Incidence of Biliary Injuries during Laparoscopic Cholecystectomy: Prevention, Recognition, Reconstruction, Outcome
- 1. Department of Surgery, Casa di Cura Bernardini, Italy
Abstract
Abstract The incidence of bile lesions after Laparoscopic Cholecystectomy (LC) remains high despite surgeons having crossed the learning curve. In fact, the data reported on bile and vascular injuries in the course of LC ranges from 0,3 to 1,4. Many of these lesions are not due to inexperience; they are the result of basic technical failure and misinterpretations.
The purpose of this work is to make a contribution, based on our experience of over 40 years, to reduce the possibility of ongoing LC injuries by improving the possibilities of their prevention as well as a timely recognition that would favor a more suitable repair with more valid results in the future.
Citation
Lacitignola S, Massafra R, Bernardini M, Fabio M, Roccasalda T (2020) Incidence of Biliary Injuries during Laparoscopic Cholecystectomy: Prevention, Recognition, Reconstruction, Outcome. JSM Gastroenterol Hepatol 7(1): 1096.
INTRODUCTION
Open cholecystectomy (OC) was the standard practice for the treatment of symptomatic gallbladder disease until the 1980s. At present, 90% of cholecystectomies are performed by laparoscopy which is one of the most common surgical procedures in the world. Unfortunately, the widespread application of laparoscopic cholecystectomy (LC) has led to a concurrent rise in the incidence of major bile duct injuries (BDIs) which are most complicated than after OC.
In fact, while many reports have cited an increased use of LC [1] at the same time BDIs increased drammatically [2]. It was shown that laparoscopic approach is associated with a twofold increase in the risk of bile duct injuries compared to open cholecystectomy (0,1%-0,2%) [3] And additionally these injuries were comparatively more severe [4]. The reported incidence of BDI varies from 0,3% to 1,4% resulting in a significant impact on quality of life (QoL), overall survival and frequent medico-legal liabilities [5].
Despite a declining trend in BDI rate (032%-052%) there was no change in the morbidity and mortality [6] because the factors predisposing to BDI are related to anatomy, disease related pathology, structural misidentification and improper techniques [7,8].
The aim of this work is to assess, on the basis of our experience, the possibility of technical measures to not only reduce the percentage of complications but also promote their prevention, their recognition, their correction for a better quality of life and finally their results.
ETIOLOGY AND PATHOGENESIS OF LAPAROSCO- PIC BILE DUCT INJURIES (LBDI)
The most feared complication of one of the greatest advances in biliary surgery in this century is laparoscopic cholecystectomy, in fact although most surgeons passed through the learning curve and reached “steady-state”, there has been no significant improvement in the incidence of BDI during the operations. Although most injuries may be repaired by conversion to an open procedure, the end-stage of biliary injury may result in disaster (Table 1). There are many factors to consider when treating a patient with a bile duct injury or benign biliary stricture. The majority of these patients are young (40-50 years), female, have a long life expectancy and are in the most productive years of their life. Because of this, it is essential that these patients have prompt recognition of their problems and a reliable treatment with a long-term success rate. Unlike malignant strictures, treatment durability is an essential factor in determining treatment success for benign biliary strictures.
LC has largely replaced OC for the management of gallstone disease. In addition, not only are laparoscopic BDI following LC more prevalent than following OC [9], but their clinical presentation is different. The symptoms of patients with laparoscopic BDI are usually vaguer than those following OC. Thus, it is important to be able to recognize these symptoms and initiate an appropriate evaluation and treatment plan. Three factors increase the morbidity associated with the treatment of these injuries: delay in diagnoses, extended length of treatment and treatment failure.
Traditionally, biliary strictures have been classified using the Bismuth classification but since LC has become the standard treatment for symptomatic gallstones, LBDIs now comprise the majority of biliary injuries. In our experience we have noticed that these injuries occur differently from injuries associated with OC, and the classification of these injuries can aid in their diagnoses and treatment. We have found that there are many patterns of laparoscopic BDI and these are shown in Figure 1.
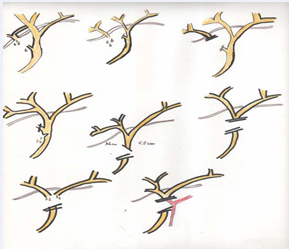
Figure 1:Patterns of laparoscopic BDI.
This classification not only complements the Bismuth classification but corresponds to the mechanism of the injury which can aid in efforts to prevent these injuries.
Table 1: The End-Stage of Biliary Injury.
| Years of morbidity |
| Shortened life expectancy |
| Repeated episodes of sepsis |
| Biliary cirrhosis |
| Portal ipertension |
| Varicele bleeding |
| Liver transplantation |
| and even |
| Death |
MECHANISM OF INJURY
Table 2.
Table 2: Mechanism of Injury.
| Lack of experience |
| Failure to recognize the structures of Calot’s triangle |
| Local risk factors |
| Factors inherent to laparoscopic technique |
| Reluctance to convert to an open procedure |
lists the mechanism of laparoscopic BDI. The lack of experience may lead to either confusing CBD with the cystic duct or making an incision too close to CBD in case of intraoperative cholangiography Figure 2.
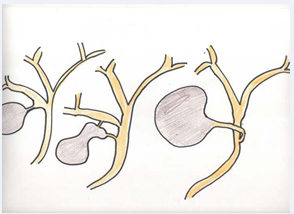
Figure 2 The lack of experience may lead to either confusing CBD with the cystic duct.
Calot’s triangle is the area where the injury is carried out and the angle of the lesionis formed by the cystic duct and the bile duct Figure 3(a-b).
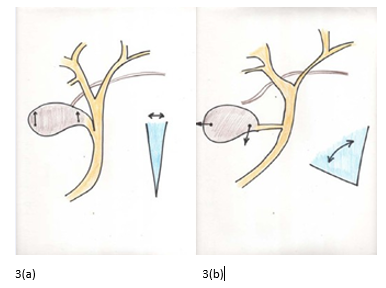
Figure 3a Calot’s triangle is the area where the injury is carried out and the angle of the lesionis formed by the cystic duct and the bile duct.(b) Anatomic anomalies of the cystic duct entry.
These injuries are recognized during the procedure in about 70% of cases, otherwise the patient will present abdominal pain and abdominal distension with high values of alkaline phosphate and bilirubin.
The local risk factors create a prolonged operative time and a higher likelihood of conversion to an open procedure. A number of parameters have been evaluated to predict such difficulty [10]. Male gender and higher age have been found to be consistent predictors of a difficult procedure in both acute colecystitis and elective cases [11].
In cases with acute cholecystitis, the severity of inflammation in the triangle and adjoining area remains the most common reason for conversion and in cases with chronic cholecystitis, presence of thick wall gallbladder, presence of Mirizzi syndrome, scleral-atrophic gallbladder and impacted large stone at neck are important predictors of a difficult procedure.
The local risk factors (Table 3)
Table 3: Local Risk Factors.
|
Severe, acute or chronic inflammation in infundibulum |
|
Contracted gallbladder |
|
Impacted cystic duct stone |
|
Tense distended gallbladder |
|
Morbid obesity with excess fat in porta |
|
Short cystic duct |
|
Large, dilated cystic duct |
|
Excessive bleeding |
|
Anatomic anomalies of cystic duct entry |
include anatomic anomalies of the cystic duct entry which we consider very important in the determination of biliary tract complications Figure 3(a-b). The same applies to factors inherent to laparoscopic technique such as lack of depth perception, use of electro cautery and limited field easily obscured by blood. No less important is the reluctance to an open procedure and according to my personal experience I recommend observing what I call the “rule of numbers” (Table 4)
Table 4: Rule of Numbers.
|
Rule nr.1 : usually just one cystic duct |
|
Rule nr.2 : there may be more than one cystic artery |
|
Rule nr.3 : the third cystic artery is the right hepatic |
|
artery or duct |
|
Rule nr.6 : if more than six clips to control |
|
a case are required> open |
|
Rule nr.10: If no progress is made in ten minutes > open |
in the attempt to carry out a safe operation.
RECOGNITION AND RECONSTRUCTION
Several features during the dissection of gallbladder might indicate a possible bile duct injury. The Intraoperative Cholangiography (IOC), which I use routinely [12], can often prevent a serious injury to the common bile duct, that is, it can limit the damage thus avoiding more serious injury. Since the review of literature [13] documents that most surgeons are inclined to selective IOC, it becomes essential to perform it correctly, thus avoiding further complications to existing ones. Figure 4
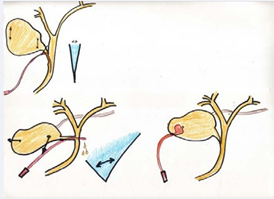
Figure 4: Execution of the procedure in relation to the degree of Calot’s triangle.
shows the correct execution of the procedure in relation to the degree of Calot’s triangle. Therefore, the higher this will be, the easier it will be to introduce the catheter into the cystic duct. Otherwise it is preferable to use the transcholecystic pathway. Once the cholangiogram is done, it is possible that the proximal hepatic ducts are excluded and this indicates that the cholangiocatheter is in the common bile duct rather than in the cystic duct. Failure to recognize it at this point would result in a transection of the common duct, in other words in a more serious complication.
In considering Stransberg’s classification which in my opinion is more comprehensive and easier to understand, this comes to be a very useful tool to decide the best method for each type of injury according to its etiological mechanism. In fact, A-type lesions which are difficult to prevent, can be treated endoscopically quite easily as the aim is to reduce pressure inside the bile ducts. Since this type of injury is quite common in tertiary hospitals where there may not be an operative endoscopy, it is advisable to insert a T-tube into the bile duct and transfer the patient to a specialized center [14].
If the injury caused concerns to a section of a segmentary bile duct or its ligature (tipo B), the treatment can be two-fold, that is conservative if the patient is symptom-free even in the presence of elevation of liver function tests. Otherwise in the presence of cholangitis, it will be appropriate to drain the occluded liver segment through percutaneous drainage or surgical resection in case of a cholangitis rebel to medical treatment.
Another possible injury is to dissect a right accessory liver duct that is not detected during surgery resulting in bile loss. In this case the endoscopy cannot play a role and therefore it will be necessary to drain the eventual bile collection to avoid peritonitis resulting in septic shock. It is possible that the leak will close spontaneously without the need for further intervention, otherwise surgical treatment will be as in A-type injuries.
A less common injury than the previous ones is a lesion on the left or right side wall of the common duct without a loss of tissue (D-type). This can be done by a false identification of structures for intense flogosis. The repair can be carried out during surgery with a 5-0 suture, but exclusively by associating an endoscopic sphincterotomy and placing bile prosthesis. In this case it is very important to be sure that you have not also associated a vascular injury. This would complicate the healing process of the lesion, which would always be treated as described by resorting to surgery as a last choice.
E-type lesions are the most severe because there is a loss of tissue of the common liver duct and almost always they occur on the level with the bifurcation. These injuries are frequently associated with vascular section which mainly concerns the right hepatic artery. Unlike the liver, bile ducts are supplied only by arteries [15]. The transverse marginal artery, also called “comunicating arcade” (Figure 5)
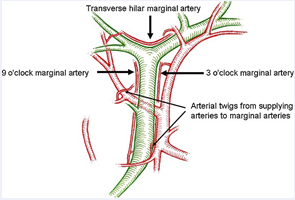
Figure 5: The transverse marginal artery, also called “comunicating arcade”.
works as an arterial shunt between the two sides of the liver and is of great importance in understanding how high biliary injuries contribute to liver ischaemia.
However, it should be acknowledged that the major disadvantage of the Stransberg classification is that it does not include any additional vascular involvement at all. For this reason, the Stransberg classification could not demonstrate a significant association between the discrimination of specific injury patterns and vascular duct injuries that were included in Stewart-Way classification.
In addition to the value of IOC that should always be performed in case of a biliary injury during cholecystectomy, there are two other factors that contribute to the surgical success rate: surgical technique and surgical experience.
The most feared of all complications during LC is a major injury to the hepatic or common bile ducts. The mechanisms often responsible for such a catastrophic event include undue traction on the neck of the gallbladder, attempts to control bleeding by aninaccurate placement of clamps and failure to fully dissect Calot’s triangle. Excessive traction on the fundus can elevate the junction of the cystic and hepatic ducts so that when the surgeon divides what is thought to be the cystic duct, in actuality a portion of the hepatic/common duct is resected (Figure 6).
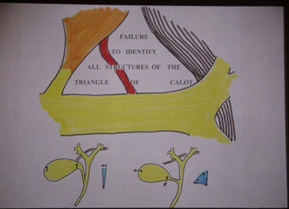
Figure 6: Excessive traction on the fundus can elevate the junction of the cystic and hepatic ducts.
Bleeding in the portahepatis is usually from the cystic artery or portal vein. Regardlessness and anxiety, combined with a desire to quickly control the bleeding, can turn an inconvenient situation into a nightmare. In the face of hemorrhage, an imprecisely applied clamp can crush or severely damage the bile duct. Recognizing the range of anatomic relationships that can exist in the liver hilium makes thorough dissection of Calot’s triangle an absolute prerequisite for the safe performance of cholecystectomy.
When the common duct or hepatic duct has been divided and there is sufficient length to perform an end-to-end anastomosis without tension, this is considered to be an option by many. In our experience, we have noticed, just like other surgeons have [16-17], a high failure rate of this repair even by surgeons who are specialized in biliary surgery. The reason for this high failure rate is related to ischemia and tension. Indeed, the blood supply of the common duct is axial running at 3:00 and 9:00 on the duct (Figure 5) and these arteries have been called “communicating arcade” by creating an arterial shunt between the two sides of the liver and it is of great importance in understanding how high biliary injuries contribute to hepatic ischaemia. To all this must be added that most of the blood supply comes from below contributing to ischaemia in the proximal portion of the duct.
Roux-en-Y hepaticojejunostomy has the best success rate for the repair of a transection or resection injury of the common duct or common hepatic duct. For years, however, expecially in young patients, we have preferred to use this technique with a simple modification such as Hutson-Russel’s loop (Figure 7);
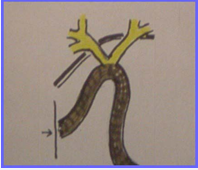
Figure 7: Simple modification such as Hutson-Russel’s loop.
we have also allowed the combination of surgery, radiology and endoscopy to improve the medical management for biliodigestive anastomosis treatment avoiding new surgery.
PERSONAL OUTCOME
We have retrospectively reviewed the medical records in the last 20 years of our experience of all patients who had a reconstruction of the bile ducts during laparoscopic cholecystectomy performed both at our institution and at other hospitals. The total number of patients treated was 141, of which 37 were our patients and had an immediate reconstruction thanks to intraoperative diagnosis of injury during laparoscopic cholecystectomy. The remaining 104 patients were re-operated after undergoing a previous surgery at other institutions. The results are shown in the table 5.
CONCLUSION
Iatrogenic biliary injury is a devastating complication of laparoscopic cholecystectomy and a growing issue in malpractice claims. Misidentification of the bile ducts is the leading cause of biliary injury. To avoid this, a critical view of safety technique should be employed with utmost care. If the biliary injury is identified intraoperatively, reconstruction should only be undertaken by experienced hepatobiliary surgeons following an operative cholangiogram. In the post-operative period, any deviation from the expected clinical course of recovery should alert the surgeon to suspect biliary injury and take a proactive approach to diagnosis and proper management. Although we have discussed about types, incidence and mechanism of injury as well as presentation, recognition and repair, the key to this problem is prevention.









































































































































{kind=link}