Exceptional Case of Family Dupuytren in the Black
- 1. Aristide Le Dantec Hospital, Senegal
Citation
Abdoulaye BA, Abdoulaye Lindor DIOP, Rokia DIA, Mohamed Elhadji Khalifa FALL and Ndeye Fatou COULIBALY (2025) Exceptional Case of Family Dupuytren in the Black. JSM Foot Ankle 6(1): 1056.
INTRODUCTION
Once considered a disease that does not affect the black subject, today it is clearly shown that it affects all races. Dupuytren’s disease is a common benign fibroproliferative disease of the hand [1]. It is twice as common in men than in women, there are hereditary factors incriminated in its genesis. The global prevalence is between 2% and 42%, with a greater presence in northern Europe. Distribution depends on geography, ethnicity, gender and age [2]. The presence of a family history of Dupuytren’s disease leads to an 8% prevalence of 20% [3]. There is still a lot of shadow area of which the etiology (traumatic theory, the nervous theory, rheumatic theory, avitaminosis...) the beginning mode (nodule or cord, brutal or progressive),the distribution... [4]. Since 1974, a few cases among Afro-descendants have been described, but no family case has been reported [5]. Dupuytren’s disease is hereditary. The mode of transmission is variable, frequently autosomal dominant, rarely autosomal recessive or even mitochondrial with incomplete variable penetrance [6,7]. Some authors raise the possibility that this disease is linked to multiple genetic lesions or an association between polymorphisms of genes. Pathophysiology may result from a failure of healing with an increase in collagen III deposition compared to collagen I with hydroxylation and increased glycosylation of collagen [6]. Alterations in many copies of genes from chromosomes [5-17], were implicated in the genesis of this disease [7]. The disease of Dupuytren discovered for a very long time (1832) still remains poorly known despite numerous publications.We report an exceptional case of familial Dupuytren disease in two black Senegalese brothers, including a bilateral case involving Ladderhose disease. Our two patients are from a sibling of seven children, including five boys and two girls all alive. Both parents are alive and would be healthy. Two boys carry the disease. The interviewee examination found no impairment that could evoke a Dupuytren disease in either the ancestry or the extended collateral.
CLINICAL CASE
Our two patients are from a sibling of seven children, including five boys and two girls all alive. Both parents are alive and would be healthy. Two boys carry the disease. The interviewee examination found no impairment that could evoke a Dupuytren disease in either the ancestry or the extended collateral.
Clinical case no. 1
Mr A.D, 44 years old, right-handed, diver with an accident of decompression in 2015 having caused a bad caisson that was received for flessum of the fingers of the two hands predominant to right evolving for eight years.
To be examined:
Presence of a hard cord with a fixed palmar skin on the axis of the 4th and 5th fingers of the right hand.
Sign of prayer with both hands (Picture 2). Tubiana classification.
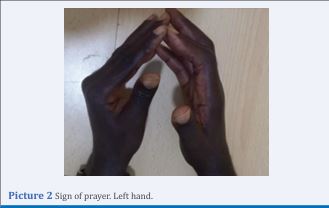
Picture 2 Sign of prayer. Left hand.
Right hand: (Picture 3)

Picture 3 Deformation of both hands.
D1: not achieved D2: stage 1
D3: Stage 1
D4: stage 3
D5: Stage 2
Left hand: (Picture 1 and 3).

Picture 1 Flessum of the fingers Left hand.
D1: not reached D2: Stage 2
D3: Stage 2 with nodules
D4: Stage 1
D5: Stage 2 with nodules
Hard, longitudinal, painless plantar cord in the left foot(Picture 4).

Picture 4 Ladderhose disease.
No penile deviation at rest or erection. Total reached
both hands and left foot.
Management consisted of an open aponeurotomy (Picture 5)

Picture 5 Open Aponeurotomy.
and the patient is currently progressing well.
Clinical case no. 2
Mr M.D, 35 years old right-handed, bricklayer by profession, who presents a deformation of the fifth finger of the right hand evolving for 3 years with a progressive aggravation. This patient has no particular terrain, he is neither alcoholic nor smoker, no notion of reported trauma.
To be examined:Flessum of the fifth finger of the right-hand classified stage II of Tubiana (Picture 6).

Picture 6 Flessum 5th finger right hand.
Elsewhere he has no touch of the other fingers, no touch of the feet, no touch penile. The patient is not being treated at this time and is working without discomfort.
DISCUSSION
Although the majority of cases reported by authors were adults, we found a few cases reported in children. Georgia et al. [8], report a case in a 10-year-old child. Already in 1832 the French anatomist Baron Guillaume Dupuytren discovered a case in a actually 06 years old but which was not confirmed histologically [9]. Since then,many isolated histologically confirmed cases have been reported in the literature. Huai Yuan Zheng and Juan Liu [10], report a congenital case in a 31-month-old infant whose histological characteristics were consistent with those of Dupuytren’s fibromatosis. Dupuytren disease affects all ages with a predominance in adults and males. Epidemiological studies show that it is a racial disease with a predominance among the Nords of Europe, which for a long time led to believe that this disease affected only these populations with heredity. Nowadays the data is changing with particular attention in black subjects, Hispanics, Asians, Native Americans. Andrew L. et al. [1], on a 10-year literature review found 2,389 patients with the disease. Among these patients 50.1% were Hispanic, 17.2% of black, 15.4% of white, 8.4% of Asian, 0.3% of American and 8.7% of other races. In Taiwan, Chin-Choon Ye et al. [11], found from 2001 to 2011 1,078 patients with an annual incidence increase of 0.46 in 2001 to 4.52 in 2011 per 100,000 population. David Slattery [12], demonstrates through a literature review in Asia the presence of many cases in China, Thailand, Vietnam, India and Japan. In view of these data, it is no longer clear that Dupuytren’s disease affects all races. Since the first case reported in 1974 by Plasse in, several authors have published cases among black subjects.In 2020, Coulibaly et al. [13], reported a series of 26 Afro-descendant patients treated at the Aristide LEDANTEC hospital between 2006 and 2018. Other authors have also published cases among blacks [5-17]. None of these publications reported family cases or cases involving the hand and another body part (penis or foot). Our case comes to add to the long list of elements to clarify in Dupuytren’s disease in general, in black in particular. Our case is unique. In the literature, authors report cases that occur mainly around 50 years with an increase in incidence with age and a risk of recurrence. Our two patients are young subjects unfortunately they will risk to be operated several times for relapses. During the operation we found a long aponeurosis cord, interlaced with the pedicles and especially very adherent to the skin reflecting above all the typical shape of the white subject. The theory of local hypoxia and chronic ischemia has already been mentioned in the past by authors. One of our patients is a scuba diver by profession. He reported a decompression-type dive accident that would have triggered his illness. Only one case is small to confirm this hypothesis but probably the local hypoxia and chronic ischemia could be the cause without counted low temperature in depth. This may also explain why this case simulates the symptomatology of Dupuytren disease in the white subject.
CONCLUSION
Although it has been discovered for a very long time, Dupuytren’s disease remains very poorly known. It is even less well known among people of African descent. Until now the genetic origin in these Afro-descendants has not been reported. For the first time a genetic origin is proven. Our case was exceptional in terms of the genetic origin, the intimate adhesion of the aponeurosis cord on the skin typical of the white subject, the etiological factor (local hypoxia and chronic ischemia) and the early age of onset but also the presence of associated Ladderhose disease.
REFERENCES
- Coulibaly NF, Doumbia MM, Dembele B, Dia R, Fall MEK, Sane AD, et al. Dupuytren’s disease: A reality in Black Africa. Hand Surg Rehabil. 2020; 39: 448-453.
- Crawford J, Raykha C, Charles D, Gan BS, O’Gorman DB. WT1 expression is increased in primary fibroblasts derived from Dupuytren’s disease tissues. J Cell Commun Signal. 2015; 9: 347-352.
- Forrester HB, Temple-Smith P, Ham S, de Kretser D, Southwick G, Sprung CN. Genome-wide analysis using exon arrays demonstrates an important role for expression of extra-cellular matrix, fibrotic control and tissue remodelling genes in Dupuytren’s disease. PLoS One. 2013; 8: e59056.
- Gary MA. Santamarina. Pediatric Dupuytren’s disease: Case report and review of the literature. Ann Pediatr Surg. 2013; 9: 127-130.
- Gonzalez MH, Sobeski J, Grindel S, Chunprapaph B, Weinzweig N. Dupuytren’s disease in African-Americans. J Hand Surg Br. 1998; 23: 306-307.
- Hu FZ, Nystrom A, Ahmed A, Palmquist M, Dopico R, Mossberg I, et al. Mapping of an autosomal dominant gene for Dupuytren’s contracture to chromosome 16q in a Swedish family. Clin Genet. 2005; 68: 424- 429.
- Mella JR, Guo L, Hung V. Dupuytren’s Contracture: An evidence based review. Ann Plast Surg. 2018; 81: S97-S101.
- Michou L, Lermusiaux JL, Teyssedou JP, Bardin T, Beaudreuil J, Petit- Teixeira E. Genetics of Dupuytren’s disease. Joint Bone Spine. 2012; 79: 7-12.
- Obrecht E. Dupuytren’s disease, retrospective of a series of 56 patients and histological and epidemiological approach to risk factors for recurrence.
- Rehman S, Goodacre R, Day PJ, Bayat A, Westerhoff HV. Dupuytren’s: A systems biology disease. Arthritis Res Ther. 2011; 13: 238.
- Richard-Kadio M, Yeo S, Kossoko H, Allah CK, Assi-Dje Bi Dje V. The disease of Dupuytren. About three cases in the Black African. Chirurgie de la Main. 2008; 27: 4042.
- Shih B, Watson S, Bayat A. Whole genome and global expression profiling of Dupuytren’s disease: Systematic review of current findings and future perspectives. Ann Rheum Dis. 2012; 71: 1440- 1447.
- Sladicka MS, Benfanti P, Raab M, Becton J. Dupuytren’s contracture in the black population: A case report and review of the literature. J Hand Surg Am. 1996; 21: 898-899.
- Slattery D. Review: Dupuytren’s disease in Asia and the migration theory of Dupuytren’s disease. ANZ J Surg. 2010; 80: 495-499.
- Spyropoulou GA, Pavlidis L, Milothridis P, Zaraboukas T, Demiri E. Dupuytren in a Child: Rare Presentation of a Rare Clinical Entity. J Hand Surg Am. 2016; 41: e477-e479.
- Vega-Villanueva LR. Espinoza, Bilateral Dupuytren’s Contracture and the “Prayer’s Sign”. J Clin Rheumatol. 2021; 27: e38-e38.
- Weinstein AL, Haddock NT, Sharma S. Dupuytren’s disease in the Hispanic population: A 10-year retrospective review. Plast Reconstr Surg. 2011; 128: 1251-1256.









































































































































{kind=link}