Endoscopic Therapy with Histoacryl for Gastric Varies
- 1. Department of Gastroenterology, Sapporo Kosei General Hospital, Japan
CITATION
Sato T (2013) Endoscopic Therapy with Histoacryl for Gastric Varies. JSM Gastroenterol Hepatol 2(1): 1007.
INTRODUCTION
Gastric variceal bleeding is a common complication, and is associated with higher morbidity and mortality rates than those seen with hemorrhage from esophageal varices [1]. Therapeutic strategies for gastric variceal bleeding include transjugular intrahepatic portosystemic shunt (TIPS), endoscopic obliterative therapy with cyanoacrylate and balloon-occluded retrograde transvenous obliteration (B-RTO). In this article, we review the treatment of gastric varices, including the clinical use of endoscopic obliterative therapy with cyanoacrylate for emergency control of acute gastric variceal bleeding classified as gastroesophageal varices type 2 (GOV2) or isolated gastric varices 1 (IGV1), based on the Sarin endoscopic classification [2].
Treatment of gastric varices by Histoacryl
Acute gastric variceal bleeding is a medical emergency requiring intensive care (Figure 1).
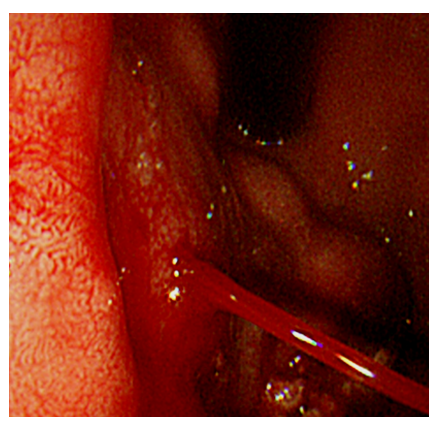
Figure 1: Acute gastric variceal bleeding
Currently, therapeutic strategies for gastric variceal bleeding include TIPS, cyanoacrylate endoscopic obliterative therapy and B-RTO, but the optimal management of bleeding gastric varices remains controversial due to a lack of randomized, controlled trial. N-butyl-2- cyanoacrylate (Histoacryl®, B.Braun Dexon GmbH Spangenberg, Germany) is a tissue glue monomer that polymerizes and solidifies instantly upon contact with blood, resulting in rapid hemostasis. Soehendra et al. were the first to report the usefulness of Histoacryl in the treatment of bleeding gastric varices, which have a high mortality rate [3]. Endoscopic obliterative therapy with Histoacryl is useful for emergency control of acute gastric variceal bleeding. It is now the first-choice treatment worldwide for the obliteration of bleeding gastric varices [4-8].
High rates of long-term rebleeding after endoscopic obliterative therapy with Histoacryl have been reported [5,7,9]. However, recent articles conclude that endoscopic obliterative therapy with Histoacryl is a highly effective modality for immediate hemostasis of gastric variceal bleeding and is associated with an acceptable rebleeding rate [10,11]. Kumar et al. reported that undiluted Histoacryl was effective in achieving initial hemostasis in case of actively bleeding gastric varices, and was very safe and not associated with embolic complications [10]. In many institutions, Histoacryl is mixed with a contrast medium, radiopaque Lipiodol®, (Guerbet Asia Pacific, Tsuen Wan, Hong Kong), to allow radiologic monitoring during and after injection. To prevent Histoacryl from solidifying too quickly, dilution with Lipiodol is necessary. Major complications of the procedure include ulceration and recurrent bleeding, although more serious complications, including embolization to the brain [12], portal vein [13], lung [14-19], and spleen [19,20] have also been reported. Risk factors for extravariceal embolization associated with Histoacryl treatment include a large injection volume, dilution of radiolucent Histoacryl with radiopaque Lipiodol, speed of injection, and the presence of shunts [18,21,22]. To avoid embolic complications as much as possible, we recommend that endoscopists aim to use the smallest volume of Histoacryl necessary for obliteration, and to use Histoacryl in the most concentrated form practicable.
Because endoscopic obliterative therapy with Histoacryl has the potential risk of serious complications, complying with the standard injection method is important to reduce the risks, and Sato et al used Histoacryl at a concentration of 70% in Lipiodol and a volume of 0.7-1.4ml per injection to minimize embolic risk [23].
CONCLUSION
Endoscopic obliterative therapy with Histoacryl is the treatment of choice for gastric variceal bleeding. By following a standard technique, this endoscopic obliterative therapy can be performed safety and effectively.









































































































































{kind=link}