Pulmonary Edema Ex Vacuo or Unilateral Shock Lung: A Case Report
- 1. Pastor Escatín, Irene, Genaro
Keyword
• Edema Ex Vacuo
• Re-Expansion Pulmonary Edema (REPE)
• Pulmonary Collapse
Citations
Navil AM (2022) Pulmonary Edema Ex Vacuo or Unilateral Shock Lung: A Case Report. JSM Burns Trauma 6(1): 1049.
SUMMARY
Pulmonary edema is a rare but potentially life-threatening iatrogenic complication after treatment through therapeutic thoracentesis of a collapsed lung due to a hydro- or pneumothorax. We present a case of a 25-years male, without any pathological antecedents, who went to our emergency services with dyspnoea, tachypnea, and hypoxemia. The final diagnosis made after a clinical examination and chest X-ray showed a complete the collapse of the right lung due to spontaneous pneumothorax (Figure 1a)
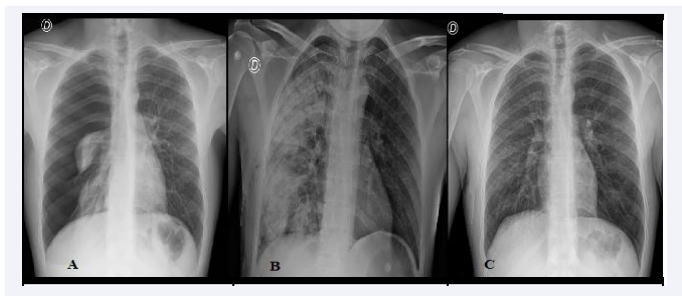
Figure 1 a: Chest X-ray showing a complete collapse of the right lung due to spontaneous pneumothorax
b: Chest X-ray revealing an alveolar infiltrate of the entire right lung field
c: Chest X-ray showing the patient treatment with supplemental oxygen therapy and methylprednisolone
The chest drainage was carried out, because of pneumothorax. About 30 minutes after pleural drainages tube placement, the patient started with thorathic pain and severe cough and was kept with Hypoxemia. We take inmediatly a control chest X-ray that revealed an alveolar infiltrate of the entire right lung field, wich was interpreted as re-expansion pulmonary edema (REPE) (Figure 1b).
We were treated successfully with supplemental oxygen therapy and methylprednisolone for 5 days, after the treatment the patient became asymptomatic and presented the following Chest X-ray (Figure 1c).
CONCLUSIÓN
Re-expansion pulmonary edema (REPE) or unilateral shock lung is an infrequent clinical entity, with a low incidence rate. It can cause worsening in patients with a tension pneumothorax after placement of the pleural tube drainage.
The suspected diagnosis is made with an anamnesis and clinical history and requires confirmation by performing a chest X-ray. The treatment consists of bolus administration of methylprednisolone and supplemental oxygen, with complete resolution of symptomatology the in the majority of patients.









































































































































{kind=link}