A Pilot Assessment of Cryopreserved Umbilical Tissue Allograft as a Surgical Wrap for Improved Rehabilitative Outcomes in Peroneus Brevis Tendon Repair
- 1. Macomb Foot, 9001 15 Mile Road A. Sterling Heights, USA
- 2. Osiris Therapeutics, Inc., 7015 Albert Einstein Drive, USA
Abstract
Surgical tendon repairs of the lower extremity are frequently associated with post-operative risks resulting in poor patient outcomes. Initially, pain levels contribute to extended lengths of post-operative rehabilitation while development of tissue adhesions and fibrosis limit long-term functionality through reduced range of motion. Several surgical methods describing incorporation of various augmentative graft materials in tendon repair exist. However, reports demonstrating technique and both short- and long-term patient outcomes are lacking. Recently, an advance in tissue-preservation technology has led to the commercialization of human placental allografts. Of these available allogeneic biomaterials, the components found in human placental membranes may provide anti-inflammatory, antimicrobial, anti-adhesive and antifibrotic properties to benefit surgical outcomes.
Here, the authors introduce and technically describe the use of a viable cryopreserved umbilical tissue (vCUT) (Stravix®, Osiris Therapeutics, Inc., Columbia, MD) as a complementary surgical wrap in primary tendon repair, with particular focus on the peroneus brevis, and report pilot study outcomes for post-operative pain, inflammation and scarring in 5 Achilles, peroneus brevis and tibialis posterior tendon repair cases using vCUT. Patients were evaluated by Visual Analog Scale (VAS) for pain both pre- and post-operatively. Transition times to CAM boot and normal shoewear with return to previous levels of activity were measured. All patients reported minimal to no pain at 1 week post-operatively and resumed previous levels of activity within 6-8 weeks, a result typically not observed until 3-6 months for historical control patients managed without adjunct vCUT in the literature. The results offer promise to improve rehabilitative outcomes for tendon repair patients.
Keywords
• Peroneal tendon
• Rupture
• Viable cryopreserved umbilical tissue
• Allograft
• Stravix®
Citation
Sundblad KW, Tassis EK (2017) A Pilot Assessment of Cryopreserved Umbilical Tissue Allograft as a Surgical Wrap for Improved Rehabilitative Outcomes in Peroneus Brevis Tendon Repair. JSM Foot Ankle 2(5): 1041
ABBREVIATIONS
vCUT: Viable Cryopreserved Umbilical Tissue; CAM: Controlled Ankle Movement; VAS: Visual Analog Scale
INTRODUCTION
Peroneal tendon injuries are associated with debilitating complications such as chronic ankle instability, foot deformities, chronic pain, and bone spurs thus [1], prompt diagnosis and repair are crucial for good clinical outcomes. In recent years, several techniques and surgical protocol algorithms for tendon repair have been proposed, some incorporating allograft use [1- 3]. Cases of acellular allograft use in peroneal tendon repair have been presented in the literature [4-6], yet reports on the use or outcomes of viable cellular allografts in tendon repair are scarce.
Recent advances in tissue-preservation technology have led to the development and commercialization of placental tissues, one being viable cryopreserved umbilical tissue (vCUT) (Stravix®, Osiris Therapeutics, Inc., Columbia, MD). Fresh umbilical tissues are known to contain a rich extracellular matrix, growth factors, and viable cells, including mesenchymal stem cells. vCUT’s unique cryopreservation method including storage at -80° C enables the umbilical tissues to retain the naturally occurring components and the inherent anti-inflammatory, antifibrotic, analgesic, and antimicrobial properties of fresh placental tissues [7].
Briefly, this report details a novel surgical tendon repair technique incorporating the use of vCUT as a pliable and conforming tendon wrap in peroneus brevis repair. However, previous assessment of the authors’ use of this augmentation technique has proven it safe, applicable, and beneficial in the surgical repair of all lower extremity tendons, including the Achilles, peroneal and tibialis. The authors believe that the utilization of vCUT in tendon repair supports the body’s natural tissue repair process, minimizing risks for post-operative infection, adhesion formation, and fibrosis that correlate with pain reduction and faster recovery. Pilot study outcomes are presented for evaluation alongside the detailed technical tip.
MATERIALS AND METHODS
Umbilical tissue allograft preparation
vCUT is delivered by the manufacturer aseptically cryopreserved in a plastic jar. To facilitate thawing at the time of required use, room temperature sterile normal saline is added to the plastic container to submerge the vCUT. Typically after 3-10 minutes, ice crystals are no longer visible in the jar and preparation is considered complete. Additional tissue rinsing is not required. When ready, the pliable vCUT can be removed from the jar with forceps (Figure 1) and conformed to the desired surgical site.

Figure 1 A 3 x 6 centimeter pliable and conforming viable cryo preserved umbilical tissue allograft (vCUT) post thawing, ready for application at the site of surgical tendon repair.
Surgical technique
The following surgical technique is described in detail for a peroneus brevis repair. (It is important to note, that vCUT can be applied in a similar fashion for all tendon repairs, including and not limited to Achilles, peroneal and tibialis repairs).
The patient is placed on the operating room table in the supine position. Following induction of intravenous and local anesthesia, the affected foot is prepped and draped in the usual sterile fashion. The affected extremity is elevated approximately 60 degrees above the horizontal plane at which point a pneumatic ankle tourniquet is applied. Following exsanguination by Martin esmarch bandage, the tourniquet is rapidly inflated to 250 mmHg.
Attention is then directed towards the patient’s lateral ankle at the malleolar region where approximately 8 cm modified Ollier curved incision is created along the course of the peroneal tendon posterior to lateral malleolus extending distally. The incision is deepened via sharp and blunt dissection to the level of subcutaneous tissues. All venous tributaries are electrocauterized as necessary. Care is taken to avoid trauma to the sural nerve. Dissection is deepened until the superior peroneal retinaculum is identified and incised. At this time, the sheath of the peroneus brevis and longus tendons is identified. The tendons are palpated proximally as far as the incision allows. The tendon sheath is incised in a longitudinal fashion along the course of the tendon utilizing a sharp #15 blade.
The peroneus brevis tendon is isolated and the proximal and distal extents to the tear are identified. The portion of the tendon containing the tear is tubularized utilizing a #2 absorbable suture (Vicryl®, Ethicon, Inc., NJ) in a continuous running suture type fashion (Figure 2A). The area is flushed with copious amounts of sterile normal saline solution. At this time, a 3 x 6 cm vCUT graft is prepared and wrapped circumferentially around the tendon (Figure 2B) and sutured in place utilizing a #3 absorbable suture (Vicryl®, Ethicon, Inc., NJ).
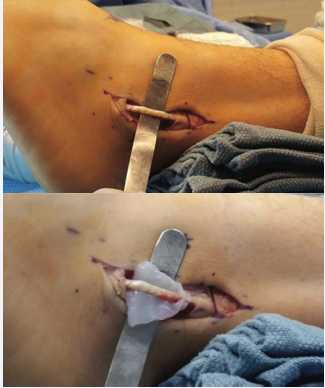
Figure 2 In the case of a peroneal tendon repair, the (A) repaired tubularized tendon is isolated and (B) a 3 x 6 centimeter vCUT is passed under the repaired tendon, and beginning with the proximal corners, is circumferentially sutured around the tendon of interest.
Attention is then directed towards closure. A #3 absorbable suture (Vicryl®, Ethicon, Inc., NJ), is used to close the peroneal tendon sheath and superior peroneal retinaculum in a continuous running suture type fashion. #4 absorbable retention sutures (Vicryl®, Ethicon, Inc., NJ) are used to re-approximate the subcutaneous tissues in a simple interrupted suture type fashion. Here, a second piece of 3 x 6 cm vCUT is laid along the incision site (Figure 3) prior to skin closure with a #5 absorbable suture (Vicryl®, Ethicon, Inc., NJ) in a horizontal mattress suture type fashion.

Figure 3 In a peroneal tendon repair, a second piece of 3 x 6 centimeter viable Cryopreserved umbilical tissue (vCUT) laid along the incision site prior to skin closure.
Prior to bandaging, a 10mL injection consisting of 0.5% Marcaine plain is instilled proximal to the surgical sites. Attention is then directed towards bandaging consisting of non-adherent layer (Adaptic®, Acelity, TX), 4x4s, kling bandage roll, and kerlix gauze bandage roll applied in a mildly compressive nature. The pneumatic ankle tourniquet is rapidly deflated and instantaneous capillary refill is noted on the patient’s digits. A below knee cast is applied to the lower extremity with the foot in dorsiflexion and slight eversion. The patient is discharged home with instructions to follow-up in 1 week.
Pilot study design
A pilot assessment was conducted on patients who underwent surgical tendon repair at Macomb Foot, Ankle and Wound Care under the same surgeon. A total of 5 cases were included in this study (1 male; 4 females; age range 19-58 years; average 41 years). Affected tendons were as follows: 2 Achilles ruptures, 2 peroneus brevis ruptures and 1 tibialis posterior rupture. All patients had failed previous conservative therapy consisting of rest, activity modification and physical therapy for 6 months. Post-operative protocol for all included non-weight bearing with weekly cast changes for 3 weeks. Patients were subsequently transitioned to a controlled ankle movement (CAM) boot with initiation of physical therapy. Patients were encouraged to transition to normal shoe and ambulate as tolerated. Patient pain scores both pre- and post-operative, using the Visual Analog Scale (VAS), and time to transition to CAM boot and normal shoe were recorded and analyzed.
RESULTS AND DISCUSSION
Patient demographics and clinical outcomes are shown in Table 1. All 5 patients demonstrated a reduction of pain (average pre-operative pain 8/10; average 1-week post-operative pain 1.4/10). Reduction in post-operative pain was accompanied by visual inspection of minimal swelling at 1- week post-operatively and rapid reduction of scarring within 6-8 weeks. Average transition time to CAM boot was 3.2 weeks. Rapidly resuming pre-injury activities, such as a weight-bearing without pain, was also noteworthy with the average return-to-activity time in normal shoe at 5.6 ± 1.3 weeks, which compares favorably to 15.2 ± 1.7 weeks previously reported for chronic tendon injuries repaired with acellular dermal allograft.8 The 2 Achilles tendon repair cases showed faster recovery by the ability to graduate from a non-weight-bearing cast to a CAM boot at 2-3 weeks post-operatively versus 4-6 weeks reported in the literature for open repair of Achilles [9,10]. The 2 peroneal cases demonstrated quick transition to CAM boot at 3-4 weeks and ambulation in normal shoe at 6 weeks, versus the reported median immobilization values of 6 weeks after primary repair, 6.3 weeks post grafting, and 8 weeks post tendon end-to-end suturing, presented in a review of 49 analyzed studies in total [3]. No post-operative complications, including infection, were observed in any patients. All patients were followed for an average of 23.15 months (range 15.75-25.5 months) after the surgery. All remained pain free with full range of motion comparable to pre-injury status, allowing patients to regain previous functional status and 100% muscle strength.
Several surgical procedures to repair tendon ruptures are reported in the literature, yet no clear consensus on the best technique or rehabilitative protocol exists [1,3,11]. Based on the severity of peroneal tendon rupture (e.g., partial-thickness split versus full-thickness split), treatment protocols vary from conservative treatment including rest, ice, compression, and elevation to invasive or percutaneous surgical repair.12 While surgical repair has proven to be effective, it has been reported that as many as 25.4% of patients struggle with post-operative complications such as pain, and 17.4% experience persistent swelling [2]. The optimal surgical technique would be one that prevents complications effectively and allows patients to resume normal activities in a reduced amount of time.
The benefits of placental tissue use in surgery were initially described in ophthalmology in 1940 by DeRoth, and since then, more reports have surfaced [13-16]. Specifically in the operative reconstruction of ocular surfaces, placental tissues have been shown to assist in minimizing post-operative inflammation, pain, and adhesion formation [14,16]. In response to such results seen in ophthalmology, Liu et al. suggested that exploration of amniotic membrane application in other medical fields is warranted to explore potential benefit [15]. Placental membrane use has since expanded to fields such as orthopedic surgery as an adhesion barrier and maxillofacial surgery for root coverage and reconstruction of temporomandibular joint ankyloses due to its antifibrotic properties [17,18]. In current literature, few cases of acellular allograft use in tendon repair exist, yet no reports detailing the surgical technique and outcomes with cellular placental allografts are available [19,20].
The previously cited outcomes in ophthalmology, orthopedic, and maxillofacial surgery have been consistent with the results the authors are seeing in tendon repairs incorporating viable placental tissue. To date, the authors have incorporated vCUT as a tendon wrap in over 30 cases. Documented patient outcomes have consistently included decreased pain and reduced inflammation and fibrosis, which have ultimately led to expedited recovery to a pre-injury status.
Despite such initially promising patient outcomes observed with utilization of vCUT in tendon repair, the authors recognize the limitations of this retrospective pilot evaluation. A prospective randomized study, comparing vCUT utilization in surgical tendon repair to non-augmented controls is necessary. Additional values such as daily narcotic use and functional score evaluations both pre- and post-vCUT utilization in surgical tendon repair will offer additional insight. As a follow-up to this pilot study, the next step in the authors’ research is to confirm benefits of vCUT as a tendon wrap augmenting surgical tendon repair in a prospective case study. These findings are currently underway and plan to be reported on in a follow up publication.
CONCLUSION
Briefly, a surgical technique using viable cryopreserved umbilical tissue allograft in peroneus brevis tendon repair is described. The authors have observed that the surgical technique is simple and safe for patients and results in favorable outcomes over historically observed controls, including minimal inflammation, pain, adhesion formation, and scarring with quick return of patients to pre-injury activities and lifestyle.
Table 1: Tendon Repair Patient and Clinical Outcomes Summary.
| Case | Age (Sex) | Patient History | Tendon Repaired | Pre-Op Pain Score (VAS) | Post-Op Pain at 1- Week (VAS) | Time to CAM Boot | Time to Normal Shoe | Adverse Events |
| 1 | 44 (F) | None | Achilles | 8/10 | 0/10 | 3 weeks | 4 weeks | None |
| 2 | 58 (F) | None | Achilles | 7/10 | 2/10 | 3 weeks | 4 weeks | None |
| 3 | 19 (M) | Vertigo | Peroneal | 8/10 | 1/10 | 4 weeks | 6 weeks | None |
| 4 | 47 (F) | Diabetes | Peroneal | 8/10 | 4/10 | 3 weeks | 6 weeks | None |
| 5 | 38 (F) | Left Side Drop Foot | Tibialis Posterior | 9/10 | 0/10 | 4 weeks | 8 weeks | None |
| Average | 8/10 | 1.4/10 | 3.2 weeks | 5.6 weeks | ||||
| Abbreviations: M: Male; F: Female; Pre-Op: Pre-Operative; Post-Op: Post-Operative; VAS: Visual Analog Scale; CAM: Controlled Ankle Movement | ||||||||
ACKNOWLEDGEMENTS
The authors would like to thank Alla Danilkovitch for her editorial support.
CONFLICT OF INTEREST
EKT is employed by Osiris Therapeutics, Inc. (“Osiris”), Department of Medical Affairs. KWS is currently a consultant and is on the speakers’ bureau for Osiris; however, KWS received no compensation or incentives for the publication of this case.









































































































































{kind=link}