Diagnosing a double lesion Tarsal Tunnel Syndrome and Retrocalcaneal Bursitis-The Cyriax Approach
- 1. Department of Physical Therapy, Quinnipiac University, USA
Abstract
This case demonstrates the importance of obtaining a careful patient history followed by a meticulous selective tissue testing examination. The clinician must keep in mind that pain can be referred from a proximal location and that numerous tissues are located in the area where the symptoms are present. Therefore one cannot establish an accurate diagnosis by simply ascertaining from the patient the location of their symptoms. The late James Cyriax was a physician who practiced in England for 50 years up until his passing in 1985. He is acknowledged as the “Father of Orthopedic Medicine”.
His systematic approach to the examination and treatment of non-surgical orthopedic problems is invaluable to clinicians who are responsible for the care of patients with musculoskeletal lesions. The purpose of this paper is to summarize and demonstrate the Cyriax evaluation and treatment approach for a patient who is suffering with foot and ankle pathology in particular tarsal tunnel syndrome and retrocalcaneal bursitis.
Keywords
• Tarsal tunnel syndrome
• Retrocalcaneal bursitis
• Cyriax
• Ankle evaluation
Citation
Mirza SB, Woodman R (2016) Diagnosing a double lesion Tarsal Tunnel Syndrome and Retrocalcaneal Bursitis-The Cyriax Approach . JSM Foot Ankle 1(2): 1011.
INTRODUCTION
This case study demonstrates how the Cyriax approach can be useful in diagnosing tarsal tunnel syndrome and retrocalcaneal bursitis. Tarsal tunnel syndrome specifically refers to compression of the posterior tibial nerve as it passes through the tarsal tunnel producing a wide variety of symptoms. Symptoms due to entrapment of all or part of the posterior tibial nerve range from tingling or numbness in the foot, burning pain depending on the particular branch of the nerve involved to feeling tightness in the arch of the foot. Retrocalcaneal bursitis is the inflammation of the retrocalcaneal bursa which lies posterior to the calcaneus and anterior to the Achilles tendon causing pain at the posterior aspect of the heel. Soft tissue lesions are frequently treated by the physician and physical therapist.
- Two major problems in treating these types of lesions are identifying the tissue causing the pain and selecting the appropriate method of treatment. In recent years clinicians have become interested in the evaluation and treatment methods of soft tissue lesions developed by the late James Cyriax, a British physician. Cyriax developed a systematic approach for identifying the exact location of a soft tissue lesion [1]. The Cyriax approach requires the following attributes: A mastery of applied anatomy
- Knowledge of the non-surgical orthopedic conditions that can occur in each region of the body
- Verbal facility in obtaining an accurate history of the patient’s condition
- An understanding of how pain and paresthesia’s can refer symptoms
- Skill in the use of active motion testing for function, passive range of motion testing for non-contractile tissue and isometric resisted muscle testing to ascertain if a contractile tissue is the source of the pain or localized muscular weakness
CASE PRESENTATION
A 42 year old female patient complaining of right lower extremity discomfort was referred to physical therapy. The patient’s history included an insidious onset of pain at the heel and posterior medial aspect of the ankle. On the visual analogue scale, patient stated that her medial ankle and heel pain while ambulating was a 3/10. She also complained of tingling and numbness in the big toe. Patient stated that she felt better with the pads placed on either side of the Achilles tendon. According to the podiatrist the diagnosis was Achilles Tendinopathy. The patient was otherwise in good health indicating she had no other possible causes of neuropathy such as diabetes or alcoholism. She also complained of paresthesias at the posterior medial aspect of the right ankle. She found it difficult to perform her duties as a waitress. She also stated that walking increased her symptoms which were relieved with resting in the sitting position.
Ankle pain combined with paresthesias can be due to variety of possibilities such as a lumbar disc lesion, neurogenic intermittent claudication or a localized neuropraxia. It was therefore important to first clear the lumbar spine and sacroiliac joint as a potential source of her symptoms. Lumbar flexion, extension, left and right side flexion had no influence on her symptoms. It is unlikely that a problem at the sacroiliac joint would result in paresthesias, however, the Ostgaard posterior pelvic thrust Figure (1)
Figure 1: Ostgaard test.
was performed and it was negative. Unfortunately the patient’s diagnosis was not confirmed by electric diagnostic testing or diagnostic imaging. This would have been ideal. Frequently in out-patient orthopedics a soft tissue lesion is diagnosed based on the clinical findings. Diagnostic imaging such as MRI can be costly and neural conduction studies which can be both costly and painful are reserved for those cases where confounding clinical findings make a diagnosis difficult. A physical therapist can only justify requesting imaging when the diagnosis is unclear. The clinical picture and positive findings for this patient were consistent with the diagnosis of tarsal tunnel syndrome and retrocalcaneal bursitis. Typically in out-patient orthopedics a soft tissue lesion is diagnosed based on the clinical findings.
- 4.1. Positive findings for the patient’s symptoms included the following:Passive plantarflexion reproduced the posterior heel pain. This test can painfully pinch the retrocalcaneal bursa, and deep distal fibers of the Achilles tendon.
- Strong and painful resisted ankle plantarflexion which can occur with both Achilles tendinopathy and tarsal tunnel syndrome. The tibialis posterior passes through the same tunnel as the posterior tibial nerve. Contraction of the tibialis posterior muscle can compress the posterior tibial nerve.
- A positive Tinel’s sign posterior and distal to the medial malleolus with both a distal and proximal radiation of pain and paresthesia. The proximal radiation of the symptoms is known as Valleix Phenomenon [2].
- Painful palpation just anterior to Achilles tendon suggesting that the patient also had retrocalcaneal bursitis. There was no painful tenderness along the Achilles tendon.
- Passive dorsiflexion and eversion exacerbated the patient’s paresthesias. This is also known as the dorsiflexion-eversion test [2] (Figure 2).
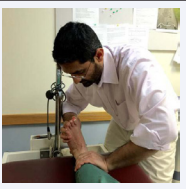
Figure 2: Ankle Dorsiflexion Eversion test
DISCUSSION
Frequently patients are diagnosed with two conditions for example; a patient with buttock pain may have both lumbar disc disease and osteoarthritis of the hip. Patients with osteoarthritis of the knee may also have a loose body at the knee. It has been the experience of these authors that double lesions do occur and must be identified to provide the complete and effective therapy. For the patient in this case study once the lumbar spine and sacroiliac joint were cleared as the source of the patient’s complaints the clinicians attention was then drawn to the foot and ankle.
Differential Diagnosis of Lower Leg and Ankle Problems
In the assessment of the lower quadrant, the examiner must keep in mind the importance of first clearing the lumbar spine and sacroiliac joint as a source of referred symptoms. Once the examiner has accomplished this, attention is then drawn to the leg. In order to appreciate the complexity of correctly diagnosing a patient with pain and/or paresthesia in the region of the lower leg and ankle the clinician must keep in mind that the lesion may lie in bone, nerve, ligament, joint capsule or contractile tissue. The purpose of this article is to demonstrate the Cyriax approach to differential diagnosis of a patient with lower leg pain and paresthesia. The selective tissue tension tests which are used in the Cyriax approach in the examination of the lower leg are listed in (Table 1).
Table 1: Cyriax Evaluation of Ankle and Forefoot [1].
| Movement | Tissue Tested |
| Passive dorsiflexion | Capsule and articular surface of ankle joint |
| Passive plantar flexion | Capsule and articular surface of ankle joint |
| Resistive dorsiflexion | Dorsiflexor muscle group |
| Resistive plantar flexion | Plantar flexor muscle group |
| Passive varus of talus | Inferior tibiofibular ligament |
| Passive eversion with plantar flexion | Deltoid ligament |
| Passive inversion with plantar flexion | Anterior fasciculus of lateral ligament |
| Resistive eversion | Peroneal muscle group |
| Resistive inversion with plantar flexion | Tibialis posterior |
| Passive eversion of talocalcaneal joint | Capsule of talocalcaneal joint |
| Passive inversion of talocalcaneal joint | Capsule of talocalcaneal joint |
| Passive dorsiflexion of midtarsal joint | Midtarsal capsule and ligaments |
| Passive plantar flexion of midtarsal joint | Midtarsal capsule and ligaments |
| Passive abduction of midtarsal joint | Midtarsal capsule and ligaments |
| Passive adduction of midtarsal joint | Midtarsal capsule and ligaments |
| Passive lateral rotation of midtarsal joint | Midtarsal capsule and ligaments |
| Passive medial rotation of midtarsal joint | Midtarsal capsule and ligaments |
In order to understand the clinical examination for tarsal tunnel syndrome and retrocalcaneal bursitis an understanding of the applied anatomy is imperative.
Anatomy of the Tarsal Tunnel
The posterior tibial nerve, a branch of the sciatic nerve is located in the deep compartment of the leg where it enters the calf between gastrocnemius and soleus muscles. Distally, the nerve passes through the tarsal tunnel. The tarsal tunnel is a fibro-osseous tunnel formed by medial malleolus, medial talus and calcaneus [2]. The flexor retinaculum forms the roof of the tarsal tunnel which is a fan shaped structure [3]. The posterior tibial nerve further eventually branches into medial and lateral plantar nerves as well as a calcaneal branch in the tarsal tunnel. According to Havel, “out of 68 dissections that he performed on cadavers, branching of the posterior tibial nerve occurred within the tunnel in 93% of the cadavers while branching occurred proximal to the tunnel in the rest of the cadavers.” The medial plantar nerve supplies sensation to medial plantar aspect of the foot which includes first, second, third and medial aspect of the fourth toe. The lateral plantar nerve supplies sensation to the lateral plantar aspect of the foot which includes the lateral aspect of the fourth and fifth toe. The posterior tibial nerve can become entrapped within the tarsal tunnel or within the fascial arcades of the abductor muscle itself [4]. The other contents of the tarsal tunnel include the posterior tibial vein and posterior tibial artery, posterior tibialis, flexor digitorum longus and flexor hallicus longus.
Etiology of tarsal tunnel syndrome
The ankle joint bears more weight per unit area than any other joint in the body; it is therefore more commonly prone to injury [5]. The posterior tibial nerve can become compressed due to intrinsic or extrinsic factors such as joint deformity, fat accumulation, fibrosis of retinaculum, ganglions, varicosities, lipomas etc [2,4]. This particular patient presented with calcaneal valgum and pain with resisted ankle plantar flexion. Any foot or ankle movement, including resisted plantarflexion, which either stretches or compresses the posterior tibial nerve will reproduce symptoms such as paresthesias and pain along the nerve distribution.
Symptoms of tarsal tunnel syndrome
Symptoms range from pain, tightness, and impending cramps along the arch of the foot to numbness and tingling in the foot depending on various activities. Some common complaints are night time pain which awakens the patient from their sleep due to nerve irritation [6]. Common clinical signs include a positive Tinel’s sign, weakness of the intrinsic muscles of the foot which is mild in nature. Weakness and atrophy is hard to detect in acute cases. It is easier to detect in chronic cases. Recent weight gain can also compress the nerve with excessive adipose tissue around the tarsal tunnel.
Treatment of tarsal tunnel syndrome
Treatment for tarsal tunnel syndrome typically consists of first trying a non-surgical approach. The physician may elect to inject the tunnel with a corticosteroid injection to relieve inflammation. Oral medicines such as non-steroid anti-inflammatory medication may be effective. Neurontin or Lyrica may work by suppressing central and peripheral neuronal firing [7]. Strengthening exercises for the tibialis posterior and the intrinsic foot muscles can improve the mechanics of the medial longitudinal arch and along with orthotics can help to control excessive pronation. Compressive stockings and a weight loss program can minimize compression within the tunnel. Neural mobilization exercises designed to improve mobility of the tibial nerve within the tunnel has been shown to be successful. A random control study consisting of 28 patients was performed by Kavlak and Uygar. One group was given exercise and supportive inserts and the other group was given exercise, supportive inserts and neural mobilization. Both groups showed improvement, but the group given neural mobilization showed a greater improvement in 2 point discrimination, and light touch with a diminished positive Tinel’s sign [8].
If conservative treatment is unsuccessful a tarsal tunnel release can be performed. Surgery may include releasing the superficial fascia overlying the Abductor Hallucis muscle belly and failure to do so may result in poor clinical outcomes [9]. Reade reports an 85% success rate for patients undergoing this surgery [10].
Anatomy of retrocalcaneal bursa
The Retrocalcaneal bursa lies between the calcaneus anteriorly and the Achilles tendon posteriorly (Figure 3).
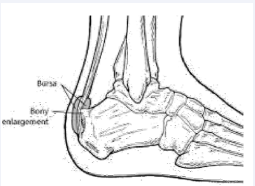
Figure 3: Retrocalcaneal bursa.
The synovial lining on the superior aspect separates the retrocalcaneal bursa from Achilles fat pad. The anterior wall of the bursa is cartilaginous and the posterior wall is tendinous. The bursa is filled with highly viscous fluid [11].
Etiology of retrocalcaneal bursitis: The retrocalcaneal bursa’s function is to decrease local pressure and friction by a (Figure 4).

Figure 4: Two finger squeeze test
sliding motion of a wedge shaped fat pad also known as Kager’s fat pad which is located adjacent to the calcaneus [12]. The fat pad is moved into the retrocalcaneal bursa during plantarflexion. This mechanism is impaired during inflammation as the bursa becomes filled with excessive fluid. Frequently, as result of the shoe’s irritation, an area of noticeable swelling is visible in this region of the foot. Haglund’s deformity which is a posterior-superior prominence of the calcaneus can also rub against the bursa resulting in inflammation. Tight fitting shoes may also contribute to the likelihood of compression between this prominence and the bursa. Occasionally Achilles tendinopathy and retrocalcaneal bursitis are both present [13].
Symptoms of retrocalcaneal bursitis: Pain anterior to the Achilles tendon and superior to the calcaneus is the hallmark of retrocalcaneal bursitis. The two finger squeeze test is usually positive with increased pain elicited from inflamed bursa. Retrocalcaneal bursitis is common in runners due to repetitive ankle dorsiflexion which stresses the bursa [11]. It has been shown that there is increased pressure in the retrocalcaneal bursa in patients presenting with retrocalcaneal bursitis. This increased pressure in the bursa may contribute to the increased likelihood of an Achilles tendon lesion [13].
Treatment of retrocalcaneal bursitis: Treatment options are ice, activity modification, orthotics, stretching the Achilles tendon and steroid injection in to the bursa. Ultrasound guided injection has proven to be effective to accurately guide the needle in to the bursa in order to avoid injecting the Achilles tendon itself which may adversely affect the biomechanical properties of Achilles tendon [11]. About 15-50% of patients suffering from chronic retrocalcaneal bursitis do not profit from conservative treatment and therefore require surgery which includes resection of the bursa or repair of anterior Achilles tendon in case of impingement lesions [13].
In conclusion this case study clearly illustrates the importance of obtaining an accurate patient history followed by performing a selective tissue tension examination can direct the clinician to an accurate diagnosis so that proper treatment can be administered.
Based upon the applied anatomy, and causes of tarsal tunnel syndrome and retrocalcaneal bursitis, the consequential signs and symptoms are understandable. Since the posterior tibial nerve traverses the medial side of the ankle it makes sense as to why the patient complained of neurological symptoms on the medial side of the ankle and big toe. Furthermore one can then understand why the patient had a positive Tinel’s sign and medial ankle pain with ankle eversion.
As previously mentioned the retrocalcaneal bursa lies in between the calcaneus anteriorly and the Achilles tendon posteriorly. Therefore, the posterior heel pain associated with retrocalcaneal bursitis was diminished when the pads were put on both the sides of Achilles tendon which would result in less contact with the counter of the shoe while walking. Furthermore it explains why passive plantarflexion will provoke pain and that the retrocalcaneal bursa can be painfully pinched just anterior to the Achilles tendon.







































































































































{kind=link}