Innovative Research and Translational Application of Autologous Tissue Stem Cell Ectopic Transplantation in the Treatment of Vitiligo
- 1. Department of Dermatology, Tianjin Perennial General Hospital, China
- 2. University of New South Wales, Australia
- 3. Department of Dermatology, Nanhai Renshu International Skin Hospital (Hainan) Co., LTD, China
Abstract
Objective: Currently, surgery is the most effective method for treating vitiligo. It involves transplanting epidermal-derived melanocytes to treat vitiligo, but it requires skin harvesting, abrasion, and grafting, resulting in significant damage, pain, and color differences, which causes patients to reject this type of surgery. Therefore, exploring the ectopic transplantation of autologous tissue (hair follicle outer root sheath) melanocyte stem cells for the treatment of vitiligo is of great clinical significance.
Methods: For a long time, many scholars have mistakenly believed that transplanting single hair follicles transfers the melanocyte stem cells from within the hair follicles to the epidermis in the treatment of vitiligo.
Results: Transplantation of single hair follicles for treating vitiligo only achieves spot repigmentation and cannot cure vitiligo at all.
Conclusion: This study not only confirms that the transplantation of single hair follicles for treating vitiligo indeed involves the transfer of melanocytes from the scalp of the hair follicles, but also successfully achieves ectopic transplantation of melanocyte stem cells from autologous tissue (hair follicle outer root sheath), marking a significant breakthrough in the efficacy of vitiligo treatment.
Keywords: Vitiligo; Ectopic Transplantation; Stem Cells; Follicle Melanocyte Stem Cells; Single Hair Follicles
Abbreviations: McSCs: Melanocyte Stem Cells; ORS: Oral Rehydration Salts; AMMC: Amelanotic Melanocyte; MC: Melanocyte; FUE: Circumferential Drill Extraction; PUVA: Psoralen and Ultraviolet A.
Introduction
In the past 30 years, many scholars have mistakenly believed that single hair follicle transplantation could transfer melanocyte stem cells from the follicles into the skin, yet clinical applications have been in vain; particularly, many reports have been misleading, leading countless clinicians to repeatedly suffer the bitter consequences of spot repigmentation. Recent clinical studies in this study have shown that the melanocytes in the hair follicle scalp of the hair follicle are actually transplanted into the epidermis, rather than the Melanocyte Stem Cells (McSCs) in the hair follicle. The myth of single hair follicle transplantation for treating vitiligo has severely misled clinicians regarding the application of hair follicle melanocyte stem cells, delaying the development of the interdisciplinary field between hair medicine and dermatology.
The origin and cognitive misunderstandings of single hair follicle transplantation in the treatment of vitiligo
In 1998, Na et al., treated 21 patients with vitiligo using a single hair follicle transplant [1]. First, a piece of spindle-shaped skin about 1 cm long is cut from the patient’s postoccipital scalp. After washing with saline, cut with a scalpel into several segments, each of which is divided into many individual hairs. Then, a hair transplant device is used to transplant each hair to the skin receiving area, and the entire hair follicle is transplanted to hair areas such as the eyebrows and scalp. For patients with smooth skin, the lower 1/3 of the hair follicle should be removed and fixed for 1 week before implantation. In 15 of these cases, within 2 to 8 weeks, “melanocytes in the hair follicles began to migrate to the epidermis”, and pigment regeneration began to appear around the hair follicles of the transplanted hair. However, only 1 in 4 patients with hairless vitiligo has pigment regeneration around the hair follicle. Many scholars mistakenly believe that by activating the proliferation of non-pigmented melanocytes (AMMCs) in the outer hair root sheath, their upward migration to the nearby epidermis results in the formation of pigment islands around the hair follicles [2,3].
Basic research on hair follicle melanocyte stem cells in the treatment of vitiligo
In 2002, Nishimura et al. found for the first time that Melanocyte Stem Cells (McSCs) at a certain stage of differentiation are widely distributed in the growing outer hair root sheath (ORS) [4], and have the characteristics of self-renewal, proliferation and differentiation. McSCs act as a reservoir of Melanocytes (MCs) for skin repigmentation in vitiligo. Although the basic research of McSCs is very mature, the use of McSCs in the treatment of vitiligo has not yet achieved clinical translation.
The treatment of vitiligo with a single hair follicle interferes with the basic research of clinical translation
For nearly 30 years, many scholars and clinicians have been treating vitiligo based on Na and its methods, but they have not been able to achieve satisfactory results, and they have not recognized the erroneous theories that lead to continuous failures such as Na. In fact, single follicle transplantation is the movement of hair follicle units, and the transplanted MC comes from the scalp epidermis where the hair follicle connects, and the McSCs in the hair follicle can only enter the scalp epidermis attached to the hair follicle and cannot enter the vitiligo epidermis, and it is the MC in the scalp that enters the epidermis. Thus, it can only form a punctate complex. Despite the rapid development of hair medicine in recent years, many scholars have been misled by Na and have a superficial view of McSCs, and there is no reason to believe that McSCs cannot be achieved by single hair follicle transplantation, which seriously affects the development of interdisciplinarity and leads to the failure to transform the basic research results of McSCs.
The reason why McSC in single hair follicle transplanted hair follicles cannot enter the vitiligo epidermis
Through clinical studies, our team found evidence that McSC in the hair follicles of single hair follicle transplantation for vitiligo cannot enter the epidermis: Evidence 1: Scalp vitiligo is the most common vitiligo in clinical practice, and the scalp of vitiligo patients turns white first, and then the hair turns white. This clinical phenomenon illustrates that scalp vitiligo does not occur if McSCs in a single hair follicle can enter the epidermis. In scalp vitiligo, vitiligo is still formed at follicle densities of up to 100 plants/cm2, indicating that McSCs in hair follicles are unable to enter the vitiligo-affected area (Figure 1). Similarly, vitiligo in long hairy areas such as eyebrows, eyelashes, beard, and vulva also indicates that McSCs in hair follicles cannot enter the vitiligo-affected area. Evidence 2, “When 21 vitiligo patients in the Na study were treated with single hair follicle transplantation, the lower 1/3 of the hair follicle should be removed before hair follicle implantation for patients with smooth skin. After surgery, the MC in the hair of 15 patients began to migrate to the epidermis within 2-8 weeks, and the pigment around the transplanted hair follicles began to regenerate and expand to 2-10 mm in diameter within 1 year.” Doctors who are engaged in hair transplantation know that the hair follicles are immediately inactivated after removing 1/3 of the hair follicles, and it is nonsense that the McSCs in the inactivated hair follicles enter the affected vitiligo; The punctate pattern formed by the scalp MC is exactly the same as the effect of punctate epidermal grafting. According to 3, clinical studies have found that the affected area of vitiligo does not produce punctate discoloration after removing the epidermis above the hair follicle funnel, which further confirms that the melanocytes in the hair follicle cannot enter the epidermis after removing the scalp around the hair follicle of a single plant. In summary, the essence of single hair follicle transplantation in the treatment of vitiligo is to transplant MC from the scalp (Figure 2).
Summary
Although it has been more than 20 years since McSCs were discovered in hair follicles, they have not been ectopic transplanted into the skin, let alone implanted into the epidermis. Many scholars have tried to extract the hair follicle carina and culture the McSCs in vitro for the treatment of vitiligo, but they have failed, so in vitro culture and activation of McSCs in ORS is an effective way to obtain hair follicle McSCs. In this study, it is concluded that the transformation of melanocyte stem cells in autologous tissues (extrafollicular hair root sheath) into MC in another organ (skin) requires three conditions: First, the resting state of McSCs in ORS must be activated to reach a functional state in order to be transformed into mature MC. Second, it is only in intact ORS that McSCs can proliferate and transform into mature MCs. Last but not least, intact follicular ORS must be fully implanted in a specific layer of the skin for McSCs to achieve the proliferation of mature MCs into the epidermis. Since the above three conditions cannot be met by single follicle transplantation, McSCs of ORS cannot enter the epidermis. Based on this, our team invented the “technical method for the treatment of vitiligo by follicle melanocyte stem cell transplantation” [5]. It has not only obtained Chinese invention patents, but also obtained international PCT patents, and applied for invention patents in the United States, the European Union, Japan, South Korea and Thailand. This patented technology successfully transplanted melanocyte stem cells from the external hair root sheath to vitiligo, completed the transformation of McSCs from the laboratory to the clinic, and realized the ectopic transplantation of stem cells between autologous xenogeneic tissues.
Figure 1
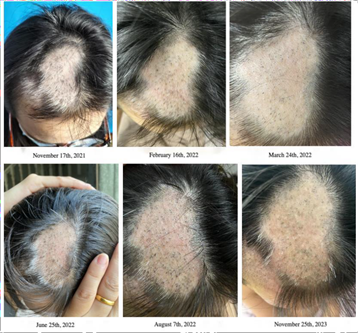
Figure 1: Results observed after the second ectopic microorgan stem cell transplantation procedure, showing significant repigmentation after six months
Figure 2

Figure 2-1 Figure 2-2
Figure 2: Single hair follicle transplantation for vitiligo. After the operation: the epidermis of the hair follicle is above the affected area, and the above part of the hair follicle funnel is not inserted into the skin at all (Figure2-1). 8 months after surgery: the epidermis above the infundibular part of the hair follicle is above the affected area, and there is no dot color (Figure 2-2).
References
- Na GY, Seo SK, Choi SK. Single hair grafting for the treatment of vitiligo. J Am Acad Dermatol. 1998; 38: 580-584.
- Yu HS. Melanocyte destruction and repigmentation in vitiligo: a model for nerve cell damage and regrowth. J Biomed Sci. 2002; 9: 564-573.
- Matz H, Tur E. Vitiligo. Curr Probl Dermatol. 2007; 35: 78-102.
- Nishimura EK, Jordan SA, Oshima H. Dominant role of the niche in melanocyte stem-cell fate determination. Nature. 2002; 416: 854-860.
- Liu JW. Technical method for treating leucoderma based on hair follicle melanocyte stem cell transplantation. China. 2021.









































































































































{kind=link}