Unusual Penetrating Mandibular Injury By A Cut-Off Wheel
- 1. Department of Université De Sousse-Tunisie, Tunisia
- 2. Department of Université De Sousse-Faculté De Médecine De Sousse-Tunisie, Tunisia
Abstract
Penetration wounds on the face caused by foreign bodies other than bullets are rare in today’s life. Most of the adult penetrating injuries reported in the literature were due to industrial accidents, criminal assaults or self-injury. We present an unusual case of a man who suffered a fracture of his lower jaw due to a broken cut- off wheel. This kind of injuries was rare in todays life because of the Poor workplace safety still existing in our country.
Keywords
Facial Injury, Mandibular Fracture, Cut-off whee
CITATION
Mabrouk H, Rejeb MB (2023) Unusual Penetrating Mandibular Injury By A Cut-Off Wheel. JSM Burns Trauma 7(1): 1050.
CASE REPORT
A 54-year-old man received a severe penetrating facial injury caused by a cutting wheel that broke during work and pierced his face (Figure 1B).
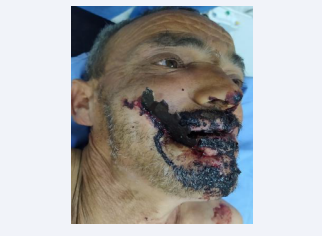
Figure 1B: A 54-year-old man with a big Fragment of the cut-off wheel protruding on his face.
The Wheel-cut was armed with iron teeth, and revolving towards each other,it is a power tool used for cutting hard materials, ceramic tile, metal (Figure 1A).

Figure 1A: Retained fragment of the cut-off wheel after removing from the face.
He was taken to the emergency department of Sahloul University Hospital, Sousse, Tunisia. Physical examination, shows a big Fragment of the cut-off wheel protrudes on the right side of the face from the upper cheek to the middle of the chin. The neurological examination was normal and the patient was conscious during the exam. A standard radiographic X-Ray with frontal and profile views was done quickly in the emergency department showed a metallic foriegn body anchroched to the mandible (Figure 1D). The history for the injury conclude to work accident.
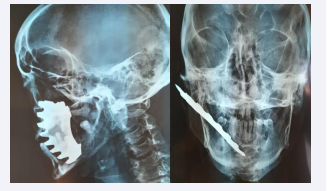
Figure 1D: X-ray of the face with frontal and profile views revealing a broken wheel fragments anchored in the bone.
In the operating room the metal body was removed without significant bleeding before intubation but after the administration of Propofol, Etomidate, and ketamine which are used to induce general anesthesia.
During the operation, we confirmed that there were no major vessel injuries and no lesion of the mental nerve, we discovered a displaced mandibular fracture. We preferred a transmucosal incisions made in the buccal sulcus instead of direct access via the wound , to protect the mental nerve also the osteosynthetic material should ideally be covred by muscle, such as the buccinator or mentalis muscle (Figure 1C).

Figure 1C: Showing that there are no major vascular structure injuries
We have used arch bars for maxillo-mandibular fixation than we reduce the fracture using a 2.0 mm plate with 3 screws 2 mm × 6 mm length monocortical in the upper border of the mandible to avoid damage of the roots of the teeth and 2.0 mm plate with 4 screws 2 mm × 6 mm length monocortical in the lower border , plates to be placed 5 mm at least (Figure 1E).

Figure 1E: Open reduction of the mandibular fracture using two titanuim manipulates.
The lip laceration was closed in 3 layers after good debridement and irrigation with normal saline. Appropriate wound care and early use of antibiotics prevent infection from a highly contaminated wound. Tetanus toxoid with tetanus immunoglobulin was given in the first 24 hours .The patient was discharged home after 3 days. Three week after, the patient came in the clinic with good improvement in oral function. He does not have a neurological déficits, and his mastication was painful only during the first week after surgery. The follow up was good without any complication.
DISCUSSION
The complexity of penetrating head and neck wounds necessitates consideration of the depth of invasion and involvement of major vascular structures, ocular structures, skull and nasopharynx, and maxillary sinuses [1,2,6].There is usually enough time to complete physical examinations and preoperative evaluations to determine vascular status and examine surrounding structures in these types of injuries. When foreign bodies located outside the wound are moving freely, attempts to remove the object should not be made in the emergency department because massive bleeding may ensue [1,2,7].
Gentle immobilization in the operating room of the impaling object is an important step for preventing further damage when the foreign material is inserted [2]. Early anticipation of potential airway obstruction is essential for patient survival and successful surgery.
In the emergency department, the surgeon and anesthesiologist should discuss how and when to intubate. We recommend not delaying intubation if there is a potential risk for patients with penetrating trauma that could compromise the airway [4-6].
In our case, a patient with mandibular fracture required nasal intubation for occlusional arrangement. Plain film and A computerized radiography of the face is a basic requirement because radiographs can confirm the location, size, shape, and number of foreign bodies , especially ones made of metal [7]. Free movement of the foreign object is also important if it is firmly anchored in the bone because can cause a massive bleeding. For the reduction of this type of fracture Titanium was preferred than resorbable materials that can cause infection [5,7].
Psychiatric consultation is always required for patients with impalement injuries. In addition, administration of appropriate medications during acute stages of patient distress can prevent persistent symptoms or disorders [3,5].
CONCLUSION
The treatment of penetrating craniofacial wounds requires methodical approach to immediate assessment and management life-threatening injuries. The location of the foreign body predicts possible injury and potential risks of removal. A workplace safety can help employers reduce the high cost of work-related injuries.








































































































































{kind=link}