021; 66: 3-7. doi: 10.1159/000515340. Epub 2021 Mar 18. PMID: 33735881; PMCID: PMC8089399.
- Janik E, Niemcewicz M, Podogrocki M, Majsterek I, Bijak M. The Emerging Concern and Interest SARS-CoV-2 Variants. Pathogens. 2021; 10: 633. doi: 10.3390/pathogens10060633. PMID: 34064143; PMCID: PMC8224338.
- Sharun K, Tiwari R, Dhama K, Emran TB, Rabaan AA, Al Mutair A. Emerging SARS-CoV-2 variants: impact on vaccine efficacy and neutralizing antibodies. Hum Vaccin Immunother. 2021; 17: 3491- 3494. doi: 10.1080/21645515.2021.1923350. Epub 2021 Jun 23. PMID: 34161189; PMCID: PMC8240541.
- Naveca FG, Nascimento V, de Souza VC, Corado AL, Nascimento F, Silva G, et al. COVID-19 in Amazonas, Brazil, was driven by the persistence of endemic lineages and P.1 emergence. Nat Med. 2021; 27: 1230-1238. doi: 10.1038/s41591-021-01378-7. Epub 2021 May 25. PMID: 34035535.
- Marquitti FMD, Coutinho RM, Ferreira LS, Borges ME, Portella TP, Silva RLPD, et al. Brazil in the face of new SARS-CoV-2 variants: emergencies and challenges in public health. Rev Bras Epidemiol. 2021; 24: e210022. English, Portuguese. doi: 10.1590/1980- 549720210022. PMID: 34105594.
- Taylor L. Covid-19: Researchers find higher than expected reinfections with P.1 variant among the Brazilian Amazon. BMJ. 2021; 373: n1353. doi: 10.1136/bmj.n1353. PMID: 34035005.
- Freitas ARR, Beckedorff O, Cavalcanti LPG, Siqueira AM, Castro AB, Costa CF, et al. The emergence of novel SARS-CoV-2 variant P.1 in Amazonas (Brazil) was temporally associated with a change in the age and gender profile of COVID-19 mortality: A population based ecological study. Lancet Reg Health Am. 2021; 1: 100021.
- Hoffmann M, Arora P, Groß R, Seidel A, Hörnich BF, Hahn AS, et al. SARS-CoV-2 variants B.1.351 and P.1 escape from neutralizing antibodies. Cell. 2021; 184: 2384-2393.e12. doi: 10.1016/j. cell.2021.03.036. Epub 2021 Mar 20. PMID: 33794143; PMCID: PMC7980144.
- Resende PC, Gräf T, Paixão ACD, Appolinario L, Lopes RS, Mendonça ACDF, et al. A Potential SARS-CoV-2 Variant of Interest (VOI) Harboring Mutation E484K in the Spike Protein Was Identified within Lineage B.1.1.33 Circulating in Brazil. Viruses. 2021; 13(5): 724. doi: 10.3390/v13050724. PMID: 33919314; PMCID: PMC8143327.
- Instituto Adolfo Lutz atualiza cenário da variante P.4 no Estado. Governo do Estado de São Paulo- Secretaria do Estado de Saúde. 2024.
- Secretaria Municipal de Saúde – Ribeirão Preto/ SP. 2024.
- Cerqueira-Silva T, Oliveira VA, Boaventura VS, Pescarini JM, Júnior JB, Machado TM, et al. Influence of age on the effectiveness and duration of protection of Vaxzevria and CoronaVac vaccines: A population- based study. Lancet Reg Health Am. 2022; 6: 100154. doi: 10.1016/j. lana.2021.100154. Epub 2021 Dec 22. PMID: 34957437; PMCID: PMC8692070.
- IBGE estimula população de Ribeirão Preto em 720.116 pessoas. 2024.
- Boehm E, Kronig I, Neher RA, Eckerle I, Vetter P, Kaiser L; Geneva Centre for Emerging Viral Diseases. Novel SARS-CoV-2 variants: the pandemics within the pandemic. Clin Microbiol Infect. 2021; 27: 1109-1117. doi: 10.1016/j.cmi.2021.05.022. Epub 2021 May 17. PMID: 34015535; PMCID: PMC8127517.
- Ong DSY, Koeleman JGM, Vaessen N, Breijer S, Paltansing S, de Man P. Rapid screening method for the detection of SARS-CoV-2 variants of concern. J Clin Virol. 2021; 141: 104903. doi: 10.1016/j. jcv.2021.104903. Epub 2021 Jun 19. PMID: 34182300; PMCID: PMC8213512.
- Kerr LRFS, Kendall C, Almeida RLF, Ichihara MY, Aquino EML, Silva AAMD, et al. COVID-19 in northeast Brazil: first year of the pandemic and uncertainties to come. Rev Saude Publica. 2021; 55: 35. doi: 10.11606/s1518-8787.2021055003728. PMID: 34105604; PMCID: PMC8139846.
- Boletim do Observatório Covid-19 Fiocruz - semanas 10 e 11 de 2021.
- Naveca FG, Nascimento V, de Souza VC, Corado AL, Nascimento F, Silva G, et al. COVID-19 in Amazonas, Brazil, was driven by the persistence of endemic lineages and P.1 emergence. Nat Med. 2021; 27(7): 1230-1238. doi: 10.1038/s41591-021-01378-7. Epub 2021 May 25. PMID: 34035535.
- Covid- 19 Coronavirus Pandemic. 2024.
- Tracking SARS- CoV-2 Variants. 2024.
- Faria NR, Mellan TA, Whittaker C, Claro IM, Candido DDS, Mishra S, et al. Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil. Science. 2021; 372: 815-821. doi: 10.1126/science. abh2644. Epub 2021 Apr 14. PMID: 33853970; PMCID: PMC8139423.
- Nota técnica: Análise de efetividade da vacinação da Covid-19 no Brasil para casos de hospitalização ou óbito. 2021.
- Cascella M, Rajnik M, Aleem A, Napoli DR. Features, Evaluation, and Treatment of Coronavirus (COVID-19). 2023.
- Silva SJRD, Pena L. Collapse of the public health system and the emergence of new variants during the second wave of the COVID-19 pandemic in Brazil. One Health. 2021; 13: 100287. doi: 10.1016/j. onehlt.2021.100287. Epub 2021 Jun 29. PMID: 34222607; PMCID: PMC8240439.
- Coronavirus/ Brasil. Painel Coronavirus.
- Números da Vacinação contra COVID-19 no Brasil. Laboratório de Estudos Espaciais do Centro de Pesquisas Computacionais, Rice University.
- Documento Técnico Campanha de Vacinação Contra a COVID-19. 2024.
- Plano Municipal de Saude de Ribeirão Preto- 2022- 2025.
- Ribeirão Preto vai fechar até padarias e mercados para conter Covid. 2024.









































































































































{kind=link}