Infected Dislocation of Metatarso Phalangeal Joint Replacement Salvage Procedure by Arthrodesis using Autograft Bone
- 1. Department of Orthopaedic Surgery, Hospital Virgen Del Mar, Spain
- 2. Department of Internal Medicine, Hospital Virgen Del Mar, Spain
Abstract
We report an unusual case of a female patient who, having been operated on by implantation of a Toefit-Plus Metatarso Phalangeal (MTP) prosthesis, suffered in the early post-operative days a deep infection produced by staphylococcus. Early treatment proved to be insufficient and thus the patient experienced a dislocation of the aforementioned prosthesis. Our management consisted in a series of surgical procedures aiming at clearing the infection. Initially, the prosthesis was removed and substituted by a gentamycin bone cement spacer. After a second look was undertaken, further debridement and implantation of a Gentamycin Beads (PMMA). When infection was completely cleared, in a final procedure arthrodesis was performed by means of a tricortical iliac crest autograft, stabilized with a mini external fixator, which was left for three months, until consolidation was proven. At follow up, the patient presented a good clinical outcome, with remission of symptoms and complete restitution of first ray length. The patient is very satisfied, presenting a normal gait and using regular footwear.
Keywords
• Metatarso phalangeal prosthesis
• Prosthesis infection
• Toefit-Plus infection
• Metatarso phalangeal arthrodesis
• Metatarso phalangeal joint replacement
• Toefit-Plus dislocation
Citation
Núñez-Samper M, Parra G, Lao E, Martialay P (2016) Infected Dislocation of Metatarso Phalangeal Joint Replacement Salvage Procedure by Arthrodesis using Autograft Bone. JSM Foot Ankle 1(3): 1014.
ABBREVIATIONS
MTP: Metatarso Phalangeal; ESR: Erytrocyte Sedimentation Rate; CRP: Protein C Reactivates; MINI-FIX: External Fixator; ROM: Range Of Movement; PMMA: Polymethacrylate
INTRODUCTION
Metatarso phalangeal prostheses were implanted for the first time in 1972 as treatment for hallux valgus and hallux rigidus. First design was reported by Swanson [1], composed by silicone and whose purpose was to serve as a spacer to keep the length and joint movement. Although early results were encouraging, long term failures lead to new designs. Currently, metatarso phalangeal prosthesis is modular; models available are diverse, some including conical components in one side, built in cobalt-chrome alloys, and a polyethylene phalangeal insert. Others are composed by two to four components (Toefit-Plus) whose attachment to bone happens through screw-in or press-fit principles.
Ceramic on ceramic models display a mushroom shaped stem at the intraosseous end of each component which eases press-fit attachment, with a concave or convex surface at the articular end depending on their distal or proximal placement respectively. There is also available a model that resembles a knee replacement implant (MTP Metis). Latest reports by, Erkokaf [2], Duncan [3], Valentini [4], Fucusi [5], Jhonson [6] , yield good results for modular, non-constrained prosthesis, with no infection or dislocations up to date, Carranza [7], nonetheless, addresses one infection and one dislocation in his series of 24 patients with the Toefit-Plus prosthesis. These dreaded complications hinge the biomechanics of the forefoot by altering Maestro´s metatarsal support and digital length formula, producing transfer metatarsalgia and a painful forefoot [8-10].
In order to clear infection, surgical treatment is mandatory, with aim at resecting the bone ends at both sides until vascularised tissue is found. This results in a significant shortening of the first ray. Definitive remnant is posteriorly evaluated in a second-look procedure [8,9]. Antibiotic treatment is needed in all case Isolated dislocation results from a breakage of the capsule-ligamentous structures that stabilize the implant, which need to be immobilised for one month after reduction [11]. Otherwise, capsular suturing is performed, also followed by immobilization. In any case, range of movement is going to be compromised.
CASE PRESENTATION
We report on a 63 year-old female patient undergoing treatment for Müller-Weiss disease and metatarsalgia due to hallux valgus-rigidus, unrelated to the talonavicular joint pathology. She underwent surgery in October 2013, when Toefit-Plus MTP prosthesis was implanted (Figure 1).
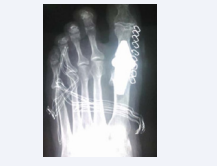
Figure 1: Immediate post-operative dorsal-plantar radiographic image of the Toefit- Plus prosthesis.
During the early post-operative period, an inflammatory picture was noticed and treated by partial wound debridement, along with Cefalosporin and Diclofenac. Partial remission took place and culture and sensitivity wasn’t performed assuming it was a superficial infection. A few months after, the inflammatory picture remained, showing the same clinical findings, spontaneous pain that it increases to the exploration, local heat and impede for the mobilization, along with progressive valgus deviation of the hallux due to prosthetic luxation (Figure 2A-2B),

Figure 2: Dorsal-plantar and lateral views of the dislocated prosthesis.
confirmed by X-ray film.
When he first attends to our Hospital in May 2015, clinical examination shows a remarkable inflammation of the forefoot and pain (Figure 3),
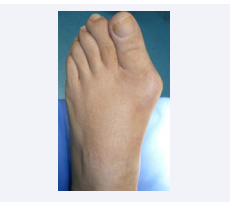
Figure 3: Valgus deformity and local swelling around the implant area.
also present on passive ROM evaluation.
Plain X-ray revealed dislocation. Nuclear medicine tests with Ga.99 and Tc.67 were highly positive (Figure 4)

Figure 4: Ga 67 gammagraphy. High uptake at distal metatarsal and proximal phalanx, marked by a black circle.
and inflammatory markers very elevated, with no elevation of the leukocyte count, all along supporting the diagnosis of chronic osteomyelitis.
In November 2015, after seeking second opinion from other colleagues, the patient returns to our Hospital seeking to commence treatment.
The prosthesis was removed (Figure 5A-5B),

Figure 5a: Dislocated prosthesis prior to removal.

Figure 5b: After implant removal, samples are taken and debridement is performed
and samples were taken for microbiology. A cement bone spacer was left in place (Figure 6A-6B),

Figure 6a: Antibiotic impregnated cement as a spacer

Figure 6b: Post-op x-ray where cement occupying medullar cavity can be seen
culture and sensitivity result came back positive for Coagulase Negative Staphilococcus, Caprae, Lugdunensis and Capitis, sensitive to Gentamicine and Ciprofloxacin, and such was the antibiotic treatment (recommended by our Internal Medicine Department), plan while for inflammatory markers were monitored. In the meantime, the patient remained on mixed antibiotic treatment at a standard dose. After two-month follow- up, ESR and CRP remain elevated, so we decided to remove the cement and take new samples for culture and sensitivity, which came back with the same results as the previous ones. The Gentamycine cement block was insufficient in order to heal the infection, probably due to the foreign body effect caused by it. At this time Gentamycin Beads (PMMA) was implanted, (Figure 7 A-C)

Figure 7a: Intraoperative image after cement removal.

Figure 7b: Implantation of Gentamycine Beads (PMMA)

Figure 7c: X-ray images
and left in place for two months.
After these two months, ESR and CRP had dropped to normal levels and so we proceeded to a reconstructive surgery, consisting in MTP arthrodesis using a block of autologous bone intramedullary, Figure (8 A-D)

Figure 8a: Intramedullar bi-polar implantation of the graft

Figure 8b: Cancellous bone graft. Set up of external fixator

Figure 8c: Check X-Ray

Figure 8d: The cancellous bone graft completely occupying the medullar canal
retrieved from the iliac crest, measuring 3, 5 cm along with cancellous bone. Stability was conferred by means of a mini external fixator (Mini-fix) Figure (8 B) allowing for progressive weight-bearing with a walking boot and crutches, during 3 months. Then, the external fixator was removed. X- Ray images were satisfactory and complete osteointegration was observed, as well as an improvement in patient clinical status so regular footwear was allowed. At six months, complete osteointegration was observed no metatarsalgia was present and a normal anteromedial load pattern was observed (Figure 9 A-D).

Figure 9a: Final clinical result at 6 months post-op. Normal foot configuration

Figure 9b: Restoration of normal forefoot

Figure 9c: Dorsal-plantar view standing X-Rays film.
.
Figure 9d: Dorsal-lateral view standing X-Rays film
The patient was already wearing her regular shoes.
Presenting AOFAS Score (Forefoot Clinical Rating System) preoperative 30 points ( Pain 20, Function 0, Shoes 5, Mobility 0, Mobility Int.- Fal. 5, Stability 0 Callus 0; Alignment 0 ) , from to 6 months, 95 points (Pain 40,Function 10, Shoes10, Mobility 0, Mobility Int-. Fal 5, Stability 5, Callus 5, Alignment 15). Important improvement in pain relief, function and alignment.
DISCUSSION
The indication criteria for first MTP joint arthroplasty must be strict and limited to primary Hallux Rigidus at stages II or III according to Regnauld’s classification [10], and no pathology affecting minor radii is present (claw toes or complex deformities), moderate or severe hallux valgus-rigidus and some patients suffering from sequels following hallux valgus surgery who maintain enough bone stock at the phalange end (>2.5 cm). Adequate bone quality and a fully competent stabilizing ligamentous system are mandatory.
Amongst complications, stiffness and loosening are the most commonly found. Infection and dislocation, nonetheless, are two serious complications rarely diagnosed. In combination, the aforementioned complications pose a very poor prognosis. Infection can appear due to poor intraoperative management or secondary to poor healing, superficial infection or skin necrosis, even with adequate antibiotic therapy.
A dislocation appears mostly when poor component positioning is present or secondary to ligamentous instability when excessive synovial debridement occurs, although infection and trauma have to be also accounted for.
In these cases, surgical intervention with removal of prosthesis and ample soft tissue and bone debridement is mandatory, resulting in many cases in a significant shortening (Gap) of the first ray that impairs anteromedial support, with subsequent transfer metatarsalgia in adjacent rays affecting 2nd and 3rd rocker stances. In order to avoid the collapse of the joint space, Myerson [11] recommends implanting a Gentamicin impregnated cement spacer until resolution of sepsis takes place. Once confirmed the latter, MTP arthrodesis after bone distraction must be undertaken, by means of a bone block and an external fixator, in order to recover the length lost during the process (staged procedure), controlling the evolution until full healing is patent, most likely at around 12 weeks. In such way, a normal minor to major ray ratio can be achieved, avoiding transfer metatarsalgia. After bibliographic review, we haven’t found results on infection and dislocation together in 1st MTP joint replacement. Although results on 1st MTP arthrodesis after distraction can be found, these are scarce (Blaut and Falliner [12], Núñez-Samper [13-15], Myerson [16], Malhotra [17], Luck [18] and Haeni [19]).
CONCLUSION
The underlying interest of this case relies on three different contexts: Firstly, it is uncommon to find a case of metatarso phalangeal dislocation due to infection by three different types of Coagulase Positive Staphylococcus, resistant to antibiotic treatment, which, despite surgical debridement, only heals after the use of Gentamycine beads (PMMA 7.5 mg. Gentamycine). Second, the procedure through which the bone and biomechanics are restored is achieved by means of an autologous bone graft, stabilized with a mini external fixator, and third, the timing for the graft implantation, making sure the infection was completely cleared, guided by blood parameters. Although the risk of pin tract infection is there, we consider it negligible compared to the risk of infection when implanting a plate in an environment where three different species of Staphilococus have grown.







































































































































{kind=link}