A Prospective Randomised Study of Ponseti Casting by a Physiotherapist and a Paediatric Orthopaedic Surgeon
- 1. Department of Trauma & Orthopedics, King’s College Hospital, England
- 2. Department of Orthopedic Surgery, Imperial College London, England
- 3. Department of Trauma and Orthopaedics, St Peter’s Hospital, UK
Abstract
The Ponseti method is widely accepted and practiced, giving reliably good long-term results. There are a number of studies showing the benefits of a physiotherapy led Ponseti service with outcomes similar to a consultant led service. We present our prospective randomized series comparing a physiotherapy led Ponseti service with a standard orthopaedic surgeon led series.
14 infants with bilateral CTEV were randomized into two groups. Each infant had one foot treated by a physiotherapist and the other foot treated by an Orthopedic Surgeon, using the Ponseti technique. Both groups had a median pre manipulation Pirani score of 6.
All patients were followed up for a minimum of 18 months and the results demonstrated no significant difference in the post-treatment Pirani scores (p=0.35) and no significant difference in the success rate of the Ponseti technique (p=0.77) between the two groups.
This study demonstrates the value of a Physiotherapy led Ponseti service in the management of CTEV. Although overall supervision by a paediatric orthopaedic surgeon is still necessary, our results suggest that manipulation and casting can be safely delegated to adequately trained physiotherapists. This may free up valuable financial and medical manpower resources.
Keywords
• Pediatric orthopedics
• Congenital talipes equinovarus
• Management
Citation
Akhbari P, Jaggard M, Hillier V, Saini A, Lahoti O (2016) A Prospective Randomised Study of Ponseti Casting by a Physiotherapist and a Paediatric Orthopaedic Surgeon. JSM Foot Ankle 1(2): 1008.
ABBREVIATIONS
CTEV: Congenital Talipes Equinovarus
INTRODUCTION
Congenital talipes equinovarus (CTEV) is a common complex three-dimensional deformity of the foot with an incidence of 1.2 per 1000 live births in Europe [1]. Over recent years, there has been a dramatic change in the management of this condition with a progression towards Ponseti casting [2], which has been demonstrated to be reproducible [3,4] and successful in up to 98% of patients [5]. However, previous studies have suggested the key to obtaining good to excellent results requires a precise understanding of the method of manipulation, casting and the use of orthotic supports [6,7].
Traditionally, serial casting was often managed by a Paediatric orthopaedic consultant assisted by any combination of junior doctors and other health care professionals. However, the Uganda and Malawi Club Foot Project demonstrates how the Ponseti technique has been successfully introduced in developing countries where medical professionals are in short supply [8].
Two recent studies have demonstrated good results when the Ponseti method is performed by a trained physiotherapist in a developed country [9,10]. Both studies were a prospective case series. We present the first prospective randomized study comparing the results of Ponseti serial casting by a trained physiotherapist on one foot and a paediatric orthopaedic surgeon on the other foot, in the same child.
MATERIALS AND METHODS
Sixteen consecutive infants with bilateral CTEV were randomized, using block randomization, to have manipulation and serial casting of one foot by a paediatric orthopaedic surgeon and the other foot by a senior physiotherapist with over three years experience in Ponseti treatment. All infants with bilateral CTEV were included. There were no exclusion criteria. Fifteen infants had idiopathic CTEV. One infant had an underlying diagnosis of arthrogryposis.
Our protocol included initial general assessment by the same orthopaedic surgeon along with the physiotherapist in all cases. The families were counselled regarding the treatment protocol and informed consent was obtained prior to the commencement of treatment in every case. All feet were scored using the Pirani clubfoot score [11], which was the primary outcome measure. After appropriate consent, the feet were randomized to have one foot manipulated by the physiotherapist and the other by the senior author (OL). The median pre-manipulation Pirani score was 6 in both groups (range 4.5-6) and was assessed by the treating senior physiotherapist and orthopedic surgeon. Serial manipulation and casting was performed weekly whilst making sure that each child’s foot remained in the same group throughout the treatment period. Once the midfoot deformity had been corrected, any residual equinus was corrected by a percutaneous Achilles tenotomy by the orthopaedic surgeon as a day case procedure followed by casting for a further 2 weeks. All feet were put in boots and bars for 23.5 hours a day for three months and then for night and nap time until the age of 3 years. At follow up, physiotherapists not involved in the treatment or randomization assessed the outcome. These physiotherapists had 2-3 years of experience with Ponseti treatment.
A power analysis was performed using preliminary Ponseti score data. A Ponseti score difference of greater than 0.5 was selected for achieving significance at 95% confidence. This revealed that 14 pairs of feet or a sample size of 28 would be required (type I error, α=0.95, β=0.8). In order to compare 2 randomized groups of paired data from the same population, the Wilcoxon signed rank test was used. A p-value of 0.05 was applied.
RESULTS AND DISCUSSION
A total of 16 children were consecutively recruited into this study. The minimum follow-up set out in our criteria was 18 months and consequently, only 14 children were included in the final analysis (Table 1).
Table 1: Patientdemographics
| Number of feet: patients | 28:14 |
| Male: Female | 11:3 |
| Left: Right | 14:14 |
| Mean (range) age at enrolment (days) | 54 (16 – 261) |
| Mean (range) follow-up (months) | 38.4 (18 – 74) |
The mean follow-up was 38.4 months (18 – 74 months). The mean age at enrolment was 54 days (16-261 days). There were 11 males and 3 females. As all patients had bilateral deformities, the data was matched for age, sex, ethnicity and co-morbidities, thus reducing the number of confounding factors.
The median Pirani score at presentation was 6 in both groups. The mean number of plaster changes was nearly identical in both groups (4.4 in the physiotherapy group and 4.3 in the orthopaedic surgeon group). A total of 7 children needed bilateral tendo Achilles tenotomies (14 tenotomies – 7 in each group) (Table 2).
Table 2: Pirani scores, number of cast changes and tenotomies.
| Orthopaedic Surgeon group (OS) | Physiotherapy group (PT) | |
| Median (range) pre-manipulation Pirani score | 6 (4.5 – 6) | 6 (4.5 – 6) |
| Median (range) post-manipulationPirani score | 0 (0 – 1.5) | 0 (0 - 1.5) |
| Mean (range) no cast changes | 4.3 (4 – 7) | 4.4 (4 – 6) |
| Number of tenotomies | 7 | 7 |
| Abbreviations: OS: Orthopedic Surgeon; PT: Physiotherapist | ||
All tenotomies were performed by the orthopedic surgeon.
We assumed a null hypothesis of no difference in the treatment effect between the orthopaedic surgeon and the senior physiotherapist. The median improvement in the Pirani score was identical at 5.5 in both groups (p=0.7728) (Figure 1).
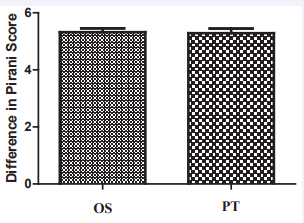
Figure 1: Improvement in the Pirani score based on the treatment provider (OS: Orthopaedic Surgeon, PT: Physiotherapist). Both groups demonstrate a median improvement in the Pirani score of 5.5 points (p=0.7728).
The median post-treatment Pirani score was zero in both groups (p=0.3458) (Figure 2).
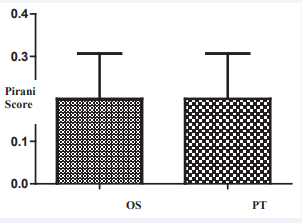
Figure 2: Post-treatment Pirani score in the 2 groups (OS: Orthopaedic Surgeon, PT: Physiotherapist). There was no significant difference in the median post-treatment Pirani score (p=0.3458).
The child with an underlying diagnosis of arthrogryposis showed limited improvement with serial casting. However, the pre and post-manipulation Pirani scores were identical in feet, 4.5 and 1.5 respectively. One foot in the physiotherapist treated group needed tibialis anterior transfer for dynamic supination. There was no recurrence of forefoot or hind foot deformities but the peronei were weak. Another child had bilateral recurrence requiring recasting. The child subsequently had a second tenotomy on the physiotherapist treated side, and a tibialis anterior transfer on the orthopaedic surgeon treated side due to a dynamic supination deformity that was unresponsive to physiotherapy.
The Ponseti method has consistently proven to give excellent results in correcting clubfeet. Studies have demonstrated that Ponseti serial casting is equally effective in the hands of a trained physiotherapist or a pediatricorthopedic surgeon [9,10]. However, none of the studies directly compared the efficacy of physician versus physiotherapist in the same child. We recruited bilateral CTEV cases consecutively irrespective of the etiology on the basis that the Ponseti method is the preferred treatment in all cases. In our series, one child proved to be a case of distal arthrogryposis, but was still managed according to the Ponseti method. The deformities remain corrected in both groups at a minimum of 18 months and beyond. These results support others in the literature, including two recent studies demonstrating the role of a physiotherapy led Ponseti service [9,10]. Shack and Eastwood demonstrated a 97.5% success rate in their physiotherapy-delivered service in a London teaching hospital [10]. Their study included 40 feet with idiopathic CTEV. Kampa et al., demonstrated a 95% success rate in their District General Hospital (DGH) physiotherapy-delivered service in a series of 39 feet with idiopathic CTEV [9].
In our series, not all patients had idiopathic club feet, and being a tertiary referral center, the deformities were more severe with a median pre-manipulation Pirani score of 6 in both groups. The mean number of casts per foot in both groups was in keeping with other studies [10,12,13]. Our tenotomy rates were equal in both groups and significantly lower than that quoted by Ponseti and some other series [3,4,7]. This may be a reflection of our small series.
This study has strength by demonstrating no difference in matched pair’s analysis with randomization and single blinding. Our study confirms no difference between an adequately trained physiotherapist and an orthopedic surgeon.
This study was limited to a single center. There was a narrow age range and although compliance with the postoperative protocols was not measured parents adhered to the use of foot abduction orthosis as per the Ponseti protocol. Larger multicenter studies with well-defined inclusion criteria are recommended to confirm that casting by a trained physiotherapist is equivalent to a pediatric orthopedic surgeon.
In the National Health Service (NHS), specialist medical time can be an expensive and scarce resource. Although overall supervision by a pediatric orthopedic surgeon is mandatory at the initial diagnostic stage and for surgical tenotomy, our results suggest that manipulation and casting can be safely delegated to adequately trained physiotherapists. This may free up valuable financial and medical manpower resources.
Our results at minimum of 18 months follow up demonstrate that a physiotherapy-led Ponseti service for the management of CTEV has a similar success rate to a traditional orthopaedic surgeon led service. This is in agreement with other studies who also feel that the Ponseti method is a skill that can be transferred to other health care professionals [8-10].
CONCLUSION
Our study demonstrated that a physiotherapy-led Ponseti service for the management of CTEV has a similar success rate to a traditional orthopaedic surgeon led service at a minimum of 18 months follow up. Manipulation and casting can be safely delegated to adequately trained physiotherapists, which may free up valuable financial and medical manpower resources.







































































































































{kind=link}